











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Nodular hidradenoma, first described by Mayer in 1941, is a benign adnexal neoplasm with eccrine or apocrine differentiation that occurs in middle-aged adults, mainly women, and with a controversial prevalence in the literature1-3. Clinically, it manifests as a solid or cystic nodule, normochromic to erythematous, with a smooth surface, slow and endophytic growing, and with rare cases of exophytic growing. The most common affected locations are the scalp, face, trunk, and proximal extremities1. At dermoscopy, the pattern consisting of a homogeneous bluish area that occupies the entire lesion, associated with vascular structures and white dots, is the most common pattern4. The unusual presentation, mimicking a nodular basal cell carcinoma (BCC) and the importance of the correct approach to atypical lesions motivated this report.
Clinical case
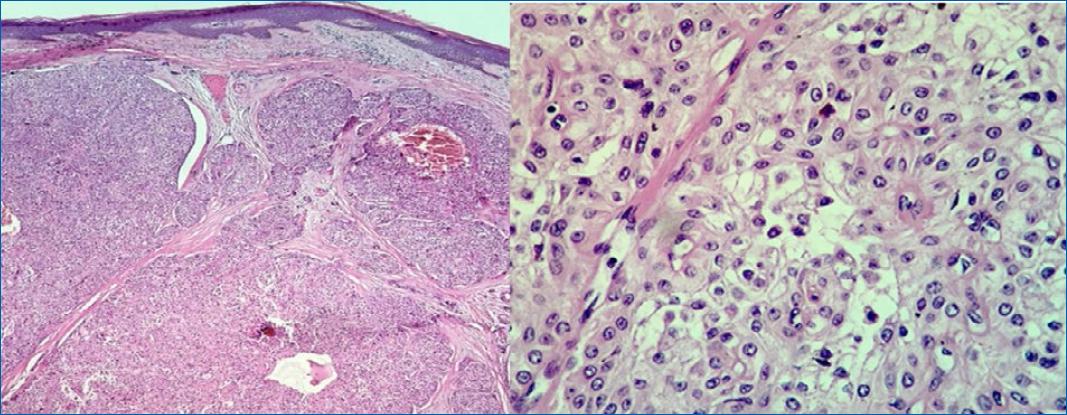
A 40-year-old female patient, phototype III, complained of a “lump” in her right forearm for a year and a half. Dermatological examination revealed a hyperchromic, erythematous, and sessile nodule (2.5 × 2 cm) of firm consistency and with points of ulceration (Figure 1). History of initial growth and subsequent stabilization, mild pain on manipulation. The diagnostic hypotheses of nodular BCC, dermatofibrosarcoma protuberans, amelanotic melanoma, Merkel cell carcinoma, and adnexal tumors were considered. On dermoscopy, the presence of structures similar to blue-gray globules, arboriform telangiectasias with some thickened vessels, bright white spots, and points of microulceration (Figure 2). An excisional biopsy was performed and the material was sent for histopathological and immunohistochemical examination. Histopathology showed nodular adnexal epithelial neoplasia without atypia, with a focal connection to the epidermis and a clear cell component, and characteristics suggestive of nodular hidradenoma (Figure 3); confirmed by immunohistochemistry with positivity for p63, epithelial membrane antigen (EMA), and cytokeratin AE1/AE3. The patient remains under follow-up with a good surgical scar aspect and no recurrence.


Discussion
Nodular hidradenoma is a benign adnexal neoplasm with eccrine or apocrine differentiation that occurs in middle-aged adults, mainly women1,2, as observed in this case. The exophytic clinical presentation is rare, however, described in the literature.1
There is considerable confusion in the literature regarding the appropriate nodular hidradenoma designation, and it has already been called clear cell hidradenoma, cystic nodule hidradenoma, clear cell myoepithelioma, and eccrine acrospiroma. This reflects different approaches among authors regarding its histological characteristics and histogenesis1,3.
The histopathology of nodular hidradenoma is characterized by the presence of a well-circumscribed but not encapsulated tumor. It presents a typical biphasic cell pattern, with polyhedral cells with eosinophilic cytoplasm and large cells with abundant clear cytoplasm and a small nucleus. There is a variable proportion between cell types, but clear cells predominate in one-third of cases1,2, as seen in this case. Immunohistochemistry shows reactivity for p63, EMA, and cytokeratin AE1/AE25, also observed in this case.
Classically, the differential diagnosis includes other adnexal tumors, being clinically indistinguishable1. Basal cell carcinoma (BCC) (ulcerated forms) as a differential diagnosis of hidradenoma nodular is rarely cited in the literature6.
Curative treatment consists of surgical excision, but the possibility of recurrence exists. Malignant transformation is rare1.
The present report registers an unusual presentation of a nodular hidradenoma, with hyperchromic, ulcerated, and exophytic manifestations, simulating a nodular BCC in the clinical aspect but mainly dermoscopically. We emphasize the importance of the correct approach to atypical lesions by the dermatologist, as well as the fundamental role of complementary exams (histopathology/immunohistochemistry) in the conclusive diagnosis of this case.

