











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
As a common clinical disease, stroke can lead to diffe-rent degrees of dysphagia and cough reflex impairment. It has been reported that 37%-74% of patients with acute stroke had dysphagia: among them 14% have aspiration pneumonia (AP),1-3being this a major cause of increased risk of mortality and dependency, resulting in higher health costs.4-6
Some risk factors like more severe strokes such as the ones with impairment of consciousness, older age, and frailty before stroke are associated with dysphagia as well as with AP.1,4,6-7Specifically, the poorer scores of performance quantified by modified-Rankin Scale (mRS) and the higher severity of stroke quantified by National Institutes of Health Stroke Scale (NIHSS) are positively correlated to the development of dysphagia and aspiration pneumonia.1,5,8-11
The aim of this study is to analyze the relationship between aspiration pneumonia and the type and severity of ischemic stroke (according to Bamford Stroke Classification (BSC) and NIHSS), the degree of dysphagia (quantified by the Gugging Swallowing Screen (GUSS)), and patients’ functional status (mRS and Barthel scale). Simultaneously, it was to compare the length of hospitalization and rate of mortality of stroke patients who develop aspiration pneumonia with the ones who do not.
Material and Methods
The retrospective database analysis includes all patients (n = 1116) admitted with acute stroke between 1st January 2017 and 31st December 2019 to the stroke unit of Centro Hospitalar de Trás-os-Montes e Alto Douro, Portugal, being excluded the ones with haemorrhagic stroke (n = 179). The transient ischemic attacks are not included in this database, nor analyzed in our study. The diagnosis of stroke was based on clinical presentation and brain imaging, either cerebral computed tomography or magnetic resonance.
Two groups of stroke patients were compared: patients with and without aspiration pneumonia; in two different times during the hospital admission: at the time of admission and at the hospital discharge. All patients admitted to this unit have an evaluation made by a doctor regarding the functional status by quantifying the modified-Rankin Scale (mRS) and Barthel scale; and concerning the severity of the stroke, considering clinical and imaging elements, defining the ischemic stroke according to Bamford Stroke Classification in total, partial or lacunar anterior circulation infarctions (TACI, PACI, LACI, respectively), and posterior circulation infarctions (POCI) and quantifying the National Institutes of Health Stroke Scale. Considering the severity of the stroke, we used the categories of mild (NIHSS 0-4), mildmoderate (NIHSS 5-15), moderate-severe (NIHSS 16-20), and severe (NIHSS 21-42). The degree of impairment of functional status was categorized as null (mRS 0-1, Barthel 100), mild (mRS 2, Barthel 75-99), moderate (mRS 3-4, Barthel 50-74), and severe (mRS 5, Barthel 0-49). The functional evaluation and the one regarding the severity of the stroke are repeated when the patient is discharged from the stroke unit. As well as part of the initial evaluation, a specialized rehabilitation nurse performs the Gugging Swallowing Screen (GUSS), which is validated as bedside screening instrument to identify acute stroke patients at risk of aspiration and dysphagia,1,2enabling the quantification of null (GUSS= 20), mild (GUSS 15-19), moderate (GUSS 10-14) and severe dysphagia (GUSS 0-9).
Aspiration pneumonia diagnosis was based on clinical symptoms and signs (cough, purulent respiratory secretions, respiratory distress, fever, rales, bronchial breath sounds), com-bined with laboratory and imaging findings (elevation of inflam-matory markers, lobar or segment opacification on X-ray), and in some cases microbiological isolation in patients’ sputum.
Statistical analysis was made using Microsoft Excel™ and SPSS™. Descriptive statistical analysis was made, using absolute values and frequencies. The continuous normally distributed variables were identified by kurtosis and skewness measurement, and characterized by average and standard deviation, and being compared using T-test. The Chisquare test and Fisher test were used to evaluate association or independency of categorical variables, the latter when the first could not be applied. The significance levels used were p<0.01 and p<0.05.
Results
DEMOGRAPHIC DATA OF THE RECRUITED POPULATION
During the three years analyzed in the study, there were 937 patients admitted with ischemic stroke in our unit, 32% (n = 301) in 2017, 35% (n = 328) in 2018 and 33% (n = 308) in 2019.
The studied population showed a gender distribution of 51.5% (n = 483) male patients, with an average age of 75.6 years old (standard deviation (SD) 12.76 years old). The youngest patient was 19 years old, while the oldest was 101 years old.
The mortality rate within all ischemic stroke patients was 11.6% (n = 109), and the length of stay was in average 11.0 days (SD 9.44 days).
STROKE CLINICAL CLASSIFICATION AND STRATIFICA-TION OF SEVERITY
Clinically and according to Bamford Stroke Classifi-cation, there was an overall larger frequency of TACI with 39.3% (n = 368), followed by LACI with 22.6% (n = 212), POCI with 19.7% (n = 185) and PACI with 18.4% (n = 172). However, considering the severity according to NIHSS, we found larger frequencies of mild to moderate (NIHSS 5-15) and mild strokes (NIHSS 0-5), with 37.4% and 36.5%, respectively.
FUNCTIONAL STATUS
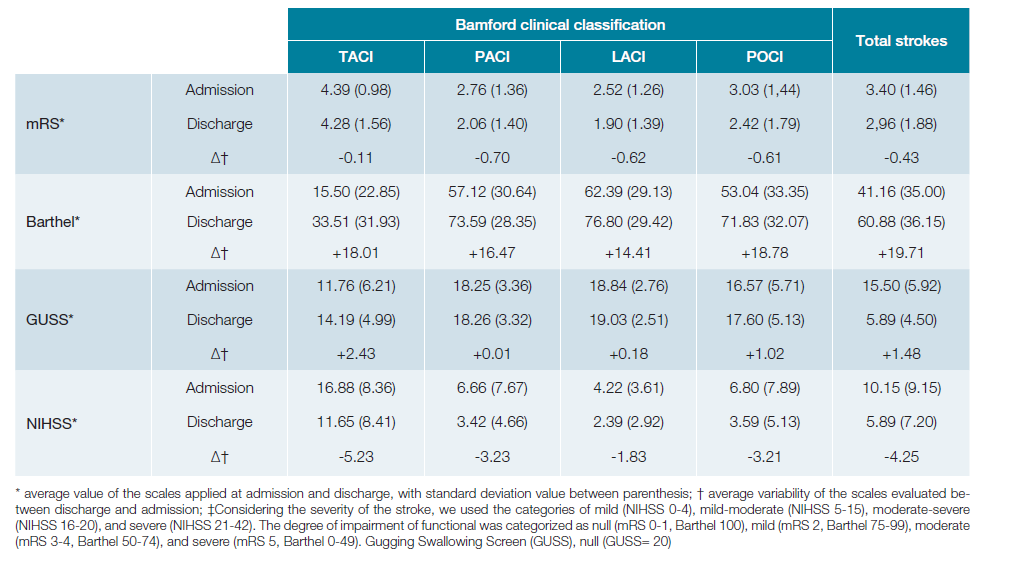
Comparing the scales evaluated at admission and at di-charge, we found that in the overall population there was an amelioration of all functional scales, with an average improvement of -0.43 points in the modified Rankin scale, greater in the PACI subgroup (-0.7 points); and +19.71 points in Barthel scale, with a larger improvement in the POCI subgroup (+18.78 points). Considering the dysphagia grades, we found an overall average improvement of +1.48 points, with greater impact in the TACI subgroup (+2.43 points), and lesser enhancement of GUSS in PACI subgroup.
The variability of functional scales, dysphagia grade, and severity of stroke through hospital admission, according to Bamford Clinical classification is demonstrated in Table 1.
ASPIRATION PNEUMONIA
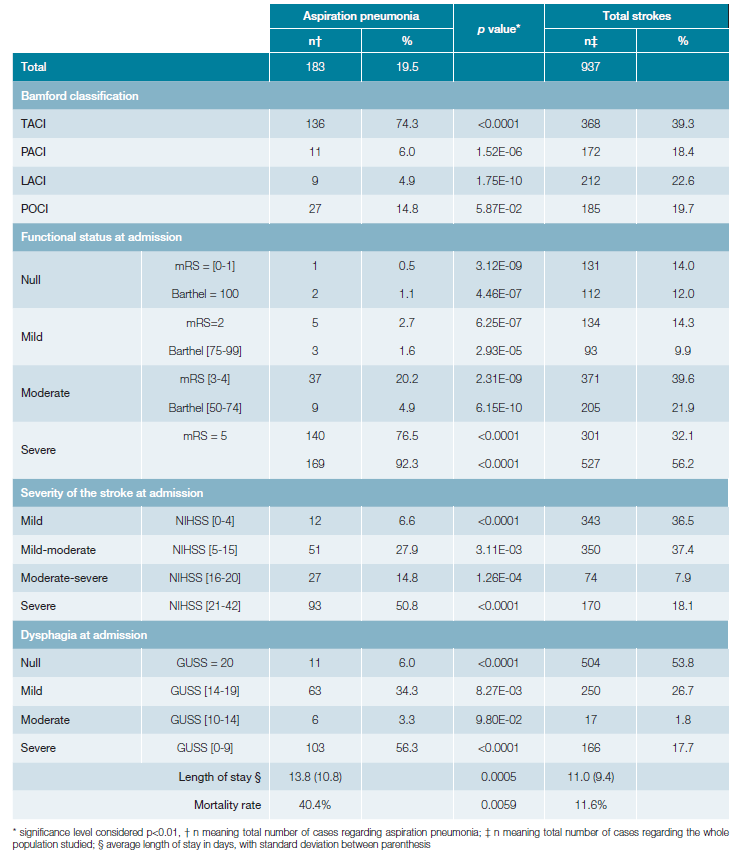
The overall incidence of aspiration pneumonia was 19.5% (n = 183). We found a higher prevalence in the TACI subgroup with 74.3% of aspiration pneumonias (n = 136), followed by POCI with 14.8% (n = 27).
According to the functional status, there were more aspiration pneumonia in the mRS severe impairment group (mRS=5) with 76.5% (n = 140) patients, and in the Barthel’s severe impairment group (Barthel [0-49]), with 92.3% (n = 169) patients having aspiration pneumonia.
Considering the severity of the stroke, we found a higher prevalence of aspiration pneumonia with severe stroke, classified by NIHSS higher than 20 points, with 50.8% (n = 93) patients, followed by the mild-moderate severity group with 27.9% (n = 51).
The group with severe dysphagia with GUSS less than 9 points was the one with higher prevalence of aspiration pneumonia with 56.3% (n = 103) cases, followed by the ones with mild dysphagia (GUSS between 14 and 19), with 34.3% (n =63) cases.
Considering the outcome of the aspiration pneumonia pa-tients, we found a mortality rate of 40.4% representing 67.9% of overall deaths, and a length of hospitalization of 13.8 days (SD 10.8 days), with statistical significance when compared to the overall population.
The relationship between stroke clinical classification, functional status at admission, dysphagia grade, and aspiration pneumonia is revealed in Table 2.
Discussion and Conclusion
Dysphagia is a frequent consequence of stroke, reaching a 74% prevalence in some studies, being its active and early search related to lesser aspiration pneumonia and complication rates.1-2Aspiration pneumonia is one of the more serious consequences of poststroke dysphagia, affecting up to onethird of acute stroke patients in some studies,12 involving almost 20% of our stroke population. As we showed in our study, where dysphagia is present in 46.1% of stroke patients, the group with the lowest GUSS scores, classified with severe dysphagia, was the one with higher rates of aspiration pneumonia. However, we found that the second highest frequency of AP was in the group with mild dysphagia (GUSS 14-19). That can be explained by the fact that mild dysphagia may go unnoticed until complications arise, coupled with the fact that our dysphagia evaluation occurs only when the patient is already on the stroke unit, after a variable period of stay in the emergency department. This makes us conclude, in line with the literature,2,4,8,9,12,13that the sooner dysphagia is assessed, the higher chance physicians have to identify patients with dysphagia, with higher risk of aspiration pneumonia.
In the available literature, it is established that the cough reflex depends not only on medullary reflex pathways, but also on cortical facilitatory pathways, with known association between dysphagia and severe stroke according to NIHSS, supratentorial and TACI strokes.5-7,9-11,14In agreement with the published literature, there was a higher AP prevalence with statistical significance in the TACI group. However, considering the severity of the stroke, we not only found a higher prevalence of aspiration pneumonia with severe stroke, classified by NIHSS higher than 20 points, with 50.8% (n = 93) patients, but also in the mild-moderate severity group with 27.9% (n = 51). Even though that was not evaluated in our study, we believe that this high prevalence of AP in mildmoderate stroke reflects the effect of thrombolysis and thrombectomy in TACI patients, with consi-derable improvement of neurological deficits and a consequent decrease in NIHSS at the time of stroke unit admission, without decreasing the pre-treatment risk of aspiration.
Stroke patients with better functional indices are less likely to have dysphagia and to develop aspiration pneumonia.1,4,6,8,15According to the functional status, our study revealed that severe functional impairment (mRS=5 and Barthel = [0-49]) was related to AP with statistical significance. That agrees with the severity of the stroke that we found in the aspiration pneumonia group.
The development of aspiration pneumonia in stroke populations increases their complications and mortality rates, as well as the length of hospitalization and health costs.2,4-6,10,12,15,16In agreement with the literature, we found that pa-tients who evolved with aspiration pneumonia had a 2.8 days longer length of hospital stay, compared to the overall population (13.8 days vs 11.0 days). On the same page, the mortality rate of aspiration pneumonia was 28.8% higher than the overall stroke population (40.4% vs 11.6%), being in this series the most frequent cause of death.
The great strength of this study is the size of the data pool that it complies, with more than 1000 patients admitted in just three years, as well as the objective data ascribed by functional scales applied both at admission and discharge of the patients. However, there are several limitations. First, the retrospective nature of the study compromises the diagnostical evaluation of aspiration pneumonia, which is based on clinical records, and some laboratorial findings, not always being the timeline of development of this entity clearly defined. On the other hand, patients submitted to thrombolysis or thrombectomy should be categorized, but as the latter procedure is not made in our institution, we decided to exclude it, because of the lack of other institutions’ clinical records, and the possible bias inherent.
Concluding, aspiration pneumonia is related to the severity of the stroke, the consequent impact on functional status, and the grade of dysphagia, being linked to higher mortality rates and longest length of stay. The early dysphagia assessment with simple clinical tools is imperative to define patients with unexpected aspiration hazards, to promote early detection and aspiration pneumonia prevention.
ACKNOWLEDGEMENTS
The authors thank the Neurology Department Director, Dr. Mário Rui Silva, and the Internal Medicine Director at the time of the study design, Drª. Paula Vaz Marques for the support.

