










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.26 no.3 Lisboa jun. 2019
https://doi.org/10.1159/000489720
IMAGES IN GASTROENTEROLOGY AND HEPATOLOGY
Fish Bone Penetrating into the Head of Pancreas in a Patient with Billroth II Gastrojejunostomy
Espinha de Peixe a Penetrar na Cabeça do Pâncreas num Doente com Gastrojejunostomia do Tipo Bilroth II
Tan Attila, Zeynel Mungan
Division of Gastroenterology and Hepatology, Koc University School of Medicine, Istanbul, Turkey; Division of Gastroenterology and Hepatology, American Hospital, Istanbul, Turkey
* Corresponding author.
Keywords: Pancreas, Endoscopy, Foreign body
Palavras-Chave: Pâncreas, Endoscopia, Corpo estranho
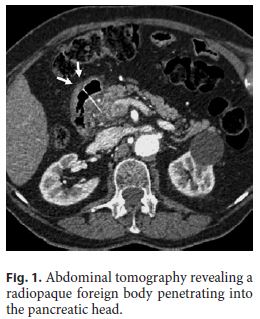
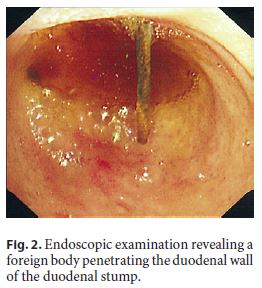
A 76-year-old male patient with a history of abdominal aortic aneurysm repair and Billroth II gastrojejunostomy (25 years ago) for refractory peptic ulcer disease presented with gradually worsening epigastric pain over the past 48 h, without any associated fever. Physical examination was significant for epigastric discomfort. A complete blood count, liver function tests, and C-reactive protein were within normal limits. Pancreatic enzyme levels were not available. The day after admission, an upper endoscopy (GIF H260; Olympus, Tokyo, Japan) revealed changes consistent with Billroth II gastrojejunostomy. The gastric remnant, distal afferent loop, and efferent loop mucosa appeared normal. An abdominal computerized tomography demonstrated a radiopaque foreign body penetrating into the pancreatic head, with the proximal portion partially residing in the duodenal lumen (Fig. 1). The patient acknowledged eating turbot fish 2 days prior to the onset of abdominal pain. In an attempt for endoscopic removal of the foreign body, the afferent enteral loop was deeply intubated with a therapeutic upper endoscope (GIF 2T 240; Olympus). The foreign body penetrating the duodenal wall (Fig. 2) was noted at the duodenal stump. The distal end of the fish bone was captured with a polypectomy snare and was removed in 1 piece. The snare’s plastic sheath was left 2–3 cm distal to the tip of the endoscope to allow alignment of the fish bone’s long axis with the axis of the lumen and the endoscope. Since the appropriate alignment was successfully achieved, an overtubeovertube was not used. The fish bone was removed from the lower and upper esophageal sphincters without any mucosal penetration and damage. The removed foreign body was 3.5 cm in length and consistent with a turbot bone (Fig. 3). The patient’s pain improved following removal of the fish bone penetrating the head of pancreas.

Foreign body ingestion occurs commonly. The majority of foreign bodies pass through the gastrointestinal tract spontaneously. Rarely, ingestion of a sharp-pointed object such as a fish bone may potentially pierce the gastrointestinal wall and cause complications such as abscess formation in adjacent structures [1–3]. Patients are usually unable to provide a clear history of fish bone ingestion. Imaging may provide valuable information, especially in patients with a surgically altered anatomy as in our case. Early recognition may allow endoscopic removal of the penetrated fish bone in 1 piece and prevent further complications that may require surgical interventions. This case is unique because a fish bone migration in retrograde fashion into the afferent loop of Billroth II surgery and penetration into the pancreas through the duodenal stump has not previously been reported. It is extremely important to have an alignment of long, pointed objects with the axis of the lumen and endoscope to avoid iatrogenic mucosal damage and foreign body penetration into the gastrointestinal wall. If needed, an overtube or soft latex protector hood should be used to prevent iatrogenic injury during the removal of a foreign body.
References
1 Horii K, Yamazaki O, Matsuyama M, et al: Successful treatment of a hepatic abscess that formed secondary to fish bone penetration by percutaneous transhepatic removal of the foreign body: report of a case. Surg Today 1999;29:922–926. [ Links ]
2 Yasuda T, Kawamura S, Shimada E, Okumura S: Fish bone penetration of the duodenum extending into the pancreas: report of a case. Surg Today 2010;40:676–678. [ Links ]
3 Gharib SD, Berger DL, Choy G, Huck AE: Case records of the Massachusetts General Hospital. Case 21–2015. A 37-year-old American man living in Vietnam, with fever and bacteremia. N Engl J Med 2015;373:174–183. [ Links ]
Statement of Ethics
This study did not require informed consent or review/approval by the appropriate ethics committee.
Disclosure Statement
The authors have no conflicts of interest to declare.
* Corresponding author.
Dr. Tan Attila
Division of Gastroenterology and Hepatology, American Hospital
Guzelbahce Sokak, No 20
TR–34365 Istanbul (Turkey)
E-Mail tanattila2003@yahoo.com
Received: January 31, 2018; Accepted after revision: April 27, 2018

