











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkAn 80-year-old male patient underwent endoscopic retrograde cholangiopancreatography (ERCP) due to moderate cholestasis (bilirubin 2.3 mg/dL) and bile duct dilation >12 mm as well as cholecystolithiasis on abdominal ultrasound. After difficult biliary access including transpancreatic sphincterotomy and pancreatic duct stenting, cholangiography indicated prepapillary impaction of a large stone >15 mm, defying basket capture for mechanical lithotripsy. The patient was referred for cholecystectomy after implantation of a 10-Fr, 11-cm biliary plastic stent. Of note, the cholecystectomy had to be converted to open surgery due to marked adhesions, but the postoperative course was otherwise uncomplicated. The postoperative ERCP 4 weeks later indicated persistent stone impaction in the prepapillary segment not to be extracted by conventional techniques (Fig. 1a). Of note, faint contrast extravasation from the cystic duct (CD) was noted, consistent with clinically well-compensated CD leakage, such that repeat bile duct stenting was performed. Single-operator digital cholangioscopy using the Spyglass DS platform (Boston Scientific) to guide electrohydraulic lithotripsy (EHL) was scheduled and performed without complications 6 weeks later (Fig. 1b). EHL fragments were removed and no remnant stones were detected. However, the initial and dedicated cholangiography replicated a cloud of contrast extravasation correlating to persistent CD leakage despite >8 weeks of biliary plastic stenting (Fig. 1c). Following this, the CD branch-off was selectively intubated (Fig. 1d), and the small underlying defect was visualized by cholangioscopy (Fig. 1e; online suppl. Video, for all online suppl. material, see www.karger.com/doi/10.1159/000516949) and fluoroscopy [1]. Due to ongoing CD leakage despite plastic stenting for >10 weeks and taking the small-volume fistula into consideration, the patient underwent implantation of a fully covered self-expanding metal stent as a mature and easy-to-implement rescue approach in this setting (Fig. 1f) [2]. Repeat ERCP after 3 months, including balloon occlusion cholangiography, demonstrated no persistent leakage or remnant stones (Fig. 1g).
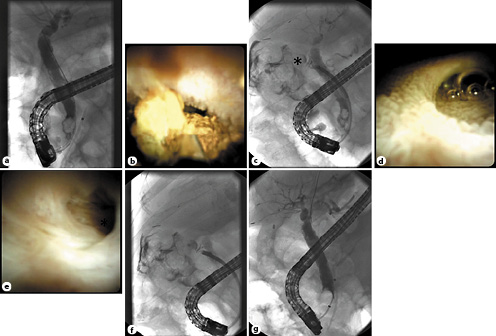
Fig. 1 a Cholangiography illustrates prepapillary impaction of a large stone >15 mm (note pancreatic duct was stent left in place due to the ongoing stone impaction and rescheduled ERCP). b Digital single-operator cholangioscopy-guided electrohydraulic lithotripsy during the third ERCP session. c Contrast media extravasation after injection into the cystic duct (CD) branch-off (d) which is also visible on cholangioscopy. e Direct endoscopic vision of a small-volume fistula at the CD’s blind end underlying the CD leakage as confirmed on fluoroscopy (f). g After a 3-month interval with fully covered, self-expanding metal stenting, balloon-occlusion cholangiography excluded persistent leakage and/or remnant stones (note repeat pancreatic stenting due to inadvertent pancreatic cannulation and minor contrast injection)

