










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkAnálise Psicológica
versão impressa ISSN 0870-8231
Aná. Psicológica vol.33 no.3 Lisboa set. 2015
https://doi.org/10.14417/ap.975
The prevalence of personality disorders in Portuguese male prison inmates: Implications for penitentiary treatment
Nélio Brazão1, Carolina da Motta1, Daniel Rijo1, José Pinto-Gouveia1
1CINEICC – Centro de Investigação do Núcleo de Estudos e Intervenção Cognitivo-Comportamental, Faculdade de Psicologia e de Ciências da Educação da Universidade de Coimbra
ABSTRACT
Prison inmates are known to be a population with a high prevalence of mental disorders. Most of these disorders are chronic and difficult to treat, particularly in what concerns Cluster B Personality Disorders, which prevalence in forensic samples are even higher than in the general population. This study assesses the prevalence of Personality Disorders in a sample of 294 Portuguese male prison inmates, interviewed with the Structured Clinical Interview for DSM-IV Axis II Personality Disorders (SCID-II). The results showed a global prevalence rate of 79.9%, with 42.8% of the participants diagnosed with Antisocial Personality Disorder as the main diagnosis. Paranoid, Passive-Aggressive, Borderline, and Narcissistic Personality Disorders were the most common comorbid diagnosis associated with Antisocial Personality Disorder. These results strongly suggest that Personality Disorders should be taken into account when deciding and planning the intervention inside prison.
Key-words: Prevalence, Personality disorders, Male prison inmates, Penitentiary treatment.
RESUMO
A população reclusa é conhecida pela elevada prevalência de perturbações mentais, muitas delas crónicas e difíceis de tratar, sobretudo no que se refere às Perturbações da Personalidade do Grupo B, cuja prevalência em contextos forenses é superior à observada na população geral. Este estudo avaliou a prevalência das Perturbações da Personalidade numa amostra de 294 reclusos Portugueses do sexo masculino. Os participantes foram avaliados com a Entrevista Clínica Estruturada para as Perturbações da Personalidade do Eixo II do DSM-IV (SCID-II). Os resultados mostraram uma elevada prevalência global de 79.9%, sendo que a Perturbação de Personalidade Anti-Social foi identificada em 42.8% dos participantes como o diagnóstico principal. As Perturbações de Personalidade Paranóide, Passivo-Agressiva, Borderline e Narcísica foram os diagnósticos comórbidos mais frequentemente associados à Perturbação de Personalidade Anti-Social. Estes resultados sugerem que a patologia da personalidade é uma variável que deve ser tida em conta na decisão e na definição da intervenção em contexto de reclusão.
Palavras-chave: Prevalência, Perturbações da personalidade, Reclusos do sexo masculino, Tratamento penitenciário.
Introduction
Personality Disorders are severe forms of a psychological disturbance affecting 9.1% of the general population (American Psychiatric Association, 2013). Data from the 2001-2002 US Epidemiologic Survey on Alcohol and Related Conditions suggests that approximately 15% of adults have at least one Personality Disorder. Over the past decades, interest in offender’s mental health has increased enormously and a considerable amount of research has focused on the prevalence rates of Personality Disorders in prison inmates. Nonetheless, no prevalence studies have been carried out in Portuguese prisons to assess offender’s psychopathology rates and mental health intervention needs.
International studies have shown that the prevalence rate of Personality Disorders among incarcerated individuals is high, reaching up to 80% (Black et al., 2007; de Ruiter & Trestman, 2006; Fazel & Danesh, 2002; Roberts & Coid, 2010; Teplin, 1994). As expected, the most prevalent DSM diagnosis among prison inmates is Antisocial Personality Disorder, with prevalence rates between 46 and 84% (Coid, 2002; Fazel & Danesh, 2002; Kjelberg et al., 2006). Other Cluster B Disorders, especially Borderline Personality Disorder, are also prevalent in prison inmates (Black et al., 2007; Coid, 2002; Coid, Kahtan, Gault, & Jarman, 1999; de Ruiter & Trestman, 2006; Johnson et al., 2000; Sansone & Sansone, 2009; Teplin, 1994; Warren et al., 2002).
The association between Personality Disorders and violent offenses is widely known and reported in several studies (Duggan & Howard, 2009; Gilbert & Daffern, 2011; Roberts & Coid, 2010; Short, Lennox, Stevenson, Senior, & Shaw, 2012; Warren & South, 2009; Yu, Geddes, & Fazel, 2012). Research with clinical and forensic samples has found that Personality Disorders are predictors of violent behavior (e.g., Hiscoke, Långström, Ottosson, & Grann, 2003; Thornton, Graham-Kevan, & Archer, 2010). Nonetheless, some Personality Disorders are more strongly associated than others with violent behavior, namely Antisocial and Borderline Personality Disorders, the only two of the ten listed in the DSM-5 (APA, 2013), which explicitly includes diagnostic criteria addressing aggression. In a study by Gandhi and colleagues (2001), subjects diagnosed with Antisocial and/or Borderline Personality Disorder presented more violent and criminal behavior after discharge from a psychiatric hospital. Longitudinal research also suggests that antisocial and impulsive personality features are substantial risk factors for criminal recidivism among adult offenders in the criminal justice system (Hiscoke et al., 2003; Warren et al., 2002).
Another related and relevant issue is that the incarcerated population presents complex problems and high rates of psychiatric comorbidity. Teplin (1994) found that, although 50% of 728 male inmates were diagnosed with Antisocial Personality Disorder, 30% still presented severe mental disorders and high rates of substance abuse/dependence after excluding Antisocial Personality Disorder. Hiscoke and colleagues (2003) observed a similar tendency, with 51% of 168 inmates fulfilling criteria for at least one Cluster A Personality Disorder, 43% for at least one Cluster B Personality Disorder, and 49% for one or more Cluster C Personality Disorder. Multiple diagnoses were the rule rather than the exception: 74% of participants were diagnosed with more than one Personality Disorder, with subjects meeting criteria for at least two Personality Disorders.
The importance of DSM Personality Disorders for the assessment of risk for violent behavior is emphasized in current clinical recommendations and checklists (Kropp, Hart, Webster, & Eaves, 1995; Tardiff, 2001; Webster, Douglas, Eaves, & Hart, 1997). However, it is still unclear to what extent mental disorders are acknowledged and recognized by prison health care services. In prisons, abnormal behavior is often tolerated or perceived as a disciplinary problem, often dealt with punitively, while the “quietly mad” are ignored (Birmingham, Mason, & Grubin, 1996). Consequently, the opportunity to treat and rehabilitate personality-disordered individuals is often lost as a consequence of the lack of effective screening procedures or failure to provide an adequate intervention to inmate’s mental health problems (Birmingham et al., 1996; Woolf, 2006). Current rehabilitation procedures and case management practices in Portuguese prisons are primarily aimed to increase educational and professional qualifications; there is no standardized screening for Personality Disorders or psychotherapeutic interventions available in prisons nationwide. Until now, no systematic evaluation or screening of Personality Disorders was carried out in Portuguese prisons. This study’s main goal was, therefore, to determine the prevalence rates of Personality Disorders in male prison inmates through a structured clinical interview for Personality Disorders.
Method
Participants
Participants in this study were male prison inmates from 11 Portuguese prisons, with a minimum age of 18 years old and, at least, with elementary education. Participants were recruited within a wider research project with the purpose of testing the efficacy of a cognitive-behavioral program (GPS – Growing Pro-Social; Rijo et al., 2007) for adult offenders. Due to the nature of this program, the selection of participants obeyed a set of exclusion criteria: (1) presence of cognitive impairment (given that the GPS program is not suitable for the cognitively-impaired) or psychotic disorders (experiential strategies used in GPS are contraindicated for psychotic patients); (2) active substance use (cessation or at least substantial reduction of drug or alcohol use must precede the GPS treatment); and (3) being sentenced exclusively for sexual offenses (sex offenders would benefit from more specific intervention programs).
Female prison inmates were also excluded from the sample because women represent less than 6% of the total prisoners, and any possible idiosyncrasies from this cohort would be underrepresented. In order to allow a period of adjustment to the prison environment and to avoid any evaluation bias from incarceration stress, all participants were assessed with a minimum interval of one month after prison intake.
A sample of 330 male prison inmates (30 for each prison) who did not meet the exclusion criteria was randomly selected. Following this selection, 36 (11%) inmates declined to participate. A total of 294 (89%) inmates were then assessed with a structured clinical interview for Personality Disorders (for a description of the interview, see the Measure section).
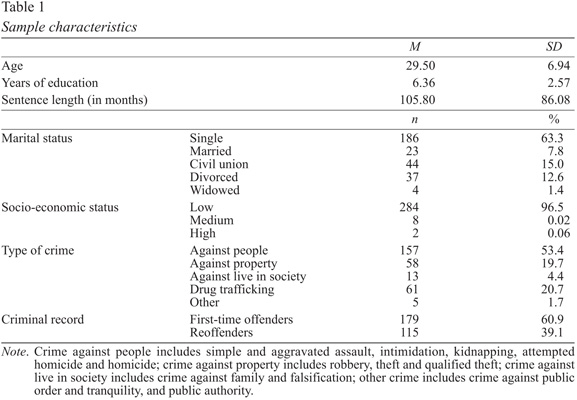
Table 1 presents the main demographic and legal features of the sample. Participants were between 18 and 55 years old, mostly single, with a low socioeconomic status, and with elementary education. The length of the sentence ranged between 7 and 867 months, with an average of 105.80 months (approximately 9 years), and most participants were first-time offenders. Crimes were predominantly against people, followed by drug-related offences and crimes against property.
Measure
Participants were interviewed with the SCID-II – Structured Clinical Interview for DSM-IV Axis II Personality Disorders (First, Gibbon, Spitzer, Williams, & Benjamim, 1997; Portuguese version by Pinto-Gouveia, Matos, Rijo, Castilho, & Salvador, unpublished), a widely known semi-structured diagnostic interview which assesses 10 Axis II Personality Disorders from the DSMIV (APA, 2000), and the Depressive and Passive-Aggressive Personality Disorders (included in DSM-IV’s appendix). It can be used to diagnose Axis II Disorders categorically (present or absent) and dimensionally (according to the number of criteria met for each diagnosis) and is considered the “gold standard” for Personality Disorders diagnosis. The SCID-II also provides a summary with a pathology profile of scores over the assessed Personality Disorders, allowing the interviewer to decide which disorder should be the major focus of clinical attention (main diagnosis).
Procedures
This study was approved by the Head of of the General Directorship of Social Reinsertion and Prison Services of the Portuguese Ministry of Justice. Data was collected between 2012 and 2014, and was carried out by three clinical psychologists of the national prison system who had special training in the diagnosis of Personality Disorders, and by the authors of this paper who had previous experience administering the SCID-II interview. The goals of the research were explained and inmates were invited to participate voluntarily. All participants signed an Informed Consent Form prior to the administration of the interview. All participants responded fully to the SCID-II interview. Personality Disorders prevalence rates were then analyzed categorically (i.e., participants met all criteria for a given personality disorder) and prevalence rates were calculated with a 95% Confidence Interval using PASW (Predictive Analytics Software), version 20 (SPSS, Chicago, IL, USA).
Results
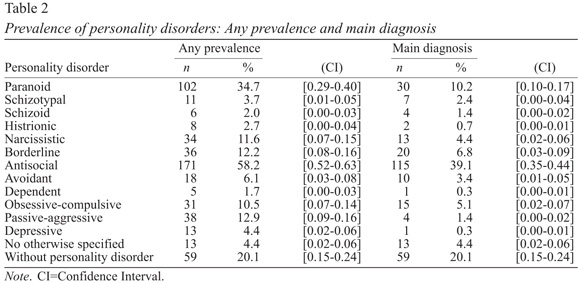
Results showed a very high prevalence of Personality Disorders, with 79.9% of the participants fulfilling criteria for, at least, one Personality Disorder. Only 20.1% of the participants did not meet enough criteria for any Personality Disorder. The prevalence rates and the frequency used to classify each Personality Disorder as the main diagnosis are reported in Table 2. The most frequently diagnosed Personality Disorders as the main diagnosis were Antisocial and Paranoid Personality Disorders, with prevalence rates of 39.1% and 10.2%, respectively. Although not accounted as the main diagnosis, Passive-Aggressive, Borderline, Narcissistic and Obsessive-Compulsive Personality Disorders were also prevalent.
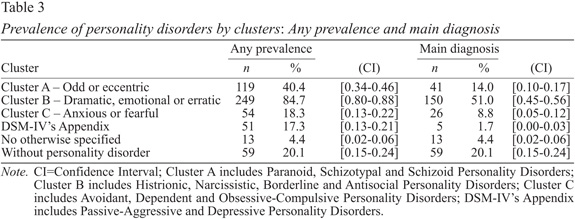
As presented in Table 3, current prevalence rates showed that Cluster B Personality Disorders were the most prevalent (with Antisocial and Borderline Personality Disorders as the more frequent diagnosis), followed by Cluster A Disorders (mainly due to the high rates of Paranoid Personality Disorder).
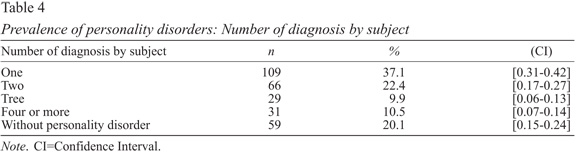
The number of Personality Disorders diagnosed was explored to account for comorbidity rates (see Table 4). Multiple diagnoses were frequent, with 42.8% of participants meeting enough criteria for two or more Personality Disorder diagnosis simultaneously.
Additionally, first-time offenders were compared with re-offenders for the main diagnosis and number of diagnoses. Concerning the main diagnosis, no significant differences were found between sub-groups (χ2=11.352; p=.571): the most frequently main diagnosis was Antisocial Personality Disorder in both sub-groups (35.6% in first-time offenders and 45.5% in reoffenders). In both sub-groups comorbidity rates was high (39.0% of first-time offenders met criteria for two or more Personality Disorders and 45.5% of reoffenders met criteria for more than one Personality Disorder) and no significant differences were observed (χ2=9.162; p=.240).
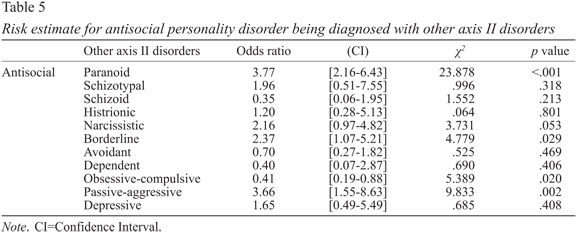
Because a high prevalence of Antisocial Personality Disorder was observed, chi-square tests with odds ratio was computed to assess the risk of antisocial individuals being diagnosed with other Axis II Disorders (see Table 5). There was a significant high risk of co-occurrence of Antisocial and Paranoid, Borderline, and Passive-Aggressive Personality Disorders. Antisocial and Narcissistic Personality Disorder odds ratio was high, but did not reach statistical significance. Obsessive-Compulsive Personality Disorder presented a significant low risk of co-occurrence with Antisocial Personality Disorder.
Discussion
Despite the international data available on the high prevalence of Personality Disorders in offenders, no systematic evaluation or screening of Personality Disorders was carried out in Portuguese prisons. This study’s main goal was, therefore, to assess the prevalence rates of Personality Disorders in a sample of male prison inmates, in order to identify the mental health intervention needs of this population.
Results showed that 80% of male prison inmates had a full-blown Personality Disorder, and more than half of the participants met the criteria for Antisocial Personality Disorder. Approximately half of the participants presented comorbid Personality Disorders, with 10% of the sample meeting sufficient criteria to be diagnosed with four or more Personality Disorders. Results also showed that the majority of participants met criteria for Antisocial and Paranoid Personality Disorder as the main diagnosis, similarly to what has been observed in studies from different countries (de Ruiter & Trestman, 2006; Fazel & Danesh, 2002; Teplin, 1994).
Almost half of the crimes, by which participants from this sample were sentenced to prison, were crimes against people, which is in accordance with studies showing an association of violence and aggressive behavior with Cluster A and B Disorders (Coid, 2002; Johnson et al., 2000; Roberts & Coid, 2010; Warren et al., 2002; Warren & South, 2009). Borderline, Passive-Aggressive, Narcissistic, and Obsessive-Compulsive Personality Disorders were the most frequently diagnosed disorders, after Antisocial and Paranoid Personality Disorders, which is also in line with previous findings (Black et al., 2007; Coid et al., 1999). This further emphasizes that most inmates present highly complex treatment needs and should receive mental health care from specially trained staff (Steadman, Osher, Clark-Robbins, Case, & Samuels, 2009).
When studying the association between Antisocial Personality Disorder and other Axis II Disorders, antisocial inmates were over three times more likely to have a Paranoid and/or Passive-Aggressive Personality Disorder. The odds of having a Borderline Personality Disorder were twice as high in antisocial inmates. Although under the significance threshold, Narcissistic Personality Disorder is also often diagnosed in antisocial inmates. According to DSM-5 (APA, 2013), these disorders share features relating to dysfunctional interpersonal patterns characterized by lack of empathy and connection with others, intolerance to criticism, anger and counterattacking, low impulse control and emotional instability, which makes this set of personality traits very common in most inmates.
Participants suffering from Obsessive-Compulsive Personality Disorder were those less likely to be diagnosed with Antisocial Personality Disorder. Taking into account that the main feature of Antisocial Personality Disorder is a pattern of violation and disregard for the rights of others, and Obsessive-Compulsive Personality Disorder relates to hyperconsciousness, excessive scrupulousness, mental and interpersonal control, and high moral or ethical standards (APA, 2013), a higher comorbidity between these two Personality Disorders would be unlikely and, thus, unexpected.
This is the first study on the prevalence of Personality Disorders in Portuguese male prison inmates, using a structured clinical interview for Personality Disorders. The use of structured interviews over self-report measures presented several advantages, such as allowing the assessment of maladaptive patterns that may not be recognized or endorsed in self-report measures due to their egosyntonic nature. Furthermore, interviews allow Personality Disorders to be assessed both categorically (disorders are either present or absent) and dimensionally (number of criteria that an individual meets for a given disorder). Structured interview formats can also make the assessment procedures more standardized, guiding the evaluation of the criteria needed to assign a particular diagnosis and preventing interpersonal biases from different interviewers or from professionals with different theoretical backgrounds.
While a considerable amount of studies focused on samples of convenience or on individuals already referred as having mental health problems (Penner, Roesch, & Viljoen, 2011), the sample of the current study was randomly selected. However, one major limitation of this study was closely related to the sample exclusion criteria. Since subjects were attending a cognitive-behavioral program, which is contraindicated for individuals with active substance abuse or sentenced exclusively for sexual offences, inmates presenting these features were not assessed for Personality Disorders. Nonetheless, the co-occurrence of substance abuse/dependence and personality pathology is common and important (Grella, Grenwell, Prendergast, Sacks, & Melnick, 2008; Zlotnick et al., 2008), and the rates of Personality Disorders in sex offenders is high (e.g., Schroeder, Iffland, Hill, Berner, & Briken, 2013). Female offenders were also excluded from this study (due to the low number of female offenders in Portuguese prisons). Thus, further research should assess the prevalence of Personality Disorders in these three sub-groups: inmates with substance abuse/dependence, sexual offenders and female inmates. The relationship between Axis I and Axis II diagnosis in prison inmates, as well as the link between Personality Disorders, violent behavior, adjustment/disciplinary infractions and recidivism should also be tested.
The effect of incarceration in previously existing personality disorder traits should be explored as well, assessing whether the prison environment maintains or exacerbates traits or pre-existing disorders. As a controlling environment aimed primarily at security, in which adaptation to prison culture may overlap and reinforce symptom-like patterns, prison environment could possibly act as a confounding variable, and may increase the frequency of symptoms relating to suspiciousness, social withdrawal and/or interpersonal hostility (Rotter, Way, Steinbacher, Sawyer, & Smith, 2002).
Considering the high prevalence rates of Personality Disorders associated with more serious and violent offences, penitentiary services should provide systematic and effective screening procedures for proper assessment of Personality Disorders at prison intake (Birmingham et al., 1996; Black et al., 2007; Roberts & Coid, 2010; Watzke, Ulrich, Marneros, 2006; Woolf, 2006). The high prevalence of Personality Disorders and comorbidity rates in incarcerated men represents a highly significant level of clinical and functional impairment, which may cause disruption within and beyond prison settings, having a significant impact on all the domains of the individual’s life (Black et al., 2007; Gilbert & Daffern, 2011). High levels of emotional and behavioral dysregulation presented by most personality-disordered inmates may compromise adhesion to penitentiary treatment. It is then justifiable that treatment of Personality Disorders should be addressed in forensic case management procedures as a focus of intervention.
Forensic mental health professionals should be prepared and available to respond to the complex needs presented by most subjects in contact with the justice system (Brooke, Taylor, Gunn, & Madden, 1996; Fazel & Danesh, 2002). The developments in effective therapies for Personality Disorders (Bernstein, Arntz, & Vos, 2007; Farrell, Shaw, & Webber, 2009; Nadort et al., 2009; van Asselt et al., 2008) suggest that psychotherapeutic interventions reducing factors underlying antisocial behavior should be a key area of investment when dealing with personality-disordered inmates (Gilbert & Daffern, 2011; Kjelsberg et al., 2006). Similarly to what is done in the case of substance dependence/abuse, differential treatment for subjects with severe personality pathology should be provided to ensure adequate treatment and rehabilitation. All of these implications are relevant for first-time offenders and reoffenders, due to the high prevalence of Personality Disorders observed in both sub-groups.
Overall, our findings pointed out the need to take into account specific mental health intervention needs in adult offenders when deciding and planning the forensic intervention. It also stressed the importance of proper screening procedures of Personality Disorders at prison intake, as well as the need for psychotherapeutic interventions specifically focused in the reduction of dysfunctional personality traits, which may contribute to a better interpersonal adjustment during inmates’ imprisonment and after release.
References
American Psychiatric Association (APA). (2000). Diagnostic and statistical manual of mental disorders (DSM-IV). Washington, DC: American Psychiatric Association. [ Links ]
American Psychiatric Association (APA). (2013). Diagnostic and statistical manual of mental disorders (DSM-5). Washington, DC: American Psychiatric Association. [ Links ]
Bernstein, D., Arntz, A., & Vos, M. (2007). Schema focused therapy in forensic settings: Theoretical model and recommendations for best clinical practice. International Journal of Forensic Mental Health, 6, 169-183. doi: 10.1080/14999013.2007.10471261 [ Links ]
Birmingham, L., Mason, D., & Grubin, D. (1996). Prevalence of mental disorder in remand prisoners: Consecutive case study. British Medical Journal, 313, 1521-1524. doi: 10.1136/bmj.313.7071.1521 [ Links ]
Black, D. W., Gunter, T., Allen, J., Blum, N., Arndt, S., Wenman, G., & Sieleni, B. (2007). Borderline personality disorder in male and female offenders newly committed to prison. Comprehensive Psychiatry, 48, 400-405. doi: 10.1016/j.comppsych.2007.04.0 06 [ Links ]
Brooke, D., Taylor, C., Gunn, J., & Maden, A. (1996). Point prevalence of mental disorder in unconvicted male prisoners in England and Wales. British Medical Journal, 313, 1524-1527. Retrieved from http://europepmc.org/backend/ptpmcrender.fcgi?accid=PMC2353052&blobtype=pdf [ Links ]
Coid, J. W. (2002). Personality disorders in prisoners and their motivation for dangerous and disruptive behaviour. Criminal Behavior and Mental Health, 12, 209-226. Retrieved from http://onlinelibrary.wiley.com/doi/10.1002/cbm.497/pdf [ Links ]
Coid, J., Kahtan, N., Gault, S., & Jarman, S. (1999). Patients with personality disorder admitted to secure forensic psychiatry services. British Journal of Psychiatry, 175, 528-36. doi: 10.1192/bjp.175.6.528 [ Links ]
de Ruiter, C. D., & Trestman, R. L. (2006). Prevalence and treatment of personality disorders in Dutch forensic mental health services. Journal of the American Academy of Psychiatry and the Law, 35, 92-97. Retrieved from http://www.jaapl.org/content/35/1/92.full.pdf+html [ Links ]
Duggan, C., & Howard, R. (2009). The ‘functional link’ between personality disorder and violence: A critical appraisal. In M. McMurran & R. Howard (Eds.), Personality, personality disorder, and violence: An evidence based approach (pp. 19-37). New York: Wiley-Blackweel.
Farrell, J. M., Shaw, I. A., & Webber, M. A. (2009). A schema-focused approach to group psychotherapy for outpatients with borderline personality disorder: A randomized clinical trial. Journal of Behavior Therapy and Experimental Psychiatry, 40, 317-328. doi: 10.1016/j.jbtep.2009.01.002 [ Links ]
Fazel, S., & Danesh, J. (2002). Serious mental disorder in 23000 prisoners: A systematic review of 62 surveys. Lancet, 359, 545-550. doi: 10.1016/S0140-6736(02)07740-1 [ Links ]
First, M. B., Gibbon, M., Spitzer, R. L., Williams, J. B. W., & Benjamin, L. S. (1997). Structured Clinical Interview for DSM-IV Axis II Personality Disorders (SCID-II). Washington, DC: American Psychiatric Press, Inc. [Portuguese version by J. Pinto Gouveia, A. P. Matos, D. Rijo, P. Castilho, & M. C. Salvador, 1999].
Gandhi, N., Tyrer, P., Evans, K., McGee, A., Lamont, A., & Harrison-Read, P. (2001). A randomized controlled trial of community-oriented and hospital-oriented care of discharged psychiatric patients. Influence of personality disorder on police contacts. Journal of Personality Disorders, 15, 94-102. doi: 10.1521/pedi.15.1.94.18644 [ Links ]
Gilbert, F., & Daffern, M. (2011). Illuminating the relationship between personality disorder and violence: Contributions of the General Aggression Model. Psychology of Violence, 1, 230-244. doi: 10.1037/a0024089 [ Links ]
Grella, C. E., Greenwell, L., Prendergast, M., Sacks, S., & Melnick, G. (2008). Diagnostic profiles of offenders in substance abuse treatment programs. Behavioral Sciences & the Law, 26, 369-388. doi: 10.1002/bsl.825 [ Links ]
Hiscoke, U. L., Långström, N., Ottosson, H., & Grann, M. (2003). Self-reported personality traits and disorders (DSM-IV) and risk of criminal recidivism: A prospective study. Journal of Personality Disorders, 17, 293-305. doi: 10.1521/pedi.17.4.293.23966 [ Links ]
Johnson, J., Cohen, P., Smailes, E., Kasen, S., Oldham, J., Skodol, A., & Brook, J. (2000). Adolescent personality disorders associated with violence and criminal behaviour during adolescence and early adulthood. American Journal of Psychiatry, 157, 1406-1412. doi: 10.1176/appi.ajp.157.9.1406 [ Links ]
Kjelsberg, E., Harting, P., Bowitz, H., Kuisma, I., Norbech, P., Rustad, A., . . . Vik, T. (2006). Mental health consultations in a prison population: A descriptive study. BMC Psychiatry, 6, 1-9. doi: 10.1186/1471-244X-6-27 [ Links ]
Kropp, P. R., Hart, S. D., Webster, C. D., & Eaves, D. (1995). Manual for the spousal assault risk assessment guide. Vancouver, BC, Canada: The British Columbia Institute on Family Violence. [ Links ]
Nadort, M., Arntz, A., Smit, J. H., Giesen-Bloo, J., Eikelenboom, M., Spinhoven, P., . . . van Dyck, R. (2009). Implementation of outpatient schema therapy for borderline personality disorder with versus without crisis support by the therapist outside office hours: A randomized trial. Behavior Research and Therapy, 47, 961-973. doi: 10.1016/j.brat.2009.07.013 [ Links ]
Penner, E., Roesch, R., & Viljoen, J. (2011). Young offenders in custody: An international comparison of mental health services. International Journal of Forensic Mental Health, 10, 215-232. doi: 10.1080/14999013.2011.598427 [ Links ]
Rijo, D., Sousa, M. N., Lopes, J., Pereira, J., Vasconcelos, J., Mendonça, M. C., . . . Massa, S. (2007). Gerar Percursos Sociais: Programa de prevenção e reabilitação para jovens com comportamento social desviante [Growing Pro-Social: Prevention and rehabilitation program for youths with deviant social behavior]. Ponta Delgada: EQUAL. [ Links ]
Roberts, A., & Coid, J. (2010). Personality disorder and offending behaviour: Findings from the national survey of male prisoners in England and Wales. Journal of Forensic Psychiatry & Psychology, 21, 221-237. doi: 10.1080/14789940903303811 [ Links ]
Rotter, M., Way, B., Steinbacher, M., Sawyer, D., & Smith, H. (2002). Personality disorders in prison: Aren’t they all antisocial?. Psychiatric Quarterly, 73, 337-349. Retrieved from http://link.springer.com/article/10.1023%2FA%3A1020468117930
Sansone, R. A., & Sansone, L. A. (2009). Borderline personality and criminality. Psychiatry, 6, 16-20. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2790397/ [ Links ]
Schroeder, M., Iffland, J. S., Hill, A., Berner, W., & Briken, P. (2013). Personality disorders in men with sexual and violent criminal offenses histories. Journal of Personality Disorders, 27, 519-530. doi: 10.1521/pedi_2012_26_050 [ Links ]
Short, V., Lennox, C., Stevenson, C., Senior, J., & Shaw, J. (2012). Mental illness, personality disorder and violence: A scoping review. Manchester: Offender Health Research Network. [ Links ]
Steadman, A. J., Osher, F. C., Clark-Robbins, P., Case, B., & Samuels, S. (2009). Prevalence of serious mental illness among jail inmates. Psychiatric Services, 60, 761-765. doi: 10.1176/ps.2009.60.6.761 [ Links ]
Tardiff, K. (2001). Axis II disorders and dangerousness. In G. F. Pinard & L. Paganini (Eds.), Clinical assessment of dangerousness: Emprical contributions (pp. 103-120). New York: Cambridge University Press. [ Links ]
Teplin, L. (1994). Psychiatric and substance abuse disorders among male urban jail detainees. American Journal of Public Health, 84, 290-293. doi: 10.2105/AJPH.84.2.290 [ Links ]
Thornton, A. J. V., Graham-Kevan, N., & Archer, J. (2010). Adaptive and maladaptive personality traits as predictors of violent and nonviolent offending behavior in men and women. Aggressive Behavior, 36, 177-186. doi: 10.1002/ab.20340 [ Links ]
van Asselt, A. D., Dirksen, C. D., Arntz, A., Giesen-Bloo, J. H., van Dijk, R., Spinhoven, P., . . . Severens, J. L. (2008). Outpatient psychotherapy for borderline personality disorder: Cost-effectiveness of schema-focused therapy versus transference-focused therapy. British Journal of Psychiatry, 192, 450-457. doi: 10.1192/bjp.bp.106.033597 [ Links ]
Warren, J. I., Burnette, M., South, S. C., Chauhan, P., Bale, R., & Friend, R. (2002). Personality disorders and violence among female prison inmates. The Journal of the American Academy of Psychiatry and the Law, 30, 502-509. Retrieved from http://www.jaapl.org/content/30/4/502.full.pdf [ Links ]
Warren, J. I., & South, S. C. (2009). A symptom level examination of the relationship between cluster B personality disorders and patterns of criminality and violence in women. International Journal of Law and Psychiatry, 32, 10-17. doi: 10.1016/j.ijlp.2008.11.005 [ Links ]
Watzke, S., Ulrich, S., & Marneros, A. (2006). Gender- and violence-related prevalence of mental disorders in prisoners. European Archives of Psychiatry and Neurosciences, 256, 414-421. doi: 10.1007/s00406-006-0656-4 [ Links ]
Webster, C. D., Douglas, K. S., Eaves, D., & Hart, S. D. (1997). HCR-20. Assessing risk for violence. Version 2. Vancouver, BC, Canada: Simon Fraser University, Mental Health, Law and Police Institute. [ Links ]
Wolf, N. (2006). Intervenção em saúde mental para pessoas com comportamento anti-social: 10 pontos de interface. [Mental health intervention for individuals with antisocial behavior: 10 point of interface] (D. Rijo, Trans.). In A. C. Fonseca, M. Simões, M. C. T. Simões, & M. S. Pinho (Eds.), Psicologia Forense (pp. 559-582). Coimbra: Nova Almedina. [ Links ]
Yu, R., Geddes, J. R., & Fazel, S. (2012). Personality disorders, violence and antisocial behavior: A systematic review and meta-regression analyses. Journal of Personality Disorders, 26, 775-792. doi: 10.1521/pedi.2012.26.5.775 [ Links ]
Zlotnick, C., Clarke, J. G., Friedmann, P. D., Roberts, M. B., Sacks, S., & Melnick, G. (2008). Gender differences in comorbid disorders among offenders in prison substance abuse treatment programs. Behavioral Sciences & The Law, 26, 403-412. doi: 10.1002/bsl.831 [ Links ]
A correspondência relativa a este artigo deverá ser enviada para: Nélio Brazão, CINEICC – Centro de Investigação do Núcleo de Estudos e Intervenção Cognitivo-Comportamental, Faculdade de Psicologia e de Ciências da Educação da Universidade de Coimbra, Rua do Colégio Novo, 3000-115 Coimbra. E-mail: nelio-brazao@hotmail.com
This paper is a part of the Project “GPS – Growing Pro-Social, a prevention and rehabilitation program for individuals with antisocial behavior: Efficacy studies in forensic samples” (PTDC/PSI-PCL/102165/2008). This project is supported by the Foundation for Science and Technology, and it is a partnership between the Research Unit of the Cognitive-Behavioral Research and Intervention Center and the General Directorship of Social Reinsertion and Prison Services of the Portuguese Ministry of Justice.
The authors would like to thank Jorge Monteiro and colleagues from the national prison system for collaborating in this research, as well as Maria do Natal Sousa and Filipe Fernandes for helping in the assessment in the Azores Island. The authors would also like to thank Ana Luísa Rosa for proof-reading the manuscript.
Submissão: 05/11/2014 Aceitação: 28/04/2015

