










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkAnálise Psicológica
versão impressa ISSN 0870-8231versão On-line ISSN 1646-6020
Aná. Psicológica vol.37 no.1 Lisboa mar. 2019
https://doi.org/10.14417/ap.1561
A pilot study of the Portuguese version of the Voices Acceptance and Action Scale: Psychometric properties in a clinical sample with psychosis-spectrum disorders
Estudo piloto da versão portuguesa da Escala de Aceitação e Ação para as Vozes: Propriedades psicométricas numa amostra clínica com perturbações do espectro da psicose
Maria João Martins1, Paula Castilho2, António Macedo3, Ana Telma Pereira3, Paula Vagos4, Diana Carvalho5, Ana Carolina Pascoal5, Célia Barreto Carvalho6
1Center for Research in Neuropsychology and Cognitive and Behavioral Intervention, Faculty of Psychology and Educational Sciences, University of Coimbra, Coimbra, Portugal / Department of Psychological Medicine, Faculty of Medicine, University of Coimbra, Coimbra, Portugal
2Center for Research in Neuropsychology and Cognitive and Behavioral Intervention, Faculty of Psychology and Educational Sciences, University of Coimbra, Coimbra, Portugal
3Department of Psychological Medicine, Faculty of Medicine, University of Coimbra, Coimbra, Portugal
4Universidade Portucalense, Portucalense Institute for Human Development – INPP, Porto, Portugal
5Faculty of Psychology and Educational Sciences, University of Coimbra, Coimbra, Portugal
6Center for Research in Neuropsychology and Cognitive and Behavioral Intervention, Faculty of Psychology and Educational Sciences, University of Coimbra, Coimbra, Portugal / Department of Psychology, Faculty of Human and Social Sciences, University of Azores, Ponta Delgada, Portugal
ABSTRACT
Given the recent interest in acceptance-based interventions for psychosis, it has been recommended that coping with voices mechanisms, namely experiential acceptance, are routinely assessed in clinical and research settings. The Voices Acceptance and Action Scale (VAAS-12) is a self-report measure developed to specifically assess acceptance-based or action-based beliefs in relation to verbal auditory hallucinations. This study aimed to translate, adapt and study the psychometric properties of the Portuguese version of the VAAS-12 in a clinical sample within the psychosis-spectrum disorders. The VAAS-12 was translated and adapted to Portuguese. Its psychometric properties were then studied in a sample of fifty-four male participants, mostly single, unemployed, and with a last week voice hearing experience. Confirmatory analysis was performed for the one-factor and two-factor structure suggested for the VAAS in previous studies. Both had unacceptable fit indicators. Exploratory analysis then yield an alternative two-factor structure (“Non-interference and action” and “Acceptance and Life functioning” subscales) with adequate fit. Adequate internal consistency and construct validity were found, with the VAAS being negatively associated with perception of voices as hostile-dominant and resistance regarding voices. The VAAS-12 seems adequate to use in clinical and research studies, although further study is needed particularly regarding subscale “Acceptance and Life functioning”.
Key words: Acceptance, Committed action, Assessment, Psychometrics, Psychosis.
RESUMO
Tendo em conta o interesse recente nas intervenções baseadas na aceitação para a psicose, tem sido recomendado que os mecanismos de coping com as vozes, nomeadamente a aceitação experiencial, sejam avaliados no contexto clínico e de investigação. A Escala de Aceitação e Ação em relação às Vozes (VAAS-12) é um instrumento de autorresposta especificamente desenvolvido para avaliar as crenças baseadas na aceitação ou na ação em relação às alucinações auditivo-verbais. O presente estudo tem como objetivo a tradução, adaptação e estudo das propriedades psicométricas da versão portuguesa da VAAS-12 numa amostra clínica dentro do espectro das perturbações psicóticas. A VAAS-12 foi traduzida e adaptada para Português. As suas propriedades psicométricas foram posteriormente estudadas numa amostra de cinquenta e quatro participantes do sexo masculino, maioritariamente solteiros, desempregados e com uma experiência de ouvir vozes na última semana. Foram realizadas análises fatoriais confirmatórias para as estruturas de um e dois fatores sugeridas em estudos prévios, sendo que ambas apresentaram índices de ajustamento inaceitáveis. A análise fatorial exploratória realizada posteriormente revelou uma estrutura alternativa de dois fatores (“Não interferência e ação” e “Aceitação e Funcionamento”) que obteve ajustamento adequado. Foi encontrada adequada consistência interna e validade de constructo, tendo sido encontradas associações negativas com a perceção das vozes como hostis-dominantes e resistência em relação às vozes. A VAAS-12 parece ser adequada para uso em contexto clínico e de investigação, embora mais estudos sejam necessários particularmente no que diz respeito à subescala “Aceitação e Funcionamento”.
Palavras-chave: Aceitação, Ação com compromisso, Avaliação, Psicometria, Psicose.
Introduction
The current work intended to translate, adapt and study the psychometric properties of an existing instrument that was developed to evaluated the acceptance and action beliefs in relation to general experiences of verbal auditory hallucinations (i.e., the ‘Voices Acceptance and Action Scale’ – VAAS; Shawyer et al., 2007). The Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association [APA], 2013) defines hallucinations as “perception-like experiences […] without an external stimulus […] not under voluntary control”, occurring in “any sensory modality”, although “usually experienced as voices […] perceived as distinct from the individual’s own thoughts” (p. 87). Verbal auditory hallucinations (referred to ‘voices’ hereafter) are conceptualized as existing in a continuum, ranging from sporadic, non-distressing and non-problematic experiences to severe, frequent, and highly distressing symptoms, usually associated with other psychiatric disorder criteria (e.g., Goldstone, Farhall & Ong, 2012), particularly those within the psychosis-spectrum. This spectrum can be used as a clinical entity or generic diagnostic term because it covers a set of severe conditions (e.g., schizophrenia, schizoaffective disorder, mood disorder with psychotic features) that may include difficulties in five domains of psychopathology: hallucinations, delusions, disorganized thought (speech), disorganized or abnormal motor behavior and negative symptoms (APA, 2013).
Cognitive approaches to voices argue that the interference caused by hearing voices is not directly and unequivocally associated with their presence, content or characteristics (Chadwick & Birchwood, 1994). Instead, distress may arise from a counterproductive relationship with voices, characterized by automatically reacting to their presence by trying to avoid, change, fight and resist them, all of which are forms of experiential avoidance (Hayes, Luoma, Bond, Masuda, & Lillis, 2006). According to Shawyer, Thomas, Morris and Farhall (2013), the hearing voices experience is particularly susceptible to experiential avoidance and to interfering with moving towards one’s valued life directions. In this regard, aspects as the experiences’ intrusiveness and salience (driving attention towards them and evoking unpleasant emotional responses), verbal content (leading to possible cognitive fusion mechanisms) and interpersonal qualities may be particularly relevant.
Studies have found that coping strategies based on avoidance of private experiences predict negative outcomes such as increased frequency of auditory hallucinations (although not when controlling for paranoia), as well as of their severity and associated distress (Varese, Udachina, Myin-Germeys, Oorschot, & Bentall, 2011). Goldstone et al. (2012) found experiential avoidance to be a relevant process in predicting ongoing hallucinations in a psychotic sample, although not when considering auditory hallucinations specifically. Also, Jones and Fernyhough (2009) found an important role of experiential avoidance strategies (i.e., thought suppression and rumination) in predicting hallucination-proneness. Alternatively, several authors propose acceptance as a mechanism through which people who hear voices may protect themselves from developing a clinical disorder (Vilardaga, Hayes, Atkins, Bresee, & Kambizc, 2013). Experiential acceptance has predicted diminished behavioral and emotional resistance to voices (Morris, Garety, & Peters, 2014).
Despite the impact that these constructs may have on psychopathology, their role as coping with voices mechanisms does not seem to be routinely assessed in clinical and research settings (Ratcliff, Farhall, & Shawyer, 2010). Several authors thus recommend the assessment of experiential acceptance (Vilardaga et al., 2013), specifically of voices. Several measures have been developed in the last decades aiming at assessing different aspects (e.g., severity, frequency, beliefs, distress, coping, perceived power, or relationships with the self) of auditory hallucinations in general and voice hearing in particular (for a review see Ratcliff et al., 2010). Nevertheless, there is only one measure specifically developed to assess acceptance of the voice hearing experience and acting with commitment independently of the voice’s presence – the ‘Voices Acceptance and Action Scale’ (VAAS; Shawyer et al., 2007).
The VAAS is a self-report measure developed to specifically assess acceptance-based or action-based beliefs in relation to auditory hallucinations (i.e., detached acceptance of auditory hallucinations while acting effectively towards one’s goals; Shawyer et al., 2007). Inspired mainly by the theoretical framework of Acceptance and Commitment Therapy (ACT; Hayes et al., 2006), the VAAS also considered research on thought suppression and includes ideas from the acceptance perspective of Romme and Esher (1989), who note taking responsibility for actions and understanding voices as a part of life although different from the self. The final version of the scale comprised 31 items divided in Section A, which is a stand-alone 12-item scale measuring acceptance and action related to auditory hallucinations in general, Section B1, referring to committed action in relation to hearing command hallucinations, and Section B2 that mixed acceptance and action items regarding behavioral and emotional responses to potentially harmful command hallucinations. The standalone scale (Section A) has been the most widely studied section of the VAAS and has been also called VAAS-12. It comprises nine acceptance items and three action items, and is intended for persons experiencing voices of any kind, independent of voice’s content (not exclusively command voices).
With a sample of 41 patients with a psychosis-spectrum diagnosis experiencing distressful and interfering medication-resistant command hallucinations, Shawyer and collaborators (2007) found acceptable internal consistency for the VAAS-12 total and the two subscales (i.e., acceptance and action) with Cronbach’s alpha ranging from .76 to .85 and test-retest reliability values ranging from .72 to .82. They also found associations between the VAAS and depressive symptoms, quality of life, and confidence in coping with voices, some of large magnitude. Both subscales were associated with each other and with beliefs about voices. The action subscale successfully discriminated between patients reporting compliance with voices from patients denying having complied with them in the last 6 months. It was found that the VAAS added significant explanation to the prediction of depressive symptoms, coping with command hallucinations, and quality of life beyond the predictive role of beliefs about voices (Shawyer et al., 2007). In a less severe, more heterogeneous and representative voice hearers sample (i.e., 40 outpatients with a schizophrenia or schizoaffective disorder diagnosis) the VAAS-12 also showed adequate internal consistency for the total scale (α=.81) and significant associations with beliefs about voices, negative affect, thought control strategies, depressive symptoms, anxiety, and stress (Brockman, Kiernan, & Murrell, 2015).
Considering the adequate psychometric properties of the VAAS-12, its briefer nature and its wider applicability and clinical utility as a general scale for voices independent of voices’ content (i.e., not restricted to command hallucinations), the present study aims to translate, adapt and study its psychometric properties in a sample of Portuguese participants with a diagnosis of a psychotic-spectrum disorder. In order to fulfill these aims this study followed a non-analytic/descriptive, cross-sectional study design.
Method
Participants
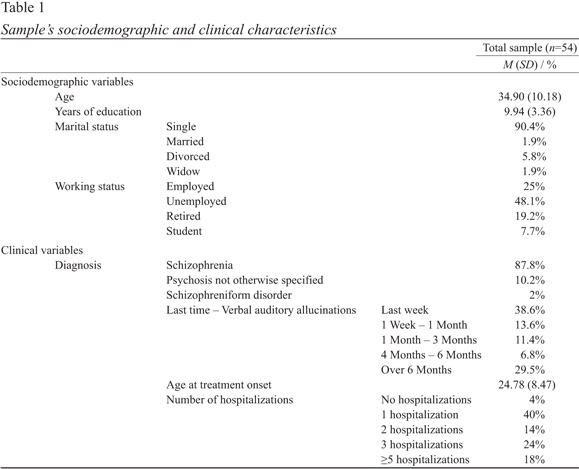
The inclusion criteria for the participation in the present study included: (a) the past or present presence of auditory/verbal hallucinations, either command or other types, (b) a diagnosis of a non-affective psychosis, (c) aged 18 years old or more, (d) absence of severe cognitive deficits, as assessed informally by the patients’ psychiatrists. The exclusion criteria included severe symptomatology that might impede participation, as assessed informally by the patients’ psychiatrists. The present study enrolled 54 male participants. Sociodemographic and clinical characteristics of the sample can be consulted in Table 1.
Only a subsample (n=29) filled in the Beliefs about voices Questionnaire-Revised (Chadwick, Lees, & Birchwood, 2000), in order to test for the construct validity of the VAAS-12.
Measures
Voices Acceptance and Action Scale (VAAS; Shawyer et al., 2007). The VAAS was developed to assess acceptance-based or action-based beliefs in response to auditory verbal hallucinations, in general and specifically to command hallucinations. This 31-item scale is divided into section A (i.e., 12 item stand-alone scale for general auditory hallucinations) and section B, referring specifically to command hallucinations. The participant is asked to rate their opinion from 1 ‘Strongly Disagree’ to 5 ‘Strongly Agree’, with higher scores meaning higher levels of acceptance and perception of acting according to one’s valued life directions. In the present study, only the section A, stand-alone scale was used (i.e., VAAS-12). Preliminary results show evidence internal consistency (Brockman et al., 2015; Shawyer et al., 2007) and test-retest reliability (Shawyer et al., 2007) for the scores of both the total and the two subscales (i.e., acceptance and action) of the VAAS-12.
After permission for the study was obtained from the authors of the original version of the VAAS, the research team proceeded with the translation to the Portuguese language of the VAAS12. The major concern at this stage was to maintain content equivalence between the Portuguese and the original versions. The draft was then sent to a bilingual researcher who was also a psychologist with therapeutic expertise, and who provided the team with a back translation. The back translation was compared with the original version by the research team and also sent to the authors of the original instrument for evaluation. No changes were deemed necessary to the Portuguese version of VAAS12 at this stage.
Beliefs about voices Questionnaire-Revised (BAVQ-R; Chadwick et al., 2000). This 35item scale was developed to evaluate beliefs people hold about verbal auditory hallucinations and their associated emotional and behavioral responses. The participants rate their agreement with each item using a four-point Likert scale in relation to their dominant voice. Chadwick et al. (2000) report five subscales: three concerning beliefs about the voice (“malevolence”, “benevolence”, and “omnipotence”) and the other two regarding behavioral responses (“resistance” and “engagement”). The scale has shown good internal reliability, with alphas ranging from 0.74 to 0.88. Construct validity was examined and strong relationships between the subscales and depressive and anxious symptoms were found (Chadwick et al., 2000). The Portuguese version (Barreto-Carvalho, Martins, da Mota, & Castilho, 2018) found a four-factor structure (“malevolence” and “omnipotence” being fused in only one subscale: hostile-dominance) that was a good fit to the data. In the Portuguese validation study, adequate internal consistency values were found for all subscales (i.e., α between .80 and .92).
Procedure
Sample collection. The sample was collected in five Portuguese hospital centers located in the north and center regions of Portugal, after all procedures were approved by the hospitals’ ethics committees. Participants were recruited after referral from their psychiatrists. In an individual session with one of the researchers, a brief description of the nature and objectives of the study was given and all questions were clarified. Confidentiality and anonymity were assured. Upon their agreement to participate, participants were asked to sign an informed consent form based on the Declaration of Helsinki. Participants were then given the self-report questionnaires that took approximately 30 minutes to complete. Participants were asked to answer the questions regarding the usual way they respond to voices when they hear them. Whenever participants had not had auditory verbal hallucinations in the last week time frame, instructions were given for them to focus on the period when the verbal hallucinations occurred. Participants were instructed to respond without reflecting excessively on the answers and were told that there are no ‘right or wrong’ answers, as ways of reducing the probability of responses driven by social desirability motives. In order to guarantee the validity of responses, one member of the researcher team with clinical expertise was present during the assessment and helped the participants, whether when difficulties in understanding the constructs or specific questions emerged or when the participant required a break, by allowing it or even suggesting one if participants showed signs of fatigue.
Data analysis. Confirmatory factor analyses (CFA) were initially performed to test the one-factor and two-factor structures of the VAAS-12 that had been proposed before (i.e., two-factors and one total scale; Shawyer et al., 2007). Following the results of the CFA, exploratory factor analysis was performed. Considering that our data was not multivariate normal (Mardia’s multivariate skewness statistic=50.77; p<.01; Mardia’s multivariate kurtosis statistic=178.19; p=.04) and that the response scale used five ordinal points, the Maximum Likelihood Robust estimator was used for all confirmatory and exploratory analyses, given that is has performed well with non-normal ordinal data (Li, 2016). To assess model fit, we first used the chi-square goodness-of-fit. A non-significant chi-square is desired as it suggests that the reproduced and observed covariance matrices do not differ significantly; hence, the data fits the proposed model structure (Kline, 2011). Moreover, the guidelines provided by Hu and Bentler (1999) were taken as indications of goodness of fit of the measurement models under analyses. Specifically, the model was considered a good fit for the data if Standardized Root Mean Residual (SRMR)≤.09, combined with either Root Mean Square Error of Approximation (RMSEA)≤.06 or with Comparative Fit index (CFI)≥.95. The confirmatory and exploratory factor analyses were carried out using the Mplus, Version 7 software (Muthén & Muthén, 1998-2011).
After having established the best fitting measurement model, it was further explored via descriptive statistics and internal consistency. Given previous findings on the vulnerabilities of the Cronbach Alpha, particularly when the item’s distribution is asymmetrical (Trizano-Hermosilla & Alvarado, 2016), we used the Guttman’s Lambda-2 as indicative of the measures’ internal consistency, with values higher than .70 being considered acceptable1. Finally, the construct validity of the VAAS-12 was analyzed via correlation analyses of its scores with the scores of a measure of beliefs about voices heard (i.e., BAVQ-R). Convergent validity would be indicated by the emergence of associations between the VAAS and BAVQ-R subscales, since the beliefs regarding the valence of voices (e.g., hostile-dominance) might be associated with lower/higher levels of experiential acceptance. The reactions to voices (e.g., resistance) might be seen as strategies based on experiential avoidance (motivated by the lack of experiential acceptance). These analyses were performed in IBM SPSS Statistics for Windows, Version 20.
Results
Validity evidence based on internal structure
Confirmatory Factor Analysis. In accordance with indications from previous studies (Brockman et al., 2015; Shawyer et al., 2007) for the use of either a one-factor or a two-factor (‘action’ – items 3, 7 and 12; and ‘acceptance’ – the other items) structure, we performed a one-factor and a two-factor CFA on our data. For the one-factor structure, the chi-square goodness-of-fit was significant (χ2(54)=107.01, p<.001), and the global fit indices also indicated a poor model fit (RMSEA=0.14, 90%IC=0.10-0.17; CFI=0.65; SRMR=.13). Similar results were found for the proposed two-factor structure (χ2(53)=106.76, p<.001; RMSEA=0.14, 90%IC=0.10-0.18; CFI=0.64; SRMR=.13).
Exploratory Factor Analysis. Considering the possibility of a different factor structure for the Portuguese population and taking into account the absence of a previous dimensional study of the VAAS-12, we proceeded with Exploratory Factor Analysis. According to parallel analysis, the best solution was a two-factor structure, in which items 2 and 5 (“There are worse things in life than hearing voices” and “My voices are just one part of my life”) were, nonetheless, eliminated due to their non-significant loading on either of the factors. Then, a two-factor 10-item solution presented acceptable fit to our data (χ2(26)=31.03, p=.23; RMSEA=0.06, 90%IC=0.00-0.13; CFI=0.96; SRMR=0.05). Item loadings on each factor are presented in Table 2. The two-factors were not significantly correlated (r=.15, p=.28).
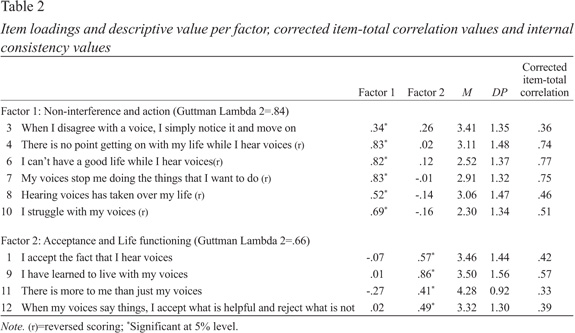
The first factor, which, after looking into the content of the items we named ‘Non-interference and Action’, reflects the intention to move towards valued life directions, giving up the ‘control agenda’ and promoting the non-interference of voices in ones’ life. The second factor, which we named “Acceptance and Life functioning”, intends to measure an accepting way of dealing with voices. High scores indicate the use of adaptive strategies in dealing with voices and the ability to separate the voice hearing experience from the self (i.e., non over identification with the content of voices) and from the person’s life.
Reliability. The “Non-interference and Action” presented a good internal consistency value. The internal consistency value for “Acceptance and Life functioning”, which includes only four items, was borderline adequate. Table 2 presents results regarding item statistics, item-total correlations and internal consistency for each subscale2.
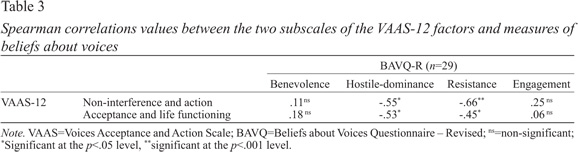
Evidence based on the relations with other variables. In the present study (n=29) the Guttman’s lambda-2 values for the BAVQ-R were .75 for hostile-dominance, .90 for benevolence, .78 for engagement, and .88 for resistance, indicating that it may serve as a consistent measure upon which to study construct validity. Spearman correlations results found between the two measures of the Portuguese VAAS-12 and measures of beliefs about voices that can be seen in Table 3. Overall, moderate to strong (negative) associations of those two measures with negative perception of voices’ intent (i.e., Hostile-dominance) were found, as well as with the behavioral response of resisting voices.
Discussion
Considering the need for psychometrically sound instruments for assessing the voice hearing experience from a contextual behavioral science framework, the present study sought to continue and further explore the work presented by Shawyer et al. (2007) and Brockman et al. (2015) on the psychometric properties of the Voices Acceptance and Action Scale (Section A – 12 items) in a Portuguese sample diagnosed with psychotic spectrum disorders. The current our work went beyond previous works on the psychometrics of the VAAS-12, which had focused solely on its internal consistency, by also explicitly considering its internal structure and construct validity in relation to beliefs about voices.
Though we started with a confirmatory approach based on the measures that were proposed for the VAAS-12 (i.e., two-factor and one-factor models), we found no evidence of their adequacy to Portuguese data. Exploratory evidence favored an alternative two-factor model in the current data, measuring “Non-interference and Action” and “Acceptance and Life Functioning”. From a theoretical point of view, each of these two factors seem to comprise constructs taken from both of the two major theories in which the original authors have based the VAAS, namely the Acceptance and Commitment Therapy framework (Hayes et al., 2006) and the Romme and Escher (1989) approach. The fact that these different theoretical backgrounds for sustained the development of different items may have influenced the division of such items in a factor structure that was different from what was expected and purported. Our proposed factor structure integrates different strategies of dealing with voices into two components, each encompassing beliefs linked both to experiential acceptance and to committed action, instead of separating these constructs in different factors, as originally hypothesized.
So, it seems that the theoretical basis for each factor was broadened within our two-factor measurement model. For example, the utility approach presented in item 12 (accepting helpful things voices say and rejecting the unhelpful) that was originally thought of as measuring ‘action’, may instead be conceptualized as an accepting, adaptive and functioning-focused way of thinking about/dealing with voices. Similarly, we do believe that ‘struggle with voices’ (item 10) can be understood as means of action against the interference/negative effects of voices, including the concept of experiential avoidance in its cognitive, emotional and behavioral facets. Nevertheless, this inversion of the item may not reflect experiential acceptance or integrating voices in the patients’ life, perhaps because not struggling sometimes may mean resignation, giving up or enduring the experience instead of accepting it. Given the non-significant association between these factors, there seems to be evidence of them measuring different constructs, which cannot be explained only by the wording of the items (i.e., the fact that three out of 4 items in this scale are reversed scored).
The two-factor structure that emerged from the current data may be seen as an integration of both theoretical models that focus on what is valued by the voice hearers, in terms of coping with voices in a way that enriches their lives. Specifically, the “Non-interference and Action” is more associated with behavioral and cognitive beliefs aiming at reducing the interference and power of voices in people’s life but also implies some degree of acceptance of voices as transient experiences that are different from reality, with people acting and taking control of their lives instead of reacting automatically to voices. “Acceptance and Life Functioning”, in turn, reflects an adaptation to voices and an integration of voices in life and in the self, but also encompasses the ability to choose information from voices in terms of its utility, thus having a say in their influence in ones’ life directions.
In terms of reliability, the “Non-interference and Action” scale presented good internal consistency, whereas the “Acceptance and Life functioning” scale presented poorer results. This may be due to ‘acceptance’ being a more abstract construct. Reflections on the separation of the ‘self’ from the voices (such as required in item 11 ‘There is more to me than just my voices’) may be difficult for patients with possible impaired abstract thinking. On the other hand, affirmations on the direct acceptance of voices (item 1 ‘I accept the fact that I hear voices’) may be confused with other processes such as resignation or enduring of voices, or simply may not grasp the complexity and conceptual meaning of experiential acceptance. Moreover, the four items that comprise this subscale seem to be measuring different parts of a positive and healthy approach to dealing with voices (i.e., acceptance in item 1, integrating voices as a part of life in item 9 and as part of the self in item 1,1 and the utility criteria for dealing with voices’ content in item 12). Although clinically useful, this diversity may have had negative psychometric consequences, particularly concerning internal consistency.
Both subscales of the Portuguese version of the VAAS-12 were negatively associated with the ‘hostile dominance’ evaluation of voices’ intentions. The negative association between perceived omnipotence of voices and experiential acceptance as well as with disruption caused by voices has been previously reported (Morris et al., 2014). Studies have shown that hearing voices appraised as malevolent and/or omnipotent is associated with higher distress levels (Connor & Birchwood, 2013), and with the tendency to suppress or try to avoid difficult and frightening internal experiences (e.g., Hayes et al., 2006).
Negative and moderate to strong correlations were found between both subscales of the Portuguese version of the VAAS-12 and ‘resistance’ response to voices. The ‘resistance’ subscale refers to trying to stop/prevent the voice from talking or to distract the self from the voice. Distraction and cognitive suppression are known experiential avoidance strategies (Hayes et al., 2006) and therefore seem to be negatively associated with measures of movement towards a valued life, integration of voices as a part of life/self-experience, non-interference of voices in life, and adaptation mechanisms to deal with voices; all of these contents are portrayed in the two subscales proposed for the Portuguese version of the VAAS-12. In fact, these results are in line with previous studies indicating emotional and behavioral resistance to voices to be negatively associated with experiential acceptance (e.g., Morris et al., 2014).
Although theoretically expected, no correlations were found between the two subscales of the VAAS-12 and a more ‘positive’ account of voices, namely the perception of them as benevolent and of engagement with voices. This might be a result due to our sample presenting lower levels of benevolence beliefs regarding voices. In fact, as stated in different studies (e.g., Chadwick, Barnbrook, & Newman-Taylor, 2007) these characteristics are less prevalent in clinical samples. Therefore, generalizations of these results should be done with caution.
There are some limitations to the present study that should be considered. Regarding the internal structure we proposed, although potentially useful and congruent with different theoretic perspectives on coping with voices, we understand it to be preliminary and in need for further study and replication. We did not have the sufficient sample size to test further hypothesis namely a higher order factor for psychological flexibility. Also, the small size and male-only sample may impede the generalizability of our results. Larger and more diversified samples are difficult to collect due to the prevalence of this phenomenon (e.g., low prevalence – APA, 2013) and to mechanisms associated with seeking for help (e.g., shame, stigma). Still, efforts should be made to test other properties of the VAAS-12 in larger samples, for instance sensitivity to change or invariance across specific diagnosis within the psychosis-spectrum. The VAAS-12 should also be tested comparing current voice hearers with people who are retrospectively remembering the voice hearing experience, since the self-report of retrospective accounts may have limitations, making new methods such as Experience Sampling Method more useful. Finally, considering the continuum hypothesis of the voice hearing experience, the assessment of VAAS-12 psychometric properties would benefit from data from both clinical and non-clinical samples.
In conclusion, the current work contributed evidence to the internal structure of the Portuguese version of the VAAS-12. This brief instrument measures several aspects of accepting voices and allows understanding of the usefulness/ non-usefulness of coping strategies that people may use to cope with the voice hearing experience. The VAAS-12 is a widely used instrument in acceptance-based clinical trials (e.g., Shawyer et al., 2012), though its psychometric features have scarcely been addressed, particularly within clinical samples. So, by adding evidence to that already collected by international research, the present study further confirmed the potential of the VAAS-12 for research and clinical purposes.
References
American Psychiatric Association [APA]. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing. [ Links ]
Barreto-Carvalho, C., Martins, M. J., da Motta, C., & Castilho, P. (2018). Relating with voices: Model comparison and properties of the Voice Rank Scale and Beliefs About Voices Scale in a sample of patients with schizophrenia. Manuscript submitted for publication. [ Links ]
Brockman, R., Kiernan, M., & Murrell, E. (2015). Psychometric properties of two brief versions of the voices acceptance and action scale (VAAS): Implications for the second-wave and third-wave behavioural and cognitive approaches to auditory hallucinations. Clinical Psychology & Psychotherapy, 22, 450-459. doi: 10.1002/cpp. [ Links ]1916
Chadwick, P., Barnbrook, E., & Newman-Taylor, K. (2007). Responding mindfully to distressing voices: Links with meaning, affect and relationship with voice. Tidsskrift for Norsk Psykologforening, 44, 581-587. [ Links ]
Chadwick, P., & Birchwood, M. (1994). The omnipotence of voices: A cognitive approach to auditory hallucinations. The British Journal of Psychiatry, 164, 190-201. doi: 10.1192/bjp.164.2.190 [ Links ]
Chadwick, P., Lees, S., & Birchwood, M. (2000). The revised Beliefs About Voices Questionnaire (BAVQ-R). The British Journal of Psychiatry, 177, 229-232. doi: 10.1192/bjp.177.3.229 [ Links ]
Connor, C., & Birchwood, M. (2013). Through the looking glass: Self-reassuring meta-cognitive capacity and its relationship with the thematic content of voices. Frontiers in Human Neuroscience, 7, 213. doi: 10.3389/fnhum.2013.00213 [ Links ]
Goldstone, E., Farhall, J., & Ong, B. (2012). Modelling the emergence of hallucinations – Early acquired vulnerabilities, proximal life stressors and maladaptive psychological processes. Social Psychiatry and Psychiatric Epidemiology, 47, 1367-1380. doi: 10.1007/s00127-011-0446-9
Hayes, S. C., Luoma, J., Bond, F., Masuda, A., & Lillis, J. (2006). Acceptance and commitment therapy: Model, processes, and outcomes. Behaviour Research and Therapy, 44, 1-25. doi: 10.1016/j.brat.2005.06.006 [ Links ]
Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1-55. doi: 10.1080/10705519909540118 [ Links ]
Jones, S. R., & Fernyhough, C. (2009). Rumination, reflection, intrusive thoughts, and hallucination proneness: Towards a new model. Behaviour Research and Therapy, 47, 54-59. doi: 10.1016/j.brat.2008.09.008 [ Links ]
Kline, R. B. (2011). Principles and practice of structural equation modeling (3rd ed.). New York: Guilford Press. doi: 10.1038/156278a0 [ Links ]
Li, C. H. (2016). Confirmatory factor analysis with ordinal data: Comparing robust maximum likelihood and diagonally weighted least squares. Behavior Research Methods, 48, 936-949. doi: 10.3758/s13428-015-0619-7 [ Links ]
Morris, E. M., Garety, P., & Peters, E. (2014). Psychological flexibility and nonjudgemental acceptance in voice hearers: Relationships with omnipotence and distress. Australian & New Zealand Journal of Psychiatry, 48, 1150-1162. doi: 10.1177/0004867414535671 [ Links ]
Muthén, L. K., & Muthén, B. O. (1998-2011). Mplus User’s Guide (6th ed.). Los Angeles, CA: Muthén & Muthén.
Ratcliff, K., Farhall, J., & Shawyer, F. (2010). Auditory hallucinations: A review of assessment tools. Clinical Psychology & Psychotherapy, 18, 524-534. doi: 10.1002/cpp.729 [ Links ]
Romme, M., & Escher, A. (1989). Hearing voices. Schizophrenia Bulletin, 15, 209-216. doi: 10.1093/schbul/15.2.209 [ Links ]
Shawyer, F., Farhall, J., Mackinnon, A., Trauer, T., Sims, E., Ratcliff, K., . . . Copolov, D. (2012). A randomised controlled trial of acceptance-based cognitive behavioural therapy for command hallucinations in psychotic disorders. Behaviour Research and Therapy, 50, 110-121. doi: 10.1016/j.brat.2011.11.007 [ Links ]
Shawyer, F., Ratcliff, K., Mackinnon, A., Farhall, J., Hayes, S. C., & Copolov, D. (2007). The Voices Acceptance and Action Scale (VAAS): Pilot data. Journal of Clinical Psychology, 63, 593-606. doi: 10.1002/jclp.20366 [ Links ]
Shawyer, F., Thomas, N., Morris, E. M. J., & Farhall, J. (2013). Theory on voices. In E. M. J. Morris, L. C. Johns, & J. E. Oliver (Eds.), Acceptance and commitment therapy and mindfulness for psychosis (pp. 12-32). Oxford: John Wiley & Sons. doi: 10.1002/9781118499184.ch2 [ Links ]
Trizano-Hermosilla, I., & Alvarado, J. M. (2016). Best alternatives to cronbach’s alpha reliability in realistic conditions: Congeneric and asymmetrical measurements. Frontiers in Psychology, 7. Retrieved from https://doi.org/10.3389/fpsyg.2016.00769
Varese, F., Udachina, A., Myin-Germeys, I., Oorschot, M., & Bentall, R. P. (2011). The relationship between dissociation and auditory verbal hallucinations in the flow of daily life of psychotic patients. Psychosis, 3, 14-28. doi: 10.1080/17522439.2010.548564 [ Links ]
Vilardaga, R., Hayes, S. C., Atkins, D. C., Bresee, C., & Kambizc, A. (2013). Comparing experiential acceptance and cognitive reappraisal as predictors of functional outcome in individuals with serious mental illness. Behaviour Research and Therapy, 51, 425-433. doi: 10.1016/j.brat.2013.04.003 [ Links ]
Correspondence concerning this article should be addressed to: Maria João Martins, CINEICC, Faculty of Psychology and Education Sciences, University of Coimbra, Rua do Colégio Novo, Apartado 6153, 3001-802 Coimbra, Portugal. E-mail martins.mjrv@gmail.com
This research has been supported by the first author, Maria João Martins, Ph.D. Grant (SFRH/BD/96092/2013), sponsored by FCT (Portuguese Foundation for Science and Technology). The authors would like to acknowledge the collaboration of the patients and clinicians from the Psychiatry and Mental Health Departments of the Baixo Vouga Hospital Centre (Aveiro, Portugal), Coimbra University and Hospital Centre (Coimbra, Portugal), Leiria-Pombal Hospital Centre (Leiria, Portugal), Magalhães Lemos Hospital (Oporto, Portugal) and Tondela-Viseu Hospital Centre (Viseu, Portugal) for which we are very grateful.
Submitted: 21/03/2018 Accepted: 23/07/2018
NOTES
1 Please note that, for those same reasons, this same internal consistency indicator was used to calculate the internal consistency of the BAVQ-R as used with the current sample.
2 For the interested reader, and given that the Cronbach alpha value is the most widely used method for estimating internal consistency, Cronbach alpha values were .83 for the “non-interference and action” factor and .64 for the “acceptance and life functioning” factor. Though, based on our results, we do not suggest the use of a complete scale measure, for comparison purposes in relation to the original version of the VAAS-12, the Lambda-2 Guttman for the total scale was .77 and Cronbach alpha value was .73, which changes to .66 by deleting item 6 at its lowest value and to .75 by deleting item 11 at its highest value.

