










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkAnálise Psicológica
versão impressa ISSN 0870-8231versão On-line ISSN 1646-6020
Aná. Psicológica vol.38 no.2 Lisboa dez. 2020
https://doi.org/10.14417/ap.1726
Cognitive deficits, social support, depression and quality of life of post-stroke patients
Défices cognitivos, suporte social, depressão e qualidade de vida após acidente vascular cerebral
Flávia Sousa1, Vânia Rocha2, Clara Estima3, São Luís Castro2, Marina Prista Guerra2
1Faculdade de Psicologia e de Ciências da Educação, Universidade do Porto, Porto, Portugal
2Centro de Psicologia, Faculdade de Psicologia e de Ciências da Educação, Universidade do Porto, Porto, Portugal
3Hospital da Prelada, Porto, Portugal
ABSTRACT
A stroke is a life-threatening event which has physical, emotional and cognitive consequences. This study aimed to identify differences between participants who suffered a stroke and healthy controls, concerning cognitive performance, depressive symptoms, social support and quality of life; to examine the associations between these variables among participants who suffered a stroke; and to identify the variables that best classify patients and controls. The sample included 30 patients who suffered a stroke and 30 healthy participants. Both groups presented similar sociodemographic characteristics. All participants were assessed with The Institute of Cognitive Neurology Frontal Screening, the Montreal Cognitive Assessment, the Hospital Anxiety and Depression Scale, the Instrumental-Expressive Social-Support Scale, and the Short Form Health Survey-36. Post-stroke patients had lower cognitive performance, lower social support, lower quality of life and higher depressive symptoms than the control group. Social support was positively related to quality of life and negatively related to depressive symptoms in the clinical group. Cognitive deficits and depressive symptoms correctly classified belonging to the clinical group in 85% of cases, and significantly predicted the stroke. This study underlines the importance of implementing psychological interventions addressing depressive symptoms and cognitive rehabilitation for post-stroke patients.
Key words: Cognitive deficits, Depression, Social support, Quality of life.
RESUMO
Um acidente vascular cerebral (AVC) é um evento ameaçador à vida que provoca consequências físicas, emocionais e cognitivas. Este estudo apresenta como objectivos: identificar diferenças entre participantes que sofreram um AVC (grupo clínico) e participantes saudáveis (grupo de controlo) no que concerne ao desempenho cognitivo, sintomatologia depressiva, suporte social e qualidade de vida; examinar as associações entre as variáveis em estudo em participantes que sofreram AVC; e identificar as variáveis que melhor classificam os dois grupos de participantes. A amostra incluiu 30 pacientes que sofreram um AVC e 30 participantes saudáveis, com características sociodemográficas semelhantes. A todos os participantes foram aplicados os seguintes instrumentos: The Institute of Cognitive Neurology Frontal Screening, the Montreal Cognitive Assessment, the Hospital Anxiety and Depression Scale, the Instrumental-Expressive Social-Support Scale, e the Short Form Health Survey-36. Pacientes que sofreram um AVC apresentaram défices cognitivos mais significativos, menor suporte social, menor qualidade de vida e sintomatologia depressiva mais elevada comparativamente ao grupo de controlo. O suporte social encontra-se, no grupo clínico, positivamente correlacionado à qualidade de vida e negativamente correlacionado à sintomatologia depressiva. A sintomatologia depressiva e os défices cognitivos classificaram corretamente 85% dos casos do grupo clínico. Este estudo realça a importância de se implementar intervenções psicológicas que incidam na sintomatologia depressiva e na reabilitação cognitiva de pacientes que sofreram um AVC.
Palavras-chave: Alterações cognitivas, Depressão, Suporte social, Qualidade de vida, AVC.
Introduction
Stroke is the second leading cause of death and the third leading cause of adult disability worldwide (World Health Organization, 2016). Following a stroke, most patients suffer from physical, cognitive and emotional complications which can negatively affect their recovery (Bour, Rasquin, Limburg, & Verhey, 2011; Cookson & Casey, 2013).
Cognitive deficits are one of the most common post-stroke complications (Xu, Ren, Prakash, Vijayadas, & Kumar, 2013). They can be caused by oxygen deprivation to brain tissue, and by increased pressure around the infarcted area. The damage effects are influenced by the area of the brain that is injured (Madureira, Guerrero, & Ferro, 2001). For example, in a study with 237 Portuguese patients Madureira et al. (2001) found that about half of the patients had cognitive impairment, and that memory, attention and verbal fluency were the most affected domains in the post-stroke acute phase (up to twelve months after the stroke). Deficits in memory, attention, and language were also the most affected domains one year after the stroke (Lésniak, Bak, Czepiel, Seniów, & Czlonkowska, 2008). Five years after the stroke, impairment of processing speed and executive functioning were the most impaired cognitive domains (Cumming, Marshall, & Lazar, 2013). Cumming, Brodtmann, Darby and Bernhardt (2014) showed that cognitive deficits negatively affected patients’ physical functioning, decreasing their quality of life and increasing depressive symptoms.
According to Pfeil, Gray and Lindsay (2009) it is common for many patients to struggle with emotional side effects following a stroke, such as depression. Em et al. (2015) indicated that patients who suffered a stroke reported more depressive symptoms than participants from a non-clinical sample. In another study, 25% to 79% of patients experienced depressive symptoms after a stroke (Gordon & Hibbard, 1997). Depressive symptoms are more common in the first six months following a stroke, but they can persist up to five years (Barker-Collo, 2007). Lincoln et al. (2013) found, in their study, that 33% patients reported depressive symptoms five years after a stroke. Depression may act as an emotional response to a sudden and disabling illness (Huang et al., 2010), but it can also result from the negative consequences of the stroke itself, such as the decrease of social activity and quality of life (White, Attia, Sturm, Carter, & Magin, 2014). White et al. (2014) followed 134 patients 3, 6, 9 and 12 months after a stroke, and concluded that few patients showed a decrease in depressive symptoms over time. Patients with depressive symptoms also reported lower quality of life, higher physical disability, and less social interactions; on the other hand, patients with less depressive symptoms reported higher social support.
Some individuals may be unable to return to their activities and roles following a stroke, and often have to depend on friends and family for support (O’Sullivan & Chard, 2010). Social support has been reported as an important factor that is associated with a quicker and more extensive recovery of post-stroke patients (Glass, Matchar, Belyea, & Feussner, 1993). Thus, Elloker and Rhoda (2018) stated that post-stroke rehabilitation strategies and interventions could focus on incorporating group activities, namely group sessions with family members and caregivers, as well as outdoor activities with support structures. However, Glass and Maddox (1992) concluded that the impact of social support does not appear during the first month of rehabilitation, indicating the importance of longitudinal designs. Huang et al. (2010) and Lewin, Jöbges and Werheid (2013) found that social support attenuated the depressive symptoms and improved the patients’ quality of life after a stroke by reducing patients’ stress, and promoting self-esteem and social interactions. Social support appears to facilitate problem solving skills and emotional expression, which helped to reduce depressive symptoms (Glymour, Weuve, Fay, Glass, & Berkman, 2008).
Quality of life is a multidimensional concept that includes physical, social, and emotional well-being of individuals (Cumming et al., 2014). Em et al. (2015) found that quality of life was lower among individuals who have suffered a stroke than among healthy participants. Stroke consequences, such as physical disability and lack of social interactions, can lead to depressive symptoms and to a low perceived quality of life (Dayapoglu & Tan, 2010; Em et al., 2015). Furthermore, depression was a significant negative predictor of quality of life in a sample of 50 patients who suffered a stroke (Kim, Warren, Madill, & Hadley, 1999).
The present study aimed: (1) to identify differences between participants who suffered a stroke and healthy controls, concerning cognitive performance and psychosocial variables scores (depressive symptoms, social support and quality of life); (2) to examine the associations between cognitive performance, depressive symptoms, social support and quality of life among participants who suffered a stroke; and (3) to identify which variables best classify patients and controls.
Thus, this study contributes to determine if previously published findings regarding differences in cognitive performance, depressive symptoms, social support and quality of life in a healthy sample compared to a sample of patients surviving a stroke are relevant to a Portuguese population, and it also explores the relationship between these variables in a Portuguese sample. This study can help to understand the patients’ experience after a stroke and to inform of potential intervention strategies and factors to improve rehabilitation of post-stroke patients by exploring cognitive performance and its relationship to quality of life, depressive symptoms, and social support in participants who suffered a stroke, and by identifying the variables that best distinguish the clinical group and the control group.
Methods
Participants
The present study is an observational and correlational study, in which two groups (a clinical group that includes post-stroke patients and a control group without clinical history of a stroke) are identified and compared, as one of the aims of this study is to identify which variables best classify patients and controls.
Sixty participants were included in this study, 30 of which suffered a stroke, and 30 of which were healthy controls. The group of patients who suffered a stroke (clinical group) was recruited from the Physical Medicine and Rehabilitation department of Hospital da Prelada (Portugal). Patients were included in the study if they were 18 years of age or older and were diagnosed with a stroke. Patients with altered states of consciousness, severe language disorders, and difficulties in understanding spoken language or written words were excluded from the study. The control group was a convenience sample recruited from Universidade Sénior e do Autodidata de Lousada and from Movimento Sénior de Cristelos (Portugal). The control group and the clinical group presented similar socio-demographic characteristics. Participants were included in the control group if they were 18 years of age or older and if they were healthy (participants were excluded if they presented disability caused by a physical or psychiatric disorder, such as cancer, stroke, brain injuries, or dementia).
Of the 30 patients who suffered a stroke, 63% (n=19) were men, 73% (n=22) were diagnosed with ischemic stroke, and 57% (n=17) had lesions in the right hemisphere. The mean age was 67.13 years (SD=10.85), with an age range of 47 to 89 years. The mean years of schooling was seven (M=7.00, SD=4.08). Most participants lived with their partner (70%; n=21) and were retired (90%; n=27). Seventy-seven percent of participants (n=23) had no previous history of stroke, and the mean of months elapsed between the last stroke and the data collection was approximately 54 (M=54.23; SD=59.85).
Of the 30 healthy controls, 60% (n=18) were men. The mean age was 66.90 (SD=10.27), with an age range of 48 to 86 The mean years of schooling was seven (M=7.00, SD=4.20). Most participants lived with their partner (86,7%; n=26) and were retired (70%; n=21).
Control participants were matched for gender, age, and educational level with the clinical group. Thus, there were no significant differences between both groups regarding age [t(58)=.086; p=.932], education [t(58)=-.125; p=.901] and gender [χ2(1, n=60)=.000; p=1.00], which means that both groups had similar socio-demographic characteristics.
Instruments
All participants were assessed with the Institute of Cognitive Neurology Frontal Screening, the Montreal Cognitive Assessment, the Hospital Anxiety and Depression Scale, the Instrumental-Expressive Social-Support Scale, and the Short Form Health Survey-36.
The Institute of Cognitive Neurology (INECO) Frontal Screening (IFS) was created by Torralva, Roca, Gleichgerrcht, López and Manes (2009) and validated for the Portuguese population by Moreira, Lima and Vicente (2014) to assess executive functioning. IFS included eight subtests: motor programming, conflicting instructions, go-no go, backwards digit span, verbal working memory, spatial working memory, proverb interpretation, and hayling test. Each subtest corresponds to a specific task and score. Total IFS score was calculated as the sum of each of the eight subtests scores and it can vary between zero and 30 points, with higher scores indicating better executive functioning. The cut-off point for the presence of deficits in executive functioning is a score below 17 points. The Cronbach’s alpha reported by Moreira et al. (2014) was .69. In the current study, the Cronbach’s alpha for this measure was .70.
The Montreal Cognitive Assessment (MoCA) was created by Nasreddine et al. (2005) and validated for the Portuguese population by Freitas, Simões, Alves and Santana (2011) as a cognitive screening tool for detecting mild cognitive impairment. MoCA assessed the following eight cognitive domains: visuospatial and executive functions, naming, attention, language, abstraction, memory, and orientation. Each domain corresponds to specific tasks and score. Total MoCA score was calculated as the sum of each of the eight subtests scores and it can vary between zero and 30 points, with higher scores indicating better cognitive performance. The cut-off point for the presence of cognitive deficits is a score below 26 points. The Cronbach’s alpha reported by Freitas et al. (2011) was .77. In the current study, the Cronbach’s alpha for this measure was .72.
The Hospital Anxiety and Depression Scale (HADS) was created by Zigmong and Snaith (1983) and validated for the Portuguese population by Ribeiro et al. (2007) to assess anxiety and depressive symptoms. HADS includes 14 items: 7 items are included in the anxiety subscale and 7 items are included in the depressive symptoms subscale. In this study, only the depression subscale was administered. Responses were made on a four point Likert-type scale that ranged from zero to three. Total depression subscale score was calculated as the sum of the 7 items scores and it can vary between zero and 21 points, with higher scores indicating higher depressive symptoms. The cut-off point for the presence of depressive symptoms is a score above 7 points. The Cronbach’s alpha reported by Ribeiro et al. (2007) for the depression subscale was .81. In the current study, the Cronbach’s alpha for this measure was also .81.
The Instrumental-Expressive Social-Support Scale (IESSS) was created by Lin, Dean and Ensel (1986) and was validated for the Portuguese population by Guerra (1995) to assess social support. IESSS includes 20 items and responses were made on a five point Likert-type scale that ranged from one (“always”) to five (“never”). Total IESSS score was calculated as the sum of the 20 items scores and it can vary between 20 and 100 points, with higher scores indicating higher perceived social support. The Cronbach’s alpha reported by Guerra (1995) was .83. In the current study, the Cronbach’s alpha for this measure was .68.
The Short-Form Health Survey (SF-36) was created by Ware, Snow, Kosinsky and Gandek (1993) and was validated by the Portuguese population by Ribeiro (2005) to assess health-related quality of life. SF-36 includes 36 items distributed in eight subscales (physical functioning, physical role functioning, bodily pain, general health perceptions, vitality, social role functioning, emotional role functioning, and mental health) and two summary scores (physical component summary (PCS) and the mental component summary (MCS), as there is no single overall score for the SF-36. PCS refers to physical quality of life, whereas MCS refers to mental quality of life. SF-36 subscales scores can vary between zero and 100 points, with higher scores indicating better quality of life, with exception to the bodily pain subscale whose higher scores indicate more bodily pain. The Cronbach’s alpha reported by Ribeiro (2005) ranged from .83 to .94 in the PCS subscales and from .69 to .87 in the MCS subscales. In the current study, the Cronbach’s alpha range from .77 to .95 in the PCS subscales and from .59 to .88 in the MCS subscales.
Procedures
This study was approved by the Faculdade de Psicologia e de Ciências da Educação da Universidade do Porto (FPCEUP) ethics committee and by the Hospital da Prelada ethics committee, in order to proceed to data collection.
The present study included a convenience and non-probabilistic sample, as it did not involve random selection of the participants. Thus, the clinical group’s data was collected at the Physical Medicine and Rehabilitation department of Hospital da Prelada during the internship of one of the researchers. The medical doctor at the hospital signalized the patients who had conditions to participate (e.g., 18 years of age or older; at least three months after the stroke; not having altered states of consciousness, severe language disorders, and difficulties in understanding spoken language or written words). The patients were either hospitalized or had an outpatient medical appointment. All the participants included in the clinical group completed the questionnaires in person, INECO and MoCA were administered by the researcher, and HADS, IESSS and SF-36 were self-administered. Some patients asked the researcher for help to complete the questionnaires due to their functional impairment. In these cases, the questions were asked verbally by the researcher. Participants of the control group were contacted and invited to participate at a senior university (Universidade Sénior e do Autodidata de Lousada) and at an association for elderly people (Movimento Sénior de Cristelos). For the subjects who agreed to be included in the control group, it was scheduled a day and time at their convenience to answer the protocol, mainly at each institution (few participants asked the researcher to administer the questionnaires at their homes). All the participants completed the questionnaires in person, INECO and MoCA were administered by the researcher, and HADS, IESSS and SF-36 were self-administered. No one of the participants asked the researcher for help to complete the questionnaires.
Data collection of both groups took place from January 2016 to May 2016 and were collected in quiet places without distracting elements, in order to not interfere with the participants’ performance and with the institutions activities. The researcher was available to clarify any doubts during the data collection, and to answer any questions about the study. Each participant was informed about the aims of the study, the instruments, and the conditions for participation (e.g., voluntary participation, confidentiality, etc.). If individuals agreed with the conditions and were available to participate in the study, they were asked to sign an informed consent form. All participants included in the study signed an informed consent form based on the Helsinki Declaration.
Statistical analysis
Data were analyzed using the Statistical Package for the Social Sciences, 23.0 version for Windows (IBM SPSS Statistics 23). The Kolmogorov-Smirnov normality test was performed and results showed a normal distribution, thus parametric methods were used. A significance level of .05 was considered, with a 95% confidence interval.
Descriptive analyses were performed to characterize the sample and the variables under study. Cronbach’s alphas were performed to assess the instruments internal consistency. Independent samples t-tests were conducted to compare the results of both groups (clinical group and control group) concerning cognitive performance, depressive symptoms, social support and quality of life. The homogeneity of variances was analyzed by Levine test when performing the t-tests. A Pearson’s product-moment correlations were also performed to examine the strength of the association between the variables included in the study, and a logistic regression was performed to identify which of the main variables best classify patients and controls.
Results
One of the aims of this study was to identify differences between participants who suffered a stroke and healthy controls regarding cognitive performance and psychosocial variables (depressive symptoms, social support and quality of life). Table 1 shows the results regarding the comparison between the clinical group and the control group on cognitive performance scores (IFS and MoCA). Table 1 shows that the control group (M=21.57; SD=3.21) exhibited a higher performance on the IFS than the clinical group (M=15.86; SD=4.63) [t(51.65)=-5.54; p<.01]. The control group also had higher scores than the clinical group in the following IFS subtests: motor programming, conflicting instructions, go-no go, backwards digit span, verbal working memory, and hayling test. There were no significant differences between both groups regarding proverb interpretation [t(58)=-1.06; p=.295] and spatial working memory subtests [t(58)=-1.43; p=.157]. Among the clinical group, 66,7% participants presented executive function deficits, as their IFS scores were below the cut-off point of 17 (Moreira et al., 2014).
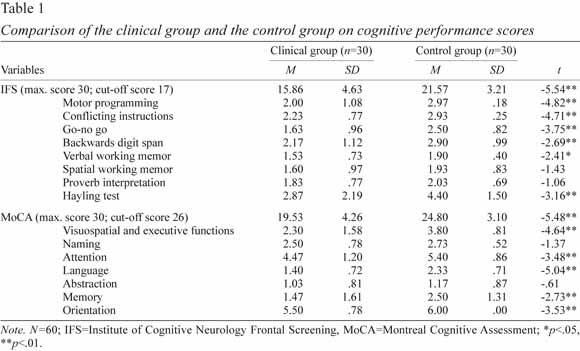
Table 1 also shows that the control group (M=24.80; SD=3.10) exhibited a higher cognitive performance on the MoCA than the clinical group (M=19.53; SD=4.26) [t(58)=-5.48; p<.01]. The control group also had higher scores than the clinical group in the following MoCA subtests: visuospatial and executive functions, attention, language, memory, and orientation. There were no significant differences between both groups regarding naming [t(50.69)=-1.37; p=.178] and abstraction subtests [t(58)=-.61; p=.542]. Among the clinical group, 86,7% participants showed cognitive deficits, assessed by MOCA. On the other hand, only 40% participants in the control group scored below the cut-off point of 26, which reveals the presence of cognitive deficits. As shown in Table 1, patients differed from controls in the IFS and MoCA in almost all of the subscales.
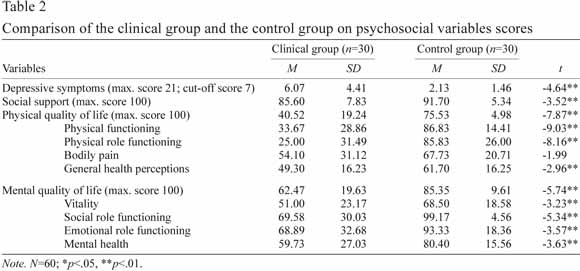
Table 2 shows that the clinical group reported higher depressive symptoms [clinical group: M=6.07; SD=4.41; control group: M=2.13; SD=1.46; t(35.24)=-4.64; p<.01], lower social support scores [clinical group: M=85.60; SD=7.83; control group: M=91.70; SD=5.34; t(58)=-3.52; p<.01], lower physical quality of life (PCS score) [clinical group: M=40.52; SD=.19.24; control group: M=75.53; SD=4.98; t(58)=-7.87; p<.01], and lower mental quality of life (MCS score) [clinical group: M=62.47; SD=19.63; control group: M=85.35; SD=9.61; t(43.13)=-5.74; p<.01] than the control group. The clinical group also reported lower scores in the following SF-36 subtests: physical functioning, physical role functioning, general health perceptions, vitality, social role functioning, emotional role functioning, and mental health. There were no significant differences between both groups regarding the bodily pain subscale [t(50.47)=-1.99; p=.051]. In the clinical group, 33.4% patients reported depressive symptoms, although the mean score of depressive symptoms in the clinical group was 6.07 (SD=4.41) and in the control group was 2.13 (SD=1.46), which stood below the established cut-off point (7/21) for depression.
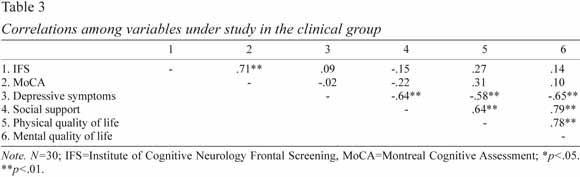
In order to examine the associations among the variables under study in the clinical group, Pearson’s correlation analysis between IFS scores, MoCA scores, depressive symptoms, social support, physical quality of life (PCS), and mental quality of life (MCS) were collected. Table 3 shows that IFS scores and MoCA scores were positively correlated (r=.71; p<.01), but neither significantly correlated to depressive symptoms, social support or quality of life. Depressive symptoms were negatively correlated to social support (r=-.64; p<.01), physical quality of life r=-.58; p<.01) and mental quality of life (r=-.65; p<.01). Social support was positively related to physical quality of life (r=.64; p<.01) and mental quality of life (r=.79; p<.01).
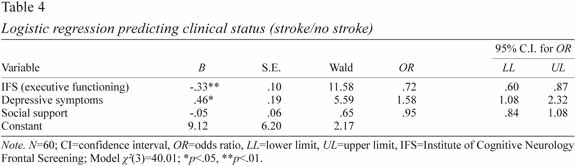
Another goal of our study was to identify the variables that best classify patients and controls. Due to their theoretical relevance and to the study’s sample-size, the logistic regression model contained three independent variables: IFS scores, depressive symptoms, and social support. The IFS had a strong positive correlation with MoCA, thus IFS was included in the model, as it was a more recent neurocognitive tool than MoCA. Depressive symptoms were also included in the model, thus MCS assesed by SF-36 was not selected. Finally, the last variable included in the model was social support that individuals believe to have received in the last 6 months.
A logistic regression was performed and the full model containing IFS scores, depressive symptoms and social support as predictors was statistically significant, χ²(3, n=60)=40.01, p<.01, indicating that the model was able to distinguish between participants who suffered a stroke and healthy controls. The model as a whole explained between 49% (Cox and Snell R square) and 65% (Nagelkerke R squared) of the variance in clinical status, and correctly classified 85% of cases. IFS scores and depressive symptoms made a statistically significant contribution to the model (Table 4). The strongest significant predictor was IFS, recording an odds ratio of .72 (B=-.33; p<.01; 95% IC [.60, .87]). This indicated that participants who exhibited a more effective executive functioning performance were .72 times less likely to report having suffered a stroke than those who did not present an effective executive functioning performance, controlling for all other factors in the model. The odds ratio for depressive symptoms was 1.58 (B=.46; p<.05; 95% IC [1.08, 2.32]), indicating that participants who experienced depressive symptoms were over one time more likely to report having suffered a stroke than those who did not experience depressive symptoms, controlling for all other factors in the model.
Discussion
The present study aimed to identify differences between participants who suffered a stroke and healthy controls, concerning cognitive performance and psychosocial variables scores (depressive symptoms, social support and quality of life); to examine the associations between the variables under study among participants who suffered a stroke; and to identify the variables that best classify patients and controls. The results indicated that patients who suffered a stroke exhibited a lower cognitive performance (both on the IFS and on the MoCA), a lower social support, a lower quality of life, and higher depressive symptoms than the control group.
Several studies have concluded that cognitive deficits were one of the most common post-stroke complications, usually affecting more than half of the patients (Cumming et al., 2013; Xu et al., 2013). Madureira et al. (2001) found that more than half of the patients who suffered a stroke had cognitive impairment. The results of the present study revealed a much higher deficit prevalence assessed by IFS and by MoCA among the clinical group. In this study, the clinical group exhibited a lower performance on working memory, attention and language. Madureira et al. (2001) also found similar results among portuguese patients who suffered a stroke. These authors stated that memory, attention and verbal fluency were the most affected cognitive domains reported in the post-stroke acute phase. Lesniak et al. (2008) also concluded that deficits in memory, attention, and language were most common one year after a stroke. These findings could also be explained due to the participants’ sociodemographic and clinical characteristics: according to Madureira et al. (2001), older patients with a lower level of education present more cognitive deficits, mainly in memory. No significant differences were found between both groups regarding abstraction, spatial working memory, and naming tasks. According to Freitas et al. (2011) and Moreira et al. (2014), age is a risk factor for cognitive impairment. The control group included mainly elderly people, which could explain the similar results found between the clinical group and the control group in the subtests previously mentioned.
Depression can also influence cognitive performance. In this study, there were differences between groups regarding depressive symptoms (one third of the participants who suffered a stroke reported depressive symptoms), but not clinically strong enough for diagnostic. Our findings regarding depressive symptoms, social support, and quality of life among patients who suffered a stroke were similar to the ones found by Gordon and Hibbard (1997), Pfeil et al. (2009), Dayapoglu and Tan (2010), and Em et al. (2015). According to Amaricai and Poenaru (2016) and Lewin et al. (2013), post-stroke depression occurs more frequently in younger patients, as elderly and retired patients experienced stroke as a less significant life-changing event than youngsters and adults. Our sample included mainly elderly people, which may explain the observed low depressive symptoms scores in both groups. The clinical group reported lower social support scores than the control group, but higher than general portuguese population (Guerra, 1995). The high perceived social support may have prevented the clinical group from developing post-stroke depression, and may have also increased quality of life as sustained by literature (Haley, Roth, Kissela, Perkins, & Howard, 2011; White et al., 2014). In addition, there were more healthy controls living with a partner but fewer who were retired compared to the clinical group, which can also help to explain the differences in depressive symptoms and social support scores between both groups. Em et al. (2015) also found that stroke survivors reported a lower quality of life than healthy controls in all SF-36 subscales and summary scores. In our study, all the SF-36 subscales were significant lower in the clinical group, except for the bodily pain subscale. We believe that no significant difference was found in this particular subscale due to the osteoarticular pains often experienced by healthy elderly people.
Social support scores were positively correlated with physical and mental quality of life, and negatively correlated with depressive symptoms in the clinical group. These results were similar to the ones obtained by Huang et al. (2010) and Lewin et al. (2013). Thus, social support can help patients to cope with an unexpected, negative and stress-inducing event such as stroke (Salter, Foley, & Teasell, 2010). We also concluded that post-stroke quality of life is positively related to social support and negatively related to depressive symptoms. Žikić et al. (2014), and Em et al. (2015) reported similar findings in their studies. In the present study, cognitive performance was not significantly correlated to post-stroke depressive symptoms, although Nys et al. (2006) and Cumming et al. (2014) found a negative association between both variables in their studies.
Cognitive deficits assessed by IFS and depressive symptoms were found to be significant predictors that best classify patients and controls. Several studies indicated that cognitive deficits are one of the most significant post-stroke implications (Cumming et al., 2013; Xu et al., 2013). According to Pfeil et al. (2009) and Gordon and Hibbard (1997), depression is the most common post-stroke emotional implication. Although depressive symptoms are more intense in the post-stroke acute phase, they can still remain up to five years after a stroke (Barker-Collo, 2007; Lincoln et al., 2013).
Some limitations of this study deserve mention. One limitation of the present study is that it included a non-probabilistic convenience sample, and the clinical group was only recruited in one single hospital, which may limit the generalization of the results to the Portuguese population of post-stroke patients. Thus, it would be important to collect a larger sample and to include patients from other hospitals and from other Portuguese cities in order to achieve more reliable conclusions. The present study is also an observational study, which do not provide the same level of evidence as other studies. Thus, a prospective study design could contribute to assess cognitive deficits and psychosocial variables (such as depression and quality of life) over time, and how they relate to suspected risk or protection factors. Another limitation was that the selected instruments only focus on executive functioning and global cognitive performance. Thus, there was no specific measure to assess other post-stroke impaired cognitive functions (e.g., memory, attention, language). Future studies should include more complex and specific tests to examine the relationship between cognitive performance and post-stroke depression (Cumming et al., 2013; Lésniak et al., 2008). It would also be useful to collect data about long-term hypertension in healthy controls, as it could help to understand the presence of cognitive deficits in this group. The limitations of the sample (namely sample-size, the sampling method, and the socio-demographic characteristics of the sample) may limit the generalization of the results to the Portuguese population of post-stroke patients.
This study enhances the importance of addressing depressive symptoms and social support in psychological interventions. Cognitive-behavioral therapy has shown effectiveness in the treatment of post-stroke depression (Gordon & Hibbard, 1997), and according to Doble, Shearer, Lall-Phillips and Jones (2009) faciliting a supportive communication between the patient, his family and friends enhances perceived social support. Considering that the mean time elapsed between the stroke and the assessment was almost 5 years (54 months), we find a relevant executive function deficit capable of distinguishing the clinical group and the control group, which was also previously found by Cummings et al. (2013). Thus, it is also important to administer instruments to assess patients’ post-stroke cognitive performance and to consequently identify the preserved and damaged cognitive functions, in order to improve the effectiveness of neuropsychological rehabilitation interventions.
Few studies assessed post-stroke cognitive deficits and their association with depressive symptoms, social support, and quality of life in Portugal. The strengths of the current study include the homogeneity of both samples in terms of group size, gender, age and educational level, which allowed for a clearer analysis and minimized the influence of individual and methodological variables. In addition, a recent neurocognitive tool (IFS) was administered, which was positively correlated with MoCA. MoCA has proved to be a valid instrument for assessing cognitive deficits in patients who have had a stroke (Horstmann, Rizos, Rauch, Arden, & Veltkamp, 2014), whereas IFS focuses on executive functioning, and there are no studies to date on its validity in portuguese patients who suffered a stroke. Therefore, the data of this study contribute to a more accurate assessment of post-stroke patients’ cognitive impairment regarding executive functioning. This study can contribute to the development of larger prospective studies in the future.
References
Amaricai, E., & Poenaru, D. V. (2016). The post-stroke depression and its impact on functioning in young and adult stroke patients of a rehabilitation unit. Journal of Mental Health, 25, 137-141. [ Links ]
Barker-Collo, S. L. (2007). Depression and anxiety 3 months post stroke: Prevalence and correlates. Archives of Clinical Neuropsychology, 22, 519-531. [ Links ]
Bour, A., Rasquin, S., Limburg, M., & Verhey, F. (2011). Depressive symptoms and executive functioning in stroke patients: A follow-up study. International Journal of Geriatric Psychiatry, 26, 679-686. Retrieved from https://doi.org/10.1002/gps.2581 [ Links ]
Cookson, C., & Casey, J. (2013). Social support following stroke. The Psychologist, 26, 566-569. [ Links ]
Cumming, T. B., Brodtmann, A., Darby, D., & Bernhardt, J. (2014). The importance of cognition to quality of life after stroke. Journal of Psychosomatic Research, 77, 374-379. [ Links ]
Cumming, T. B., Marshall, R. S., & Lazar, R. M. (2013). Stroke, cognitive deficits, and rehabilitation: Still an incomplete picture. International Journal of Stroke, 8, 38-45. Retrieved from https://doi.org/10.1111/j.1747-4949.2012.00972.x [ Links ]
Dayapoglu, N., & Tan, M. (2010). Quality of life in stroke patients. Neurology India, 58, 697-701. Retrieved from https://doi.org/10.4103/0028-3886.72165 [ Links ]
Doble, S. E., Shearer, C., Lall-Phillips, J., & Jones, S. (2009). Relation between post-stroke satisfaction with time use, perceived social support and depressive symptoms. Disability & Rehabilitation, 31, 476-473. Retrieved from https://doi.org/10.1080/09638280802168368 [ Links ]
Em, S., Bozkurt, M., Karakoç, M., Çaglayan, M., Akdeníz, D., Oktayoglu, P., . . . Nas, K. (2015). Determining quality of life and associated factors in patients with stroke. Turkish Journal of Physical Medicine & Rehabilitation / Turkiye Fiziksel Tip Ve Rehabilitasyon Dergisi, 61, 148-154. [ Links ]
Elloker, T., & Rhoda, A. (2018). The relationship between social support and participation in stroke: A systematic review. African Journal of Disability, 7, a357. Retrieved from https://doi.org/10.4102/ajod.v7i0.357 [ Links ]
Freitas, S., Simões, M. R., Alves, L., & Santana, I. (2011). Montreal Cognitive Assessment (MoCA): Normative study for the Portuguese population. Journal of Clinical and Experimental Neuropsychology, 33, 989-996. Retrieved from https://doi.org/10.1080/13803395.2011.589374 [ Links ]
Glass, T. A., & Maddox, G. L. (1992). The quality and quantity of social support: Stroke recovery as psycho-social transition. Social Science & Medicine, 34, 1249-1261. Retrieved from https://doi.org/10.1016/0277-9536(92)90317-J [ Links ]
Glass, T. A., Matchar, D. B., Belyea, M., & Feussner, J. R. (1993). Impact of social support on outcome in first stroke. Stroke: A Journal of Cerebral Circulation, 24, 64-70. Retrieved from https://doi.org/10.1161/01.STR.24.1.64 [ Links ]
Glymour, M. M., Weuve, J., Fay, M. E., Glass, T., & Berkman, L. F. (2008). Social ties and cognitive recovery after stroke: Does social integration promote cognitive resilience?. Neuroepidemiology, 31, 10-20. Retrieved from https://doi.org/10.1159/000136646 [ Links ]
Gordon, W. A., & Hibbard, M. R. (1997). Poststroke depression: An examination of the literature. Archives of Physical Medicine and Rehabilitation, 78, 658-663. [ Links ]
Guerra, M. (1995). Uma escala de avaliação do suporte social: Sua aplicação numa população seropositiva ao vírus HIV. Avaliação Psicológica: Formas e Contextos, 3, 25-34. [ Links ]
Haley, W. E., Roth, D. L., Kissela, B., Perkins, M., & Howard, G. (2011). Quality of life after stroke: A prospective longitudinal study. Quality of Life Research, 20, 799-806. [ Links ]
Horstmann, S., Rizos, T., Rauch, G., Arden, C., & Veltkamp, R. (2014). Feasibility of the Montreal Cognitive Assessment in acute stroke patients. European Journal of Neurology, 21, 1387-1393. [ Links ]
Huang, C., Hsu, M., Hsu, S., Cheng, P., Lin, S., & Chuang, C. (2010). Mediating roles of social support on poststroke depression and quality of life in patients with ischemic stroke. Journal of Clinical Nursing, 19, 2752-2762. Retrieved from https://doi.org/10.1111/j.1365-2702.2010.03327.x [ Links ]
Kim, P., Warren, S., Madill, H., & Hadley, M. (1999). Quality of life of stroke survivors. Quality of Life Research: An International Journal of Quality of Life Aspects of Treatment, Care & Rehabilitation, 8, 293-301. [ Links ]
Leśniak, M., Bak, T., Czepiel, W., Seniów, J., & Członkowska, A. (2008). Frequency and prognostic value of cognitive disorders in stroke patients. Dementia and Geriatric Cognitive Disorders, 26, 356-363. Retrieved from https://doi.org/10.1159/000162262 [ Links ]
Lewin, A., Jöbges, M., & Werheid, K. (2013). The influence of self-efficacy, pre-stroke depression and perceived social support on self-reported depressive symptoms during stroke rehabilitation. Neuropsychological Rehabilitation, 23, 546-562. Retrieved from https://doi.org/10.1080/09602011.2013.794742 [ Links ]
Lin, N., Dean, A., & Ensel, W. M. (1986). Social support, life events, and depression. London: Academic Press. [ Links ]
Lincoln, N. B., Brinkmann, N., Cunningham, S., Dejaeger, E., De Weerdt, W., Jenni, W., . . . De Wit, L. (2013). Anxiety and depression after stroke: A 5 year follow-up. Disability and Rehabilitation, 35, 140-145. Retrieved from https://doi.org/10.3109/09638288.2012.691939 [ Links ]
Madureira, S., Guerreiro, M., & Ferro, J. M. (2001). Dementia and cognitive impairment three months after stroke. European Journal of Neurology, 8, 621-627. [ Links ]
Moreira, H. S., Lima, C. F., & Vicente, S. G. (2014). Examining executive dysfunction with the Institute of Cognitive Neurology (INECO) Frontal Screening (IFS): Normative values from a healthy sample and clinical utility in Alzheimer’s disease. Journal of Alzheimer’s Disease, 42, 261-273. Retrieved from https://doi.org/10.3233/JAD-132348
Nasreddine, Z. S., Phillips, N. A., Bédirian, V., Charbonneau, S., Whitehead, V., Collin, I., . . . Chertkow, H. (2005). The Montreal Cognitive Assessment, MoCA: A brief screening tool for Mild Cognitive Impairment. Journal of the American Geriatric Society, 53, 695-699. Retrieved from https://doi.org/10.1111/j.1532-5415.2005.53221.x [ Links ]
Nys, G. S., van Zandvoort, M. E., van der Worp, H. B., de Haan, E. F., de Kort, P. M., Jansen, B. W., & Kappelle, L. J. (2006). Early cognitive impairment predicts long-term depressive symptoms and quality of life after stroke. Journal of the Neurological Sciences, 247, 149-156. [ Links ]
O’Sullivan, C., & Chard, G. (2010). An exploration of participation in leisure activities post stroke. Australian Occupational Therapy Journal, 57, 159-166. Retrieved from https://doi.org/10.1111/j.1440-1630.2009.00833.x [ Links ]
Pfeil, M., Gray, R., & Lindsay, B. (2009). Depression and stroke: A common but often unrecognized combination. British Journal of Nursing (Mark Allen Publishing), 18, 365-369. [ Links ]
Ribeiro, J. (2005). O importante é a saúde: Estudo de adaptação de uma técnica de avaliação da percepção do estado de saúde. Lisboa: Fundação Merck. [ Links ]
Ribeiro, J., Silva, I., Ferreira, T., Martins, A., Meneses, R., & Baltar, M. (2007). Validation study of a Portuguese version of the Hospital Anxiety and Depression Scale. Psychology, Health & Medicine, 12, 225-237. [ Links ]
Salter, K., Foley, N., & Teasell, R. (2010). Social support interventions and mood status post stroke: A review. International Journal of Nursing Studies, 47, 616-625. Retrieved from https://doi.org/10.1016/j.ijnurstu.2009.12.002 [ Links ]
Torralva, T., Roca, M., Gleichgerrcht, E., López, P., & Manes, F. (2009). INECO Frontal Screening (IFS): A brief, sensitive, and specific tool to assess executive functions in dementia. Journal of International Neuropsychology Society, 15, 777-786. [ Links ]
Ware, J., Snow, K., Kosinski, M., & Gandek, B. (1993). SF-36 Health Survey: Manual and interpretation guide. Boston: The Health Institute, New England Medical Center. [ Links ]
White, J. H., Attia, J., Sturm, J., Carter, G., & Magin, P. (2014). Predictors of depression and anxiety in community dwelling stroke survivors: A cohort study. Disability and Rehabilitation, 36, 1975-1982. Retrieved from https://doi.org/10.3109/09638288.2014.884172 [ Links ]
World Health Organization. (2016). Global health estimates 2015: Disease burden by cause, age, sex, by country and by region, 2000-2015. Geneva: WHO Press. [ Links ]
Xu, X.-D., Ren, H.-Y., Prakash, R., Vijayadas, S. M., & Kumar, R. (2013). Outcomes of neuropsychological interventions of stroke. Annals of Indian Academy of Neurology, 16, 319-328. Retrieved from https://doi.org/10.4103/0972-2327.116909 [ Links ]
Žikić, T. R., Divjak, I., Jovićević, M., Semnic, M., Slankamenac, P., Žarkov, M., & Žikić, M. (2014). The effect of post stroke depression on functional outcome and quality of life. Acta Clinica Croatica, 53, 294-301. [ Links ]
Zigmond, A. P., & Snaith, R. P. (1983). The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica, 67, 361-370. [ Links ]
Correspondence concerning this article should be addressed to: Vânia Rocha, Centro de Psicologia, Faculdadede Psicologia e de Ciências da Educação, Universidade do Porto, Rua Alfredo Allen, 4200-135 Porto, Portugal. Email: vmasrocha@gmail.com
Funded by the Portuguese Foundation for Science and Technology through grant UID/PSI/0050/2013 awarded to the Center for Psychology of University of Porto.
Submitted: 26/06/2019 Accepted: 05/02/2020

