











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Intimate partner violence (IPV), a prevalent form of interpersonal violence (Pill et al., 2017), is defined by the World Health Organization (WHO, 2014) as behaviors by an intimate partner that cause physical, sexual, or psychological harm. Globally, almost one in three women will experience IPV in their lifetime (WHO, 2018).
The consequences attributed to perpetrated acts within the scope of IPV, whether direct and immediate or those that proceed, are recognized as an integral part of this scourge (Centers for Disease Control and Prevention [CDC], 2020). The prevalence rates of morbidity and mortality in this population are high, and the likelihood of experiencing an incident of IPV over one’s lifetime appears to be greater than the development of certain physical illnesses, such as diabetes or cancer (Miller & McCaw, 2019). IPV is considered a significant risk factor for women’s health, the effects of which extend even after victims have separated from the abusive context (Hisasue et al., 2024). Furthermore, victimization by IPV is associated with increased use of health services (Makaroun et al., 2020), and these women exhibit heightened vulnerabilities in the development of physical illnesses (Sttubbs & Szoeke, 2021). Nevertheless, there remains a need for improved recognition of this public health issue (Miller & McCaw, 2019).
Among several other demographic and psychosocial factors, PTSD is one of the emotional consequences most consistently studied in victims of IPV (Kiefer et al., 2023; White et al., 2024). Indeed, PTSD symptoms have been associated with the severity of the IPV victimization experience (Konstantopoulou et al., 2024). According to some studies, women with a history of IPV are at least twice as likely to exhibit PTSD symptoms as women without such a history (Iverson et al., 2015). Studies specifically conducted with women victims of IPV also attest to the emergence of symptoms and/or the development of PTSD with high frequencies. For example, in a study by Holmes and colleagues (2019) involving 227 women victims of IPV residing in shelters, 68.3% of the included women met the diagnostic criteria for PTSD. Furthermore, although there are studies demonstrating a positive relationship between various dimensions of IPV and PTSD (Costa & Botelheiro, 2020), the influence of its subcategories is particularly significant in the manifestation of symptoms (Galovski et al., 2021). In this context, psychological violence is recognized as one of the strongest predictors of the emergence of PTSD symptomatology (Dokkedahl et al., 2021). Among the explanations for this strong impact, research suggests that acts of psychological violence are often accompanied by systematic and continuous devaluation from the partner (i.e., prolonged exposure), as well as specific forms of coercion, defamation, and verbal insults directed at the victim, which compromise their ability to initiate or maintain healthy relationships and their self-concept. According to Herman (1992), psychological violence resembles a state of captivity, in which the perpetrator exerts continuous control over the victim. Therefore, it is likely that psychological violence significantly impacts victims, equally or more than the harm resulting from physical or sexual violence, with prolonged exposure being a key factor in this impact (Dokkedahl et al., 2021).
Additionally, that IPV falls within the scope of interpersonal violence is particularly significant, as there are robust associations in the scientific community indicating that interpersonal traumas carry a significantly higher cost for victims compared to non-interpersonal traumas (Thomas et al., 2021). Furthermore, women who are victims of IPV with dependent children may face greater challenges and stress, as many adults with PTSD are also parents (Lauterbach et al., 2007; Leen-Feldner et al., 2011), and several authors have emphasized the need to study the presence of children, particularly with respect to how children affect different vulnerability factors, which may differ from those faced by victims without children (Petersson & Thunberg, 2022). The number of children may be a key factor in these outcomes, as caregiving demands often increase with more children, potentially exacerbating stress and limiting access to mental health resources. According to Lapierre (2010), when women who are victims of IPV with children distance themselves from the abusive context, they tend to experience an increased sense of responsibility, while simultaneously facing fewer resources and means to meet their needs. This disparity appears to be associated with the emergence of feelings of failure, guilt, and self-blame, all of which can intensify mental health symptoms. This is reflected in the study by Brown and colleagues (2020), which found that women with children who were victims of IPV had a higher risk of developing symptoms associated with PTSD. However, despite this recognition, not all victims of IPV develop such issues, and research highlights the importance of considering additional psychosocial variables (Pugliese et al., 2024).
Several risk factors have been identified as contributing to the emergence of this clinical condition, including childhood trauma, low socioeconomic status, low educational attainment, prior exposure to traumatic events, event severity, and cumulative trauma (Cruz et al., 2022; Folayan et al., 2024). Among these, childhood trauma is one of the most prevalent risk factors associated with individuals’ increased vulnerability to developing PTSD (Zwienenberg et al., 2024). For example, the study by Dias and colleagues (2017) found that exposure to childhood abuse in the general population tripled the likelihood of a PTSD diagnosis, with emotional abuse being the most significant predictor of the severity of PTSD symptoms. Studies conducted with women victims of IPV also demonstrated the association between physical, emotional, and/or sexual abuse and PTSD (Hoeboer et al., 2021). As a result, research has shown that women victims of IPV report higher levels of physical and emotional abuse or sexual abuse in childhood (Costa et al., 2019). In this context, it is important to highlight the perspective of the intergenerational transmission of violence theory, which is based on social learning theory (SLT; Bandura, 1977). This theory posits that observing or being a victim of violent behaviors in childhood increases the likelihood of replicating such behaviors or becoming a victim of them in future intimate relationships (Bandura, 1977; Widom, 1989).
Nemeroff (2016) emphasizes that the presence of childhood trauma facilitates the development of mental disorders and physical pathologies, leaving open the specific question regarding the mechanisms involved and the interactions that mediate these consequences. He concludes that, although the question remains unanswered, one of the etiological factors that may help explain this increased susceptibility could be related to the low engagement of childhood trauma victims in health behaviors, as they often deviate, for example, from physical exercise and/or engage in substance use behaviors, which in itself constitutes a risk factor for the development and/or alteration of the developmental trajectory of PTSD symptoms (Hughes et al., 2017; María-Ríos & Morrow, 2020). Campbell and colleagues (2016) found that the presence of childhood abuse was correlated with lower engagement in health behaviors and a greater adoption of risk behaviors, with childhood sexual abuse exhibiting the strongest correlations with the analyzed behaviors. In fact, other studies suggest that childhood sexual abuse is a significant risk factor for revictimization in the context of coercion or sexual assault throughout women’s life cycles (Jaffe et al., 2022). These experiences can lead to the adoption of risky behaviors, which tend to persist once established (Ferreira et al., 2018). For example, the analysis of 19 meta-analyses conducted by Hailes and colleagues (2019) highlights the connections between sexual abuse and 93% of the assessed psychosocial, clinical, and physical health consequences, with engagement in health risk behaviors that may contribute to the escalation of negative consequences (Webster, 2022).
In fact, one of the most frequent comorbidities of PTSD is substance use (Najavits et al., 2020), and the literature suggests links between the symptoms of the disorder and engagement in risk behaviors. Berk-Clark and colleagues (2018) conducted a meta-analysis, which found that individuals diagnosed with PTSD had lower probabilities of consuming healthy food or engaging in sports activities, and higher probabilities of obesity compared to individuals without PTSD. The same relationship can be found for involvement in risky sexual behaviors, with higher levels associated with PTSD (Banks et al., 2022), maladaptive eating behavior (Roer et al., 2021), and risky driving behavior (Bernstein et al., 2022).
In the context of IPV, Teixeira and colleagues (2022) found that women victims of IPV were more likely to self-medicate with sedatives and analgesics as well as to use substances such as alcohol, tobacco, and cannabis. Mehr and colleagues (2023) argue that IPV victims with PTSD symptoms may use substances to alleviate the emotional distress associated with their clinical condition. Therefore, IPV victims are more prone to developing clinical symptoms of PTSD, and the very situation of victimization has been identified as a predictor of involvement in risk behaviors (Ogden et al., 2022; Weiss et al., 2017). For all these reasons, it is suggested that the negative health outcomes for victims may be related to their low engagement in health behaviors (Hoerster et al., 2019; Teixeira et al., 2022; Weiss et al., 2017). However, more studies are needed (Stubbs & Szoeke, 2021).
Despite this recognition, studies focusing on PTSD, childhood trauma, and health behaviors in women victims of IPV are scarce in the international literature and nonexistent, to the best of our knowledge, in the Portuguese context. Therefore, this study aims to fill this gap by analyzing the various physical, psychological, social, and behavioral implications that IPV has for victims, with the goal of contributing to a more informed society that is aware of the changes resulting from this phenomenon, which, although sometimes visible, are often underrecognized (Miller & McCaw, 2019).
The present study
Based on the above discussion, a general objective of this study was to analyze the impact of IPV, physical/emotional abuse, and childhood sexual abuse on PTSD symptomatology, as well as the effect that these variables have on the adoption of health behaviors. Considering the state of the art in this field, the following specific hypotheses were formulated: it is expected that IPV and physical/emotional abuse and childhood sexual abuse will be positive predictors of PTSD symptomatology; and it is expected that IPV, physical/emotional abuse and childhood sexual abuse, and PTSD symptomatology will be negative predictors of health behaviors.
Method
Participants
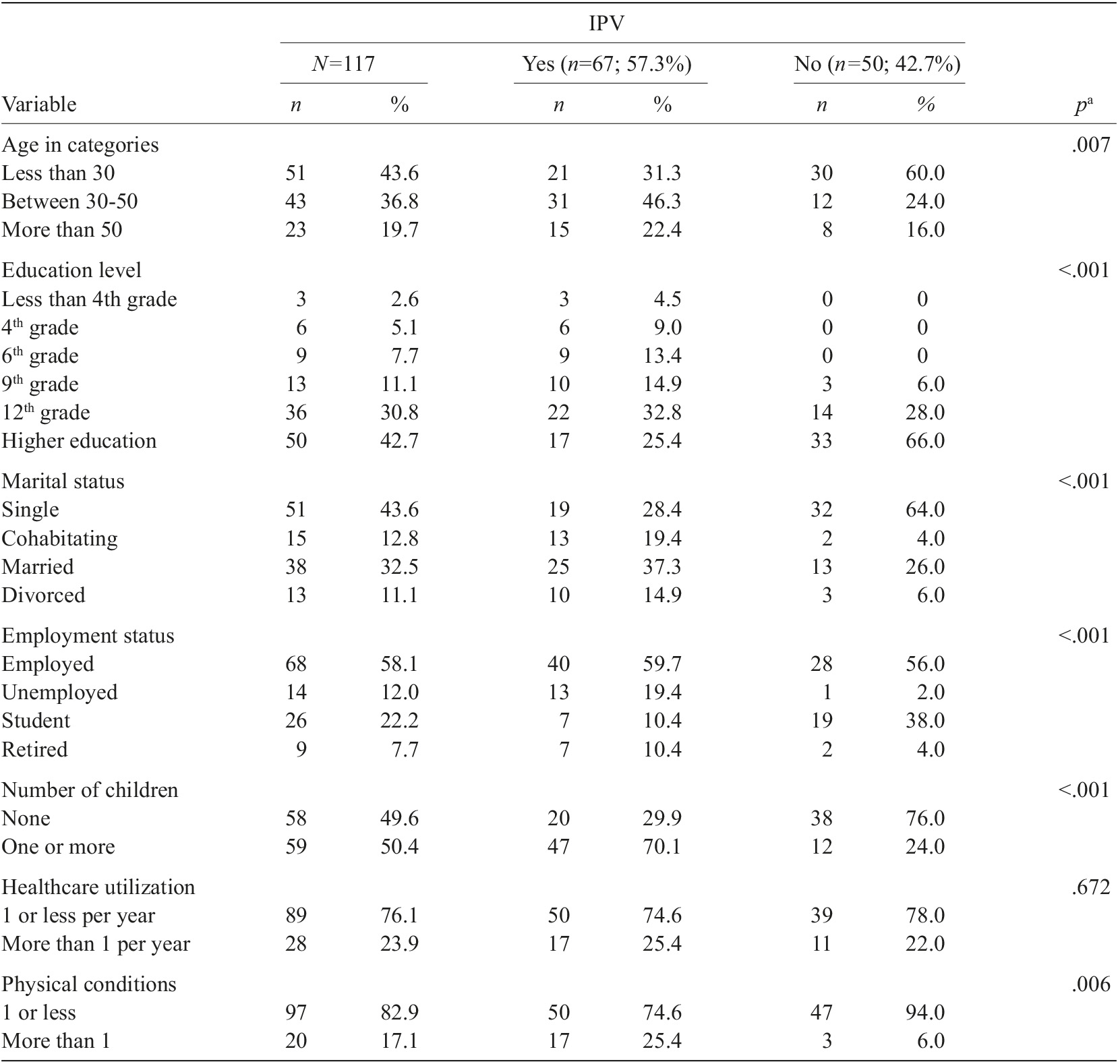
Data were collected from 117 women, 67 IPV victims, and 50 non-victims of IPV using accidental/convenience sampling methods for the IPV victims and snowball sampling for the non-victims. The women who were victims of IPV and participated in the study were recruited through victim support services in the northern area of Portugal. Women from the general population, victims and/or non-victims of IPV, participated in the study by completing the online form. The inclusion criteria were being female, aged 18 years or over, and able to read and write. Two male participants who submitted the online form were excluded from the study. The mean age for the total sample was 37.76 (SD=14.85), with IPV victims having a mean age of 41.45 years (SD=14.44) and non-victims a mean age of 33.82 years (SD=14.06). Participants’ ages ranged from 19 to 74 years. Regarding education level, most victims of IPV have completed secondary school (32.8%) or college education (25.4%), while most non-victims have completed college education (66%). Most women victims of IPV are married or single (37.3% or 28.4%, respectively), while most non-victim women are single (64%). The majority of women, regardless of their victimization status, were employed (59.7% and 56%, respectively). Most women victims of IPV had one or more children (70.1%) and most non-victims had no children (76%).
Measures
Sociodemographic information. A sociodemographic questionnaire comprising continuous and dichotomous questions was utilized to collect data on sociodemographic and clinical variables for women victims of IPV and non-victims. This included variables such as age, gender, education, professional status, marital status, number of children, frequency of healthcare utilization (e.g., Typically, how many times per year do you visit your doctor due to physical complaints you experience?), and presence of physical health conditions (i.e., neurological disorders, diabetes, hypertension, asthma, and/or others).
Revised Conflict Tactics Scales. The CTS2 is a self-report measure that assesses how individuals manage conflicts within intimate relationships. It consists of 39 items, grouped into pairs of questions directed at the participant (victimization scale) and the partner (perpetration scale), totaling 78 items and requiring approximately 10 to 15 minutes for completion. The measure has a five-factor structure, which corresponds to the subscales of negotiation, psychological aggression, sexual coercion, physical abuse with sequelae, and physical abuse without sequelae. In terms of response typology, it includes eight response categories: (1) “once in the past year”; (2) “twice in the past year”; (3) “3-5 times in the past year”; (4) “6-10 times in the past year”; (5) “11-20 times in the past year”; (6) “more than 20 times in the past year”; (7) “not in the past year, but occurred earlier”; and (8) “never occurred.” The first six response categories are designed to assess prevalence and chronicity over the past year, while the remaining categories determine overall prevalence and the absence of such abuse.
In this study, were used the version adapted and validated for the Portuguese population by Paiva and Figueiredo (2006), and used the subscales of psychological aggression (e.g., My partner yelled at me or shouted at me), sexual coercion (e.g., My partner used threats to make me have sexual relations with him), physical abuse without sequelae (e.g., My partner threw something at me that could hurt me), and physical abuse with sequelae (e.g., My partner kicked me) from the victimization scale with a total of 33 items. With regard to the evidence of reliability, Cronbach’s alpha value for the victimization scale was .80, for the subscale of physical abuse without sequelae was .74, followed by the subscale of psychological aggression (α=.64), sexual coercion (α=.51) and physical abuse with sequelae (α=.47; Paiva & Figueiredo, 2006). In the present study, the victimization scale showed an alpha of .96, and .90 for the psychological aggression subscale, .97 for physical aggression without sequelae, .88 in sexual coercion, and .88 for physical aggression with sequelae.
Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5; Weathers et al., 2013). The PCL-5 is a self-report instrument that assesses the 20 symptoms of PTSD according to the DSM-5 (American Psychiatric Association [APA], 2014), validated for the Portuguese population by Carvalho and colleagues (2020). Each item is rated on a five-point Likert scale, with responses indicating the extent to which individuals were affected by each symptom in the past month. The PCL-5 can be used as a continuous variable, assessing the severity of symptoms, or as a dichotomous variable, allowing for a provisional diagnosis of PTSD.
The instrument has a cutoff point of 33 or higher, and a diagnosis of PTSD is suggested based on the following criteria: the total score is equal to or above the cutoff; an individual item is rated at or above the cutoff on the response scale (i.e., 2 [moderately]); and the necessary number of symptomatic items for a diagnosis according to the DSM-5 are present, namely, at least one item related to intrusions and avoidance (e.g., Avoiding memories, thoughts, or feelings related to the stressful experience?), and two items related to negative alterations in cognition and mood (e.g., Blaming yourself or someone else for the stressful experience or what happened after it?) and changes in reactivity and arousal (e.g., Irritable behavior, angry outbursts, or acting aggressively?; Blevins et al., 2015; Weathers et al., 2013).
The results of the validation study for the Portuguese population reveal adequate internal consistency values for the factors reexperiencing (α=.89), avoidance (α=.76), negative changes in cognitions and mood (α=.87), and changes in activation and reactivity (α=.85). For the total scale, the Cronbach’s alpha value was .94 (Carvalho et al., 2020). In the present study, the alpha value for the total scale was .97.
Childhood Trauma Questionnaire (CTQ; Bernstein et al., 2003). The CTQ is a retrospective self-report measure that assesses the history of childhood abuse and neglect. It includes 28 items, derived from the long version of 70 items developed by Bernstein and colleagues (1994), and five traumatic components: physical abuse, emotional abuse, sexual abuse, physical neglect, and emotional neglect (Grassi-Oliveira et al., 2006). It was translated and validated for the Portuguese population by Costa and McIntyre (2006) and is composed of 11 items from the original scale, which form two subscales: physical/emotional abuse (5 items; e.g., When I was 15 years old or younger, someone in my family yelled and shouted at me) and sexual abuse (6 items; e.g., When I was 15 years old or younger, someone tried to touch me sexually or tried to force me to touch them). Each item is rated on a 5-point Likert scale, ranging from 1 “never true” to 5 “very often true.” The time required for completion varies between 10 to 15 minutes. Regarding evidence of reliability, the Cronbach’s alpha value in the validation study was .74 for physical/emotional abuse and .72 for sexual abuse. In the present study, the internal consistency values were .88 for physical/emotional abuse and .95 for sexual abuse.
Questionnaire of Attitudes and Health Behaviors (QACS; Pais-Ribeiro, 2004). To assess health behaviors, the QACS, developed by Pais-Ribeiro (2004), was administered. It comprises 28 items measuring the daily adoption of health behaviors across various domains related to general health. Responses are provided on a Likert scale ranging from 1 “almost always” to 5 “almost never.” Completion time for the QACS is approximately five to ten minutes, with total scores ranging from 28 to 140. The questionnaire includes five subscales: physical exercise (3 items), nutrition (5 items), self-care (11 items), motor safety (3 items), and substance use (6 items). Item scores can be summed for individual subscales or an overall score. The internal consistency of the total scale was reported as .76 in the original study (Pais-Ribeiro, 2004). In the present study, only the overall participant scores were utilized, yielding a Cronbach’s alpha of .91.
Procedures
Permission was requested from various victim support entities to facilitate the identification and subsequent participation of women victims of IPV. During the initial contact with these entities, efforts were made to ensure the consistency of the conditions under which the questionnaires would be administered, as well as to emphasize the importance of participants’ understanding of the questions during administration. After data collection was authorized, participants were contacted by the heads of the relevant organizations. They informed participants about the study’s purpose, the estimated response time (15 to 25 minutes), and emphasized that participation was voluntary, anonymous, and confidential. This process began in May 2021 and ended in January 2022 due to the restrictions associated with the COVID-19 pandemic. For data collection from women in the general population, the link was initially shared within the researcher’s immediate network, with participants encouraged to disseminate it further, emphasizing the inclusion criteria. Informed consent, voluntary participation, anonymity, and confidentiality of responses were ensured. Regarding the ethical aspects, this study received approval from the Ethics Committee of the Faculty of Philosophy and Social Sciences at the Portuguese Catholic University.
Analyses
The IBM® SPSS Statistics 23 statistical analysis software was used for this quantitative study. The distributions of the scores in the variables were assumed to be normal, according to the central limit theorem (Field, 2009). Descriptive analyses of the sociodemographic and clinical variables were performed. Categorical variables were described as absolute and relative frequencies. In addition, t-tests (for continuous variables) and Chi-square tests (for categorical variables) were performed to compare the sociodemographic and clinical variables of women victims and non-victims of IPV. Independent t tests were used to establish differences. To investigate the associations Pearson correlation coefficients were computed. Hierarchical regression analyses were performed after analyzing the variables that were correlated to assess the effects of consider variables in predicting PTSD, and health behaviors. For the regression models a criterion of 10 to 15 participants per variable included in the regression was considered (Field, 2009). In all blocks, the variables that were related to the dependent variables were equated. Data were considered significant if the F value for the change in R 2 associated with each model was significant. In all analyses, p-values<.05 were considered statistically significant.
Results
Demographics
The study sample consisted of 117 women, 67 victims and 50 non-victims. Regarding annual use of medical services, most of the women in both groups report less than one utilization (74.6% for IPV victims and 78% for non-IPV victims). About the number of physical illnesses, 25.4% of IPV victims and 6% of non-IPV victims live with more than one physical illness. Statistically significant differences were found for all sociodemographic variables and for the clinical variable of physical illnesses. Therefore, women victims of IPV are older (p=.007), have less education (p<.001), are more unemployed and retired in a consensual union (p<.001), married or divorced (p=.001), have more children than non victim women (p<.001), and live with more physical illnesses (p=.006; see Table 1).
Differences between women with versus without IPV
As shown in Table 2, women victims of IPV experienced, on average, more childhood physical and emotional abuse (M=4.33, SD=5.13) and childhood sexual abuse (M=1.36, SD=4.13), compared to women non-victims of IPV (M=1. 70, SD=2.80; M=.02, SD=.14, respectively), with statistically significant differences being found for childhood physical and emotional abuse (t=3.547, p=.001), as well as for childhood sexual abuse (t=2.653, p=.010). In relation to PTSD symptoms, statistically significant differences were found according to the victimization situation (t=8.168, p<.001), with women victims of IPV having on average, higher PTSD symptoms (M=25.58, SD=18.75), compared to women who were not victims (M=4.80, SD=7.83). Regarding health behaviors, statistically significant differences were also found (t=-4.777, p<.001), with women victims of IPV showing, on average, lower adoption of health behaviors (M=97.97, SD=21.16), compared to non-victims (M=112.92, SD=14.47).

Relation between IPV, childhood trauma, PTSD symptoms and health behaviors
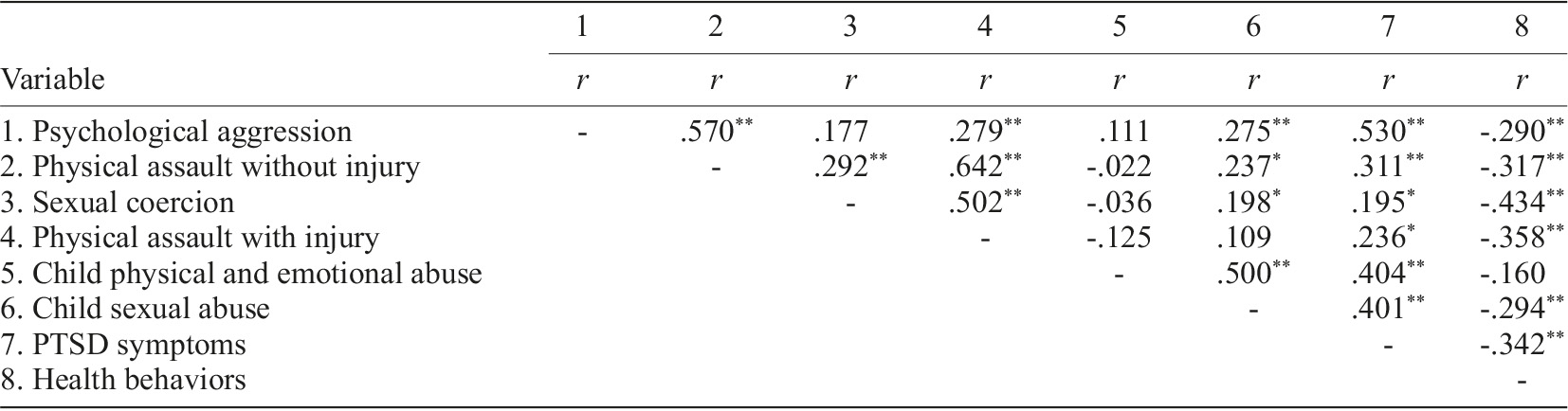
As can be seen in Table 3, no statistically significant correlations were found between the subcategories of IPV and physical and emotional abuse in childhood. On the other hand, except for the subcategory of physical assault with injury, all the remaining subcategories were positively correlated with childhood sexual abuse (i.e., psychological aggression [r=.275, p<.01], physical assault without sequelae [r=.237, p<.05], sexual coercion [r=.198, p<.05]. Regarding PTSD symptomatology, positive and statistically significant correlations were found with all subcategories of IPV (i.e., psychological aggression [r=.530, p<.01], physical assault without sequelae [r=.311, p<.05], sexual coerciony [r=.195, p<.05], physical assault with sequelae [r=.236, p<.05]), physical and emotional abuse [r=.404, p<.01] and childhood sexual abuse [r=.401, p<.01], and a negative and statistically significant correlation with health behaviors [r=-.294, p<.01]. Respecting health behaviors, negative and statistically significant correlations were also found for all variables, except for physical and emotional abuse in childhood, ranging from .290 to .434 (p<.01).
Effects of child abuse and IPV severity on PTSD symptoms
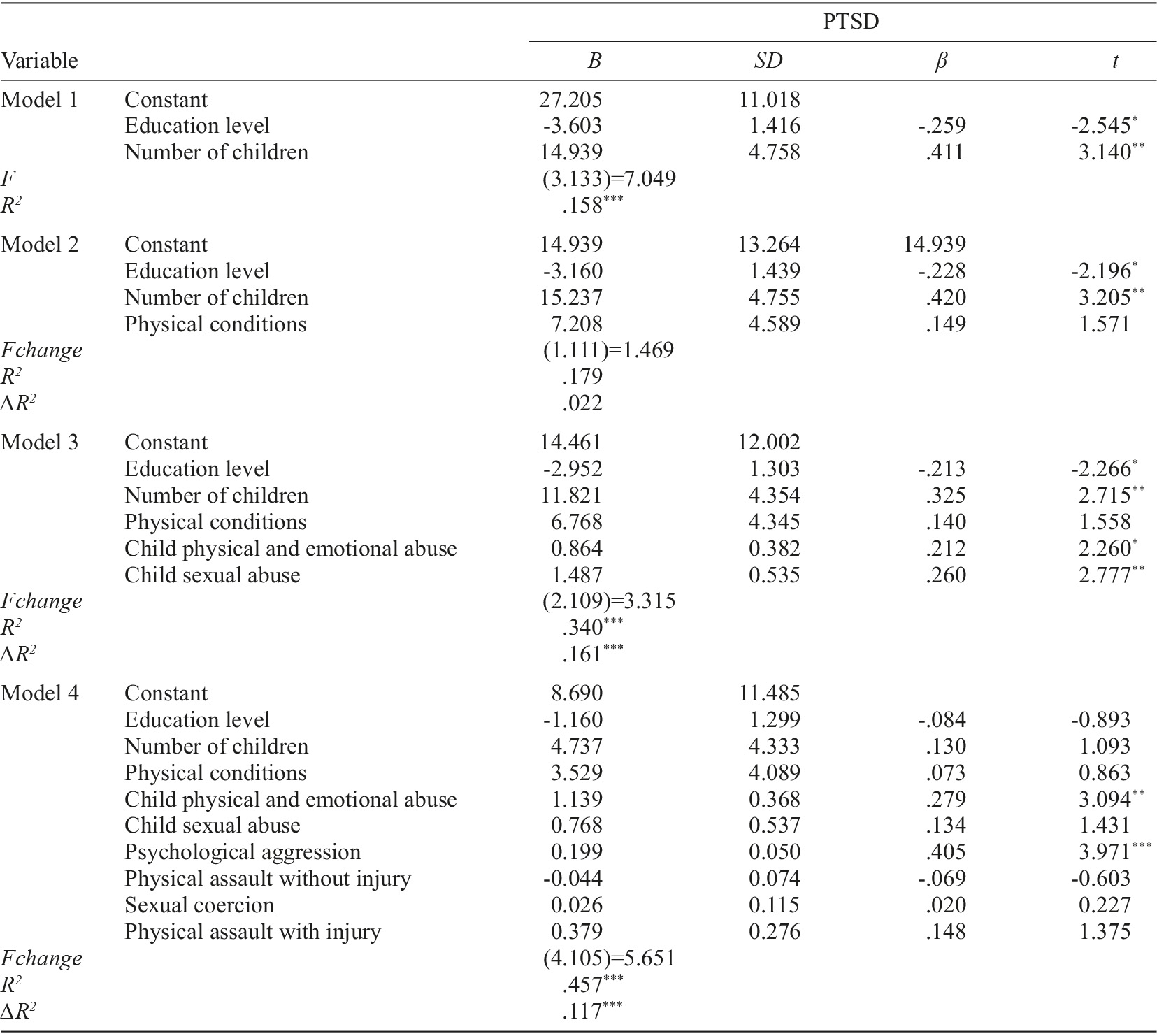
Table 4 shows the results of the hierarchical linear regression analyses for the total sample. Results show a statistically significant model 1 (F[3.113]=7.049, p<.001), which includes two socio-demographic variables as predictors (i.e., education and number of children), explaining 15.8% of the variance in PTSD symptomatology (R 2 =.158). Model 2, to which the clinical variable physical illness was added, explained an additional 2.2% variance, after controlling for the previous variables, and was not statistically significant (R 2 change=.022, Fchange[2.111]=1.469, p=.235). Model 3, to which the variables, physical and emotional abuse, and childhood sexual abuse, were added, explained an additional 16.1% variance and was significant (R 2 change=.169, F[2.109]=13.315, p<.001). To model 4, the variables relating to IPV victimization (i.e., psychological assault, physical assault without sequelae, sexual coercion, and physical assault with sequelae) were added and explained an additional variance of 11.7% and was statistically significant (R 2 change=.118, F[4.105]=5.651, p<.001). Overall, the model explained a total variance of 45.7% (R 2 =.457), suggesting that physical and emotional abuse in childhood and the severity of the psychological aggression subcategory are admittedly the strongest predictors of PTSD symptomatology.
Effects of child abuse, IPV severity and PTSD symptoms on health behaviors
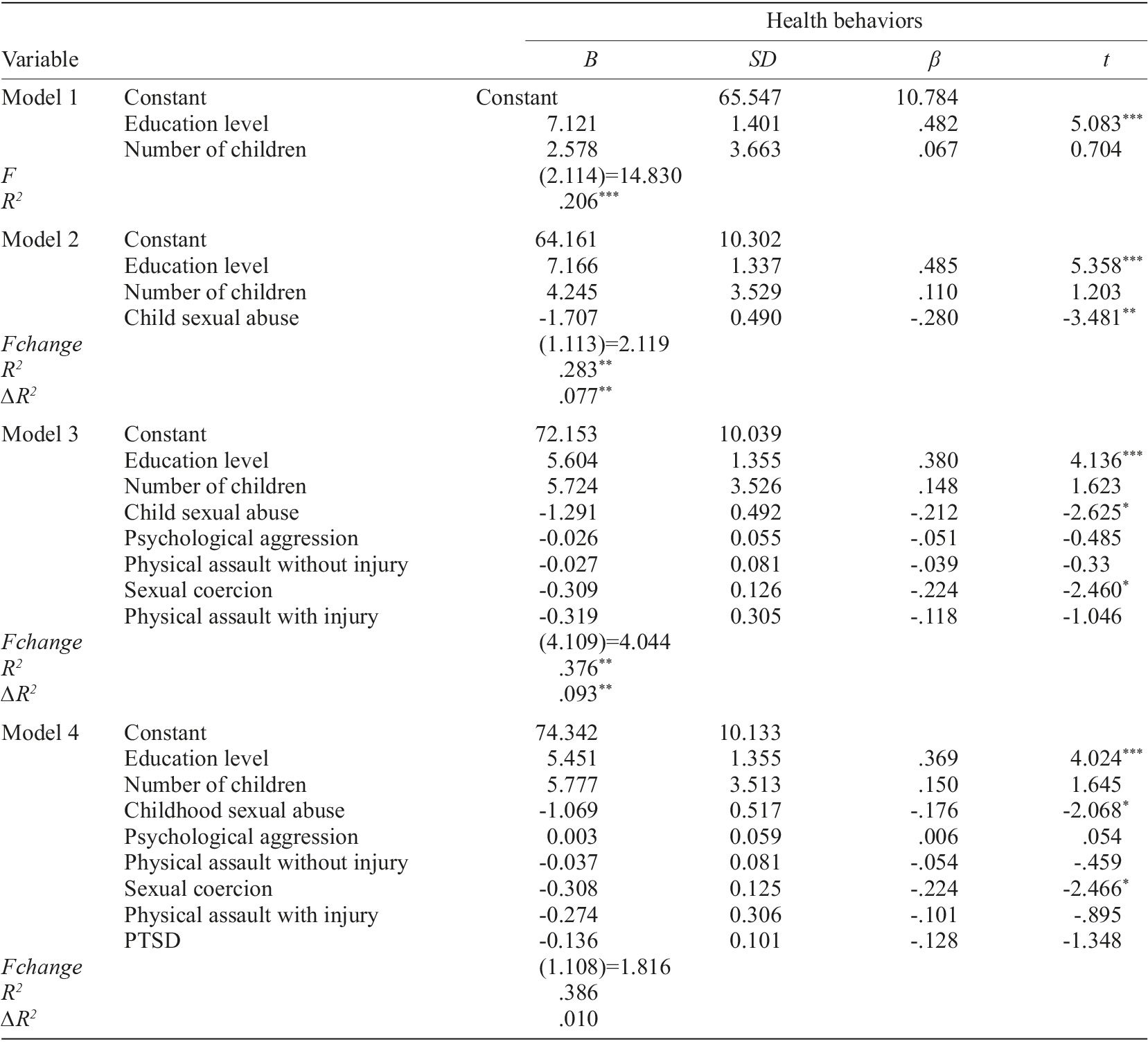
Table 5 presents the results of the hierarchical linear regression analyses for the total sample. The results show a statistically significant model 1 (F[2.114]=14.830, p<.001), which includes two sociodemographic variables as predictors (i.e., education and number of children), explaining 20.6% of the adoption of health behaviors (R 2 =.206). Model 2, to which the childhood sexual abuse variable was added, explained an additional 7.7% variance, after controlling for the previous variables, and was statistically significant (R 2 change=.077, Fchange[1.113]=2.119, p<.01). Model 3, to which the variables relating to IPV victimization (i.e., psychological assault, physical assault without sequelae, sexual coercion and physical assault with sequelae) were added, explained an additional 9.3% variance and was statistically significant (R 2 change=.093, F[4.109]=4.044, p<.01). PTSD was added to model 4, and explained an additional 10% variance, and was not statistically significant (R 2 change=.010, Fchange[1.108]=1.816, p=.181). Overall, the model explained a total variance of 38.6% (R 2 =.386), suggesting that childhood sexual abuse and the severity of the sexual coercion subcategory are admitted to be the strongest negative predictors of health behaviors.
Discussion
The primary objective of this study was to analyze the impact of IPV, physical/emotional abuse, and childhood sexual abuse on PTSD symptomatology, as well as the effect these variables have on the adoption of health behaviors. To the best of our knowledge, studies investigating childhood trauma, PTSD, and engagement in health behaviors in IPV victims are scarce in the international literature and nonexistent in the Portuguese context.
The hypothesis posited that IPV, physical/emotional abuse, and childhood sexual abuse are positive predictors of PTSD symptomatology. Our results provide empirical support for this hypothesis, indicating that, after adjusting for education level and number of children, physical/emotional abuse in childhood, childhood sexual abuse, and the severity of psychological aggression were significant predictors of PTSD symptomatology. Physical/emotional abuse in childhood and the subcategory of IPV related to psychological aggression emerged as the strongest predictors of PTSD. These results are consistent with prior studies suggesting that childhood trauma and IPV increase the risk of developing PTSD symptoms (Costa et al., 2020; Cruz et al., 2022; Dias et al., 2017; Zwienenberg et al., 2024). Studies show that women who experience IPV are three times more likely to develop PTSD symptoms compared to those without a history of IPV (Iverson et al., 2015). Our findings further confirm that psychological IPV is one of the strongest predictors of PTSD, aligning with evidence regarding the specific contributions of the subcategories that comprise IPV (Galovski et al., 2021). Psychological violence seems to have more severe consequences than physical or sexual violence and has been classified as one of the strongest predictors of PTSD in women victims of IPV (Dokkedahl et al., 2021). Some authors explain this relationship by referring to the convergence of specific forms of coercion, defamation, and verbal insults directed at the victim, resembling a state of captivity (Herman, 1992), in which continuous and systematic control over the victim leads to significant harm that can undermine their ability to initiate or maintain healthy relationships, as well as their self-concept. Regarding the number of children, further research is needed to examine its role in mental health outcomes for IPV victims. This is particularly relevant in light of Lapierre’s (2010) perspective, which suggests that IPV victims with children may experience an exacerbation of mental health symptoms. Such exacerbation may be due to an increased sense of responsibility and a simultaneous lack of resources after leaving the abusive relationship. It is important to note that the victims included in this study were recruited from support structures after seeking help and leaving the abusive relationship. Nevertheless, additional studies are needed to further investigate this relationship. These results also highlight the need for early assessment and intervention for women with a history of childhood abuse, which emerges as a crucial element in preventing revictimization and the deterioration of mental health. Similarly, according to our results, attention must be paid to the invisible effects of psychological violence, whose outcomes demonstrate greater damage compared to acts of physical or sexual violence.
The other hypothesis suggests that IPV, physical/emotional abuse, childhood sexual abuse, and PTSD symptomatology are negative predictors of health behaviors. Our results partially support this hypothesis. After controlling for education level, childhood sexual abuse and greater severity of IPV related to sexual coercion were identified as negative predictors of health behaviors, confirming that childhood trauma and IPV adversely affect health behavior engagement. PTSD did not emerge as a predictor of health behaviors in the regression analysis, although it showed significant negative correlations with health behaviors. This discrepancy might suggest that childhood trauma and IPV may play a more direct role in influencing health behaviors. PTSD is frequently associated with a range of risky behaviors (Banks et al., 2022; Bernstein et al., 2022; Roer et al., 2021) and with less involvement in health behaviors (Berk-Clark et al., 2018). This result adds complexity to the understanding of how PTSD interacts with health behaviors and suggests that PTSD may influence these behaviors indirectly, highlighting the need for further investigation into the specific pathways through which PTSD affects health behaviors. However, our findings related to childhood sexual abuse and the greater severity of IPV related to sexual coercion in health behaviors are consistent with prior studies showing that childhood trauma and IPV victimization decrease engagement in health behaviors and increase risky behaviors (Campbell et al., 2016; Ogden et al., 2022; Webster, 2022). It is known that IPV is a predictive experience for involvement in health risk behaviors (Teixeira et al., 2022) potentially driven by the emotional distress associated with their clinical condition, which may be alleviated through unhealthy behaviors (Mehr et al., 2023). Indeed, some argue that the negative health outcomes for victims may be linked to their involvement in pathogenic behaviors (Hoerster et al., 2019; Teixeira et al., 2022; Weiss et al., 2017), which contribute to various physical illnesses (Hoerster et al., 2019; Stubbs & Szoeke, 2021). In this context, it is also important to evaluate whether the reverse relationship exists and if it can lead to improvements in the overall health of women. Regarding childhood sexual abuse, it is important to consider the study by Campbell and colleagues (2016), which found that, among the types of abuse, childhood sexual abuse was most strongly associated with lower engagement in health behaviors and a greater adoption of risk behaviors, in contrast to physical and emotional abuse. The results of Hailes and colleagues (2019) reinforce this by linking sexual abuse to 93% of the assessed psychosocial, clinical, and physical health consequences, highlighting the critical role of sexual abuse. These findings emphasize the specific and devastating impact of different types of abuse, with sexual abuse being the most harmful, as it not only predicts low engagement in health behaviors but also contributes to PTSD symptoms. Prioritizing school intervention programs that focus on recognizing and reporting sexual abuse among children is essential. Integrating childhood abuse screenings within primary healthcare and offering educational initiatives for families, alongside coordination with other practitioners, can significantly mitigate the adverse effects of such abuse and promote better future outcomes (Hailes et al., 2019).
Finally, the results also showed that women victims of IPV experienced more physical/emotional and sexual abuse during childhood, had greater severity of PTSD symptoms and engaged less in health behaviors, compared to non-victimized women. These data corroborate the findings of other studies that found women victims of abuse in adulthood tend to have higher levels of childhood physical/emotional abuse and childhood sexual abuse (Costa et al., 2019), greater PTSD symptomatology (Costa & Botelheiro, 2020), and lower scores on engagement in health behaviors (Teixeira et al., 2022). The differences observed highlight the need to focus attention on women with a history of childhood abuse to prevent revictimization (Costa et al., 2019) and emphasize the need for interventions that raise awareness and promote health behaviors among IPV victims (Stubbs & Szoeke, 2021).
Given that traumatic childhood experiences increase vulnerability to accumulating risk factors, and that sexual abuse is a significant risk factor for revictimization through coercion or sexual assault throughout women’s life cycles (Jaffe et al., 2022), it is critical to address the long-term impact of these experiences on health behaviors. These experiences can lead to the adoption of risky behaviors, which tend to persist once established (Ferreira et al., 2018). Therefore, developing public policies that mitigate the adverse effects of these traumas and address them from an early age is essential, ultimately restoring individuals’ ability to proactively seek health. The results of the present study also highlight the need to prioritize interventions for women exposed to IPV, as they seem to carry with them other victimization experiences that should also be addressed, while the clinical and psychosocial variables present should also be assessed, since it was found in the present study that these women have higher PTSD symptomatology scores and adopt health behaviors less often, compared to non-victimized women.
Despite the results, several limitations should be noted. The retrospective nature of the questionnaires may impair recall in some cases, and self-reports could be influenced by social desirability. The study design does not allow for establishing causal relationships between variables. Additionally, data collection occurred during the pandemic, which may have affected responses. The sample size and failure to consider other childhood traumas - such as witnessing parental intimate partner violence or exposure to collective violence - are also limitations. Finally, the significant differences between the groups of women who are victims and non-victims of intimate partner violence may have impacted the results.
Future studies should prioritize longitudinal designs. This study demonstrates the influence of childhood trauma and IPV on health behaviors, making it imperative to analyze different types of abuse in relation to various health behaviors rather than treating health behaviors as a single variable. Additionally, investigating the mediating effects of childhood trauma between IPV and PTSD or health behaviors could provide valuable insights into these relationships. Incorporating psychobiological markers may further elucidate the underlying mechanisms. It is also important to understand the number of abusive relationships experienced by IPV victims and to include male participants in future studies. This inclusion is essential to contributing to the discussion on gender asymmetry in the context of IPV.
Furthermore, the absence of IPV screening in healthcare settings highlights a significant disconnect from established needs. Therefore, measures should be adopted to integrate IPV screening into routine practice, ensuring that care becomes more accessible and that prevention and intervention can occur more effectively.

