











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Suicide is defined as death caused by self-directed behavior intended to end one’s own life (American Psychiatric Association [APA], 2013). According to the World Health Organization (WHO, 2023), around 800.000 people die by suicide worldwide each year, which equals one death every 40 seconds. In Portugal, it is estimated that three people die by suicide daily (Ordem dos Psicólogos Portugueses [OPP] 2022).
The reasons for suicide are numerous and complex (O’Connor & Nock, 2014). Suicidal ideation, the act of thinking, considering, or planning one’s own death (APA, 2013), is a strong predictor for suicide and suicide attempts (WHO, 2023). In fact, about one in four individuals with suicidal ideation will attempt suicide (Jacobs, 2003). More specifically, in Europe, the lifetime prevalence of suicidal ideation is 20.27% for a wish to be dead, 9.08% for thinking about suicide, and 2.13% for planning suicide (Castillejos et al., 2020).
The WHO (2023) considers suicide a public health issue, advising for an urgent need for its prevention, including effective psychological assessment and intervention. However, globally, around 40% of people who died by suicide visited an emergency department one year before their death (Xanthopoulou et al., 2021). This indicates potential gaps in suicide risk assessments or missed intervention opportunities in at-risk patients (Ronquillo et al., 2012). For instance, most patients who refer suicidal ideation do not receive subsequent follow-up care (Kemball et al., 2008).
Previous studies (Airey & Iqbal, 2022; Jobes & Maltsberger, 1995; Roy et al., 2017) explored physicians’ experiences with suicide risk assessment in emergency departments, concluding that this is a highly anxiety-provoking task for professionals, leading to judgment errors and decreased confidence. Similarly, psychiatrists in primary and secondary healthcare often find discussing suicidal ideation uncomfortable, influencing patient’s responses towards not reporting suicidal ideation (Ford et al., 2020; McCabe et al., 2017).
While psychologists play a key role in suicide risk assessment and intervention (Groth & Boccio, 2018), to our knowledge, only one study (Dubue & Hanson, 2020) has explored their experiences regarding suicide risk assessment. The authors found that, when assessing suicide risk, psychologists often rely on intuition rather than formal guidelines or protocols, face emotional difficulties, and report a need for additional supervision and academic training. Furthermore, as far as we know, no study has investigated psychologists’ experiences regarding suicide intervention.
Therefore, this study aimed to explore the experiences and perceptions of a group of Portuguese psychologists regarding intervention in suicidal ideation, focusing on their strategies, difficulties, and needs.
Method
Participants
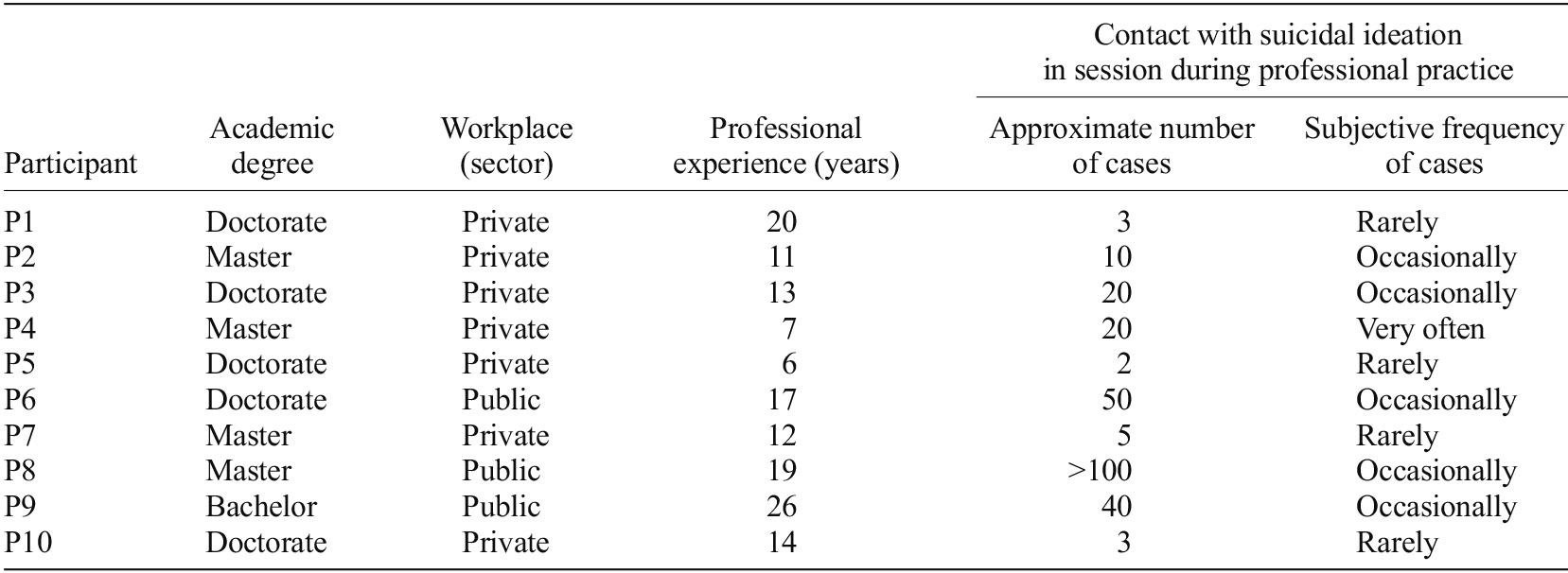
Ten clinical psychologists participated in this study, aged 31 to 49 years (M = 40.1, SD = 5.7), with eight (80%) identifying as women. Participants’ academic degree, workplace sector, professional experience, and contact with suicidal ideation during professional practice are detailed in Table 1. Inclusion criteria were (a) being a clinical psychologist, (b) having experience with suicidal ideation cases, and (c) speaking Portuguese.
Instruments
Sociodemographic and Professional Experience Questionnaire. Collected data on age, gender, academic degree, workplace sector, years of professional experience, number of suicidal ideation cases treated, and frequency of interaction with suicidal ideation patients (1 = Rarely to 4 = Very often).
Semi-structured Interview. The interview script was developed specifically for this study, including open-ended questions (Donalek, 2005) about intervention in suicidal ideation, covering the dimensions: (a) methods (e.g., “How do you usually carry out intervention in suicidal ideation?”), (b) acquisition of knowledge during university (e.g., “Do you consider that the training you received at university was useful/sufficient to know how to intervene in suicidal ideation?”), (c) difficulties (e.g., “What are the main difficulties/obstacles you encounter when intervening in suicidal ideation?”), (d) feelings (e.g., “How do you feel when intervening in suicidal ideation?”) and e) aspects to improve (e.g., “What do you think could be improved in your intervention in suicidal ideation?”).
Procedure
This study was approved by the Ethics Committee for Research in Social and Human Sciences (CEICSH) of the University of Minho. Initially, a pilot study was conducted with two psychologists, resulting in a reduction and restructuring of the questions in the script. Then, participants were recruited from clinics, hospitals, and universities, using the non-probability criterion sampling technique, for convenience (Carmo & Ferreira, 2008). All received an email outlining the study’s purpose and requesting their participation.
Data collection occurred between December 2022 and February 2023. Recruitment ceased upon reaching data saturation (Fusch & Ness, 2015), in the 10th interview. Those who agreed to participate were provided with a Google Forms link to complete the informed consent. Each participant was assigned a code to preserve anonymity. Once consent was obtained, the link directed them to the sociodemographic and professional experience questionnaire.
Interviews were conducted online, via Zoom. Prior to each interview, the interviewer provided an overview of the study’s aim and structure. The interviews lasted between 40 and 100 minutes (M = 55, SD = 17.5). At the conclusion, participants were asked if they had any questions. All interviews were audio and video recorded, destroyed after the transcription of the interviews.
Data analysis
Thematic analysis was used to identify and establish patterns of meaning (themes) in the data (e.g., interviews; Braun & Clarke, 2006). Within thematic analysis, an inductive approach was adopted (coding process where codes emerge from the content of the data), as well as an essentialist paradigm, since the focus was to understand participants’ experiences and perceptions of reality (Braun & Clarke, 2006).
The analysis followed the six steps of thematic analysis from Braun and Clarke (2012), where interviews were transcribed verbatim (Schegloff, 1997) using Microsoft Word 365 software. Secondly, initial codes were generated, reducing the information from the interviews into pieces of meaning, using Taguette software (Rampin et al., 2021). In the third phase, the coded data was combined and organized into broader themes. In the fourth and fifth phases, potential themes and subthemes were reviewed and thematic maps were generated. Finally, the final themes were defined to address the research question. The sixth and final step involved writing up the findings.
Methodological integrity
To ensure qualitative rigor, validation and reliability strategies were implemented (Cypress, 2017). Another author reviewed the coding of 30% of the interviews to ensure consensus and consistency. Likewise, the data was recoded several times, spaced apart (Castleberry & Nolen, 2018). Special care was ensured at all stages of the analysis and the data was meticulously transcribed. Additionally, feedback on the data analysis was requested at different stages from members of a research group, to reach consensus on the codes and themes (Morse, 2015). Detailed descriptions of findings, including interview’s excerpts, were provided to support the findings (Cypress, 2017).
Findings
The analysis of the interviews resulted in one theme: Intervention in suicidal ideation, which addresses participants’ experiences and perceptions regarding how they conduct intervention in suicidal ideation, as well as their difficulties and needs. This theme encompassed three subthemes: Different Intervention Strategies in Suicidal Ideation, Obstacles and Difficulties in Suicidal Ideation Intervention, and Improvements and Needs in Intervention in Suicidal Ideation. Each subtheme is represented by a thematic map and described in detail, supported by direct quotes from participants to ground the interpretation in the data.
Different intervention strategies in suicidal ideation
This subtheme refers to the strategies used by the participants when intervening in suicidal ideation (see Figure 1). All participants described their main goal while intervening in suicidal ideation is to prevent future situations. One participant noted, ‘So that we can intervene to prevent new situations arising from this ideation’ (P8).
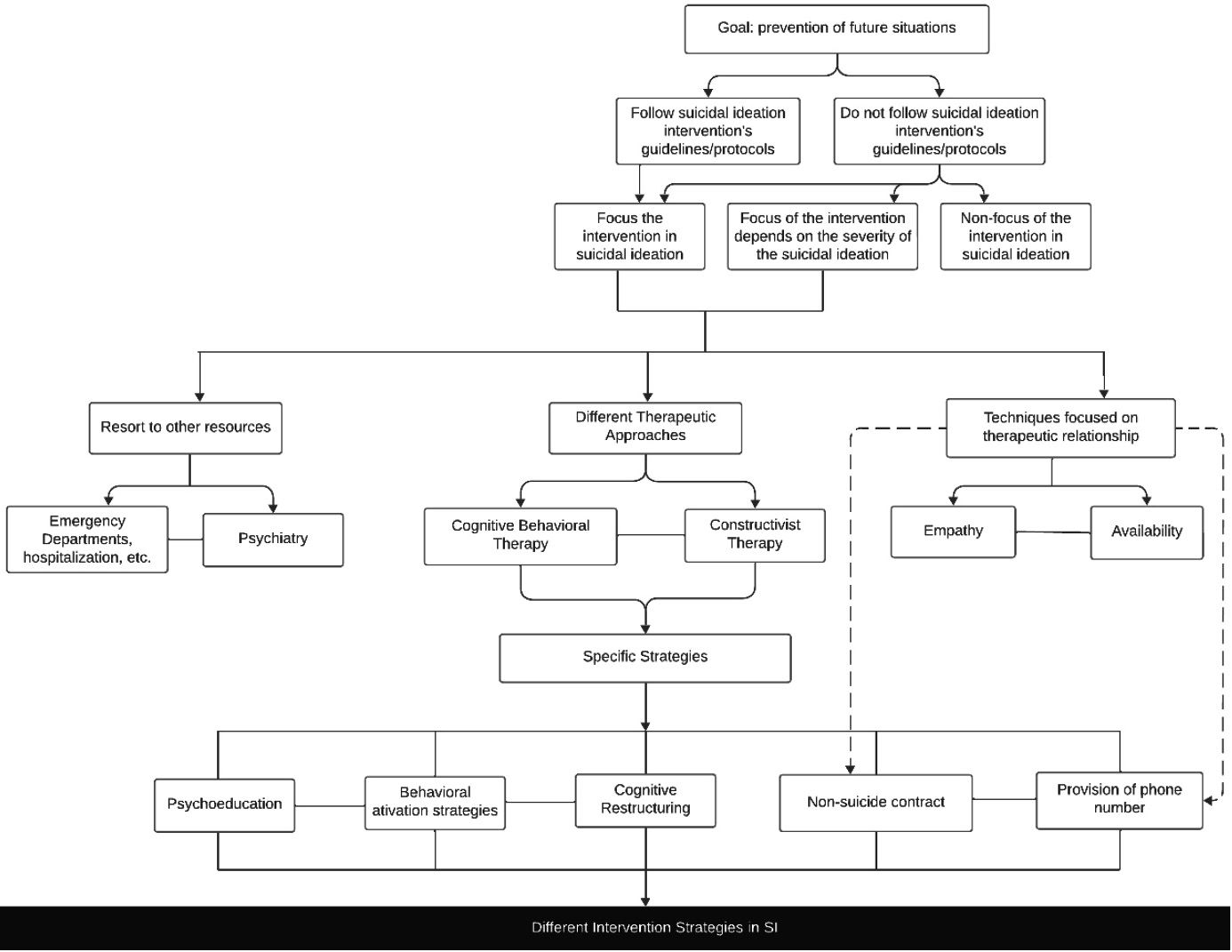
Few participants mentioned following intervention guidelines/protocols, while the remaining did not. As stated by P3, ‘I follow generic guidelines’, and by P7, ‘Nothing very structured, specific’.
When suicidal ideation is present, some participants mentioned focusing the intervention specifically in suicidal ideation. As expressed by P3, ‘From the moment there’s suicidal ideation, I’ll immediately respond to it’.
Some participants reported they focus the intervention on suicidal ideation only if it is structured (with a plan), or if the patient is suffering, otherwise, they choose to intervene in other symptoms/factors. According to P4, ‘If we address burnout first, for example, suicidal ideation will be minimized because we no longer have that symptomatology’. Contrary to the previous participants, one participant mentioned not focusing the intervention on suicidal ideation itself, ‘I think if we spend an entire session just talking about ideation, we’re there... I try to focus more on the person’s strengths’ (P6).
Those who reported focusing their intervention on suicidal ideation mentioned using different strategies, adapting the intervention to the characteristics of each case. As explained by P2, ‘There are specificities of the case that I may have to attend to and adapt’. Most of these participants reported seeking help from other professionals. Depending on the suicide risk (e.g., existence of a plan), some highlighted the need to resort to other resources (e.g., emergency department, hospitalization, etc.). In the words of P3, ‘We need to seek patient stabilization. This isn’t about psychotherapy. It is an articulation with the national health system’. In parallel, most participants mentioned articulating with psychiatry, and, in some cases, complementing their intervention with psychotropic drugs. One participant remarked, ‘I always coordinate with the psychiatrist to work together’ (P3).
Regarding the specificities of psychological intervention, all participants who focus on intervening in suicidal ideation mentioned basing it on therapeutic approaches. Most mentioned using Cognitive Behavioral Therapy (CBT) and the remaining Constructivist Therapy. A participant shared, ‘I work with the cognitive behavioral approach, and I don’t change it in these cases to another’ (P3).
Based on the mentioned approaches, most participants reported providing psychoeducation. As emphasized by P2, ‘Make the person understand how the mind works and why these thoughts are going through their mind’. Moreover, most participants mentioned using behavioral activation strategies and cognitive restructuring, so that the patient can learn how to deal with their thoughts and adopt more adaptive emotional regulation strategies. As mentioned by P8, ‘Activation of more adaptive coping strategies to manage the problems’, and by P1, ‘Trying to make her understand how this desire to end her life was an expression of great suffering’.
In parallel with these strategies, most participants reported making a non-suicide contract with the patient. The remaining referred disagreeing with its use. One participant stated, ‘I prepare an anti-suicide contract with the patients’ (P4), while other noted ‘I still remember the time when we had to give them the non-suicide contract, which’s no longer considered a strategy for dealing with it’ (P6). Simultaneously, most participants mentioned providing their phone number to monitor the patient’s condition between sessions and for patients’ use in emergencies. According to P1, ‘I give my phone number for emergencies. I think it’s a gesture towards the person to show that someone cares.
Alongside the use of these strategies, most participants mentioned adopting techniques that prompt the therapeutic relationship, as they consider it the main factor for therapeutic success, demonstrating empathy and availability towards the patient. As mentioned by P1, ‘The important thing is that the person felt understood and what we talked about helped her to vent what she was feeling’.
Obstacles and difficulties in suicidal ideation intervention
This subtheme refers to obstacles in suicidal ideation intervention identified by participants (see Figure 2). All participants mentioned the existence of gaps in academic training, which some of them felt that contributed to a lack of knowledge on how to intervene in suicidal ideation. As shared by P10, ‘I never addressed suicide at any moment during university and when we are ‘thrown to the lions’ like this, there can be difficulties’, and by P5, ‘I have some ignorance in dealing with thoughts around ending one’s life’.
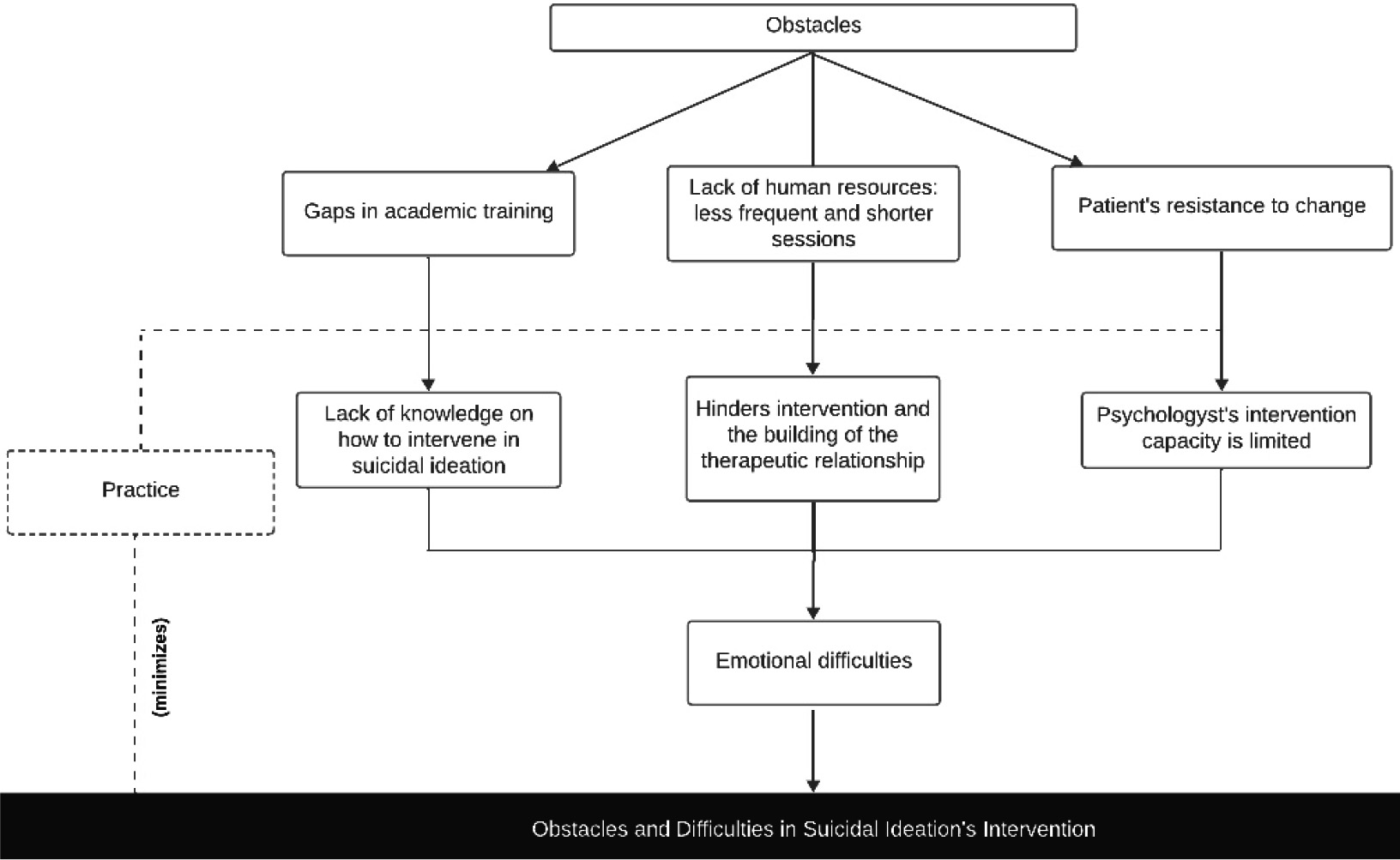
Figure 2 Thematic map of the subtheme “Obstacles and difficulties in suicidal ideation intervention”
Another obstacle observed by most participants was the lack of human resources in the services, which implies less frequent and shorter sessions that hinder intervention and the building of the therapeutic relationship. In the words of P8, ‘We don’t have enough human resources to be able to dedicate ourselves only to this area of intervention in suicide risk’, and P9, ‘A follow-up every 3 or 6 months isn’t effective’.
Most participants also noted that these cases are resistant to change, which presents an obstacle and leads them to believe that their intervention’s capacity is limited. As stated by participants, ‘The motivational level of these patients is very low’ (P5), ‘I think if the person has a very strong desire to do something, not even the best psychologist in the world will be able to dissuade him’ (P1).
The mentioned obstacles were referred by all participants as generating emotional difficulties for them (e.g., tension, discomfort, anxiety, impotence, etc.) when dealing with suicidal ideation and with potential negative consequences of their intervention. As remarked by P5, ‘It’s not a population I feel comfortable working with, at all.’.
Most participants also mentioned the importance of practice, which helps to minimize difficulties in intervention over time. As referred by P5, ‘Practice makes all the difference. Practice is fundamental, in my opinion’.
Improvements and needs in intervention in suicidal ideation
This subtheme addresses the needs identified by the participants to mitigate their difficulties and improve intervention in suicidal ideation (see Figure 3). All participants reported considering it is essential that psychologists are prepared to know how to intervene in a case of suicidal ideation. As observed by P4, ‘If we know how to intervene, or simply direct, we are doing much of what is expected of and helping people’.
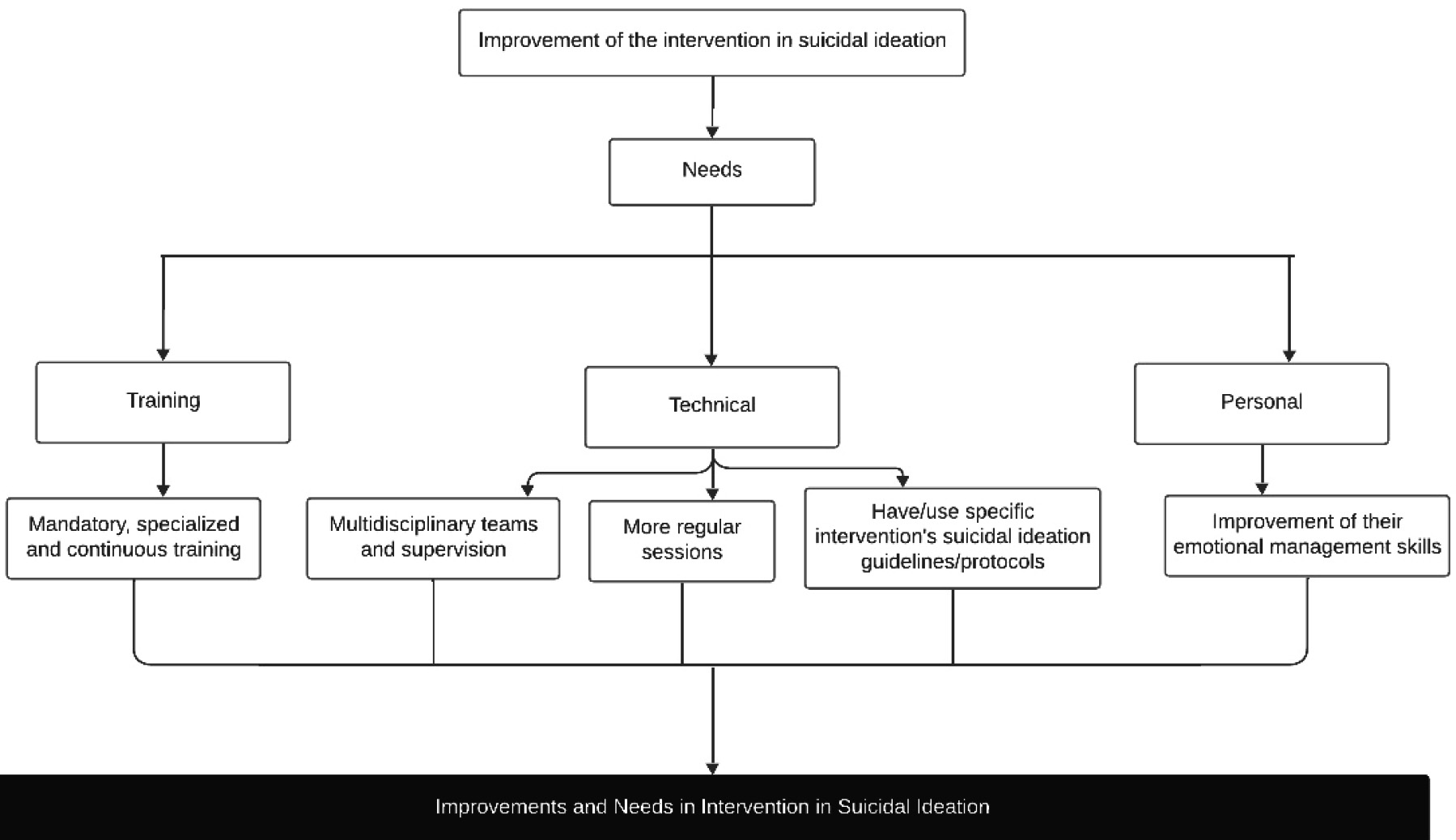
Some participants identified a need for mandatory and ongoing specialized training in suicidal ideation intervention for all psychologists. As explained by P5, ‘I think it should be mandatory training for all clinicians, given the risk that is being taken in relation to people’s lives’. In addition, some participants indicated technical needs, such as integrating multidisciplinary teams, i.e., articulating, in a more accessible way, with the emergency department and psychiatry, and having supervision. Participants also mentioned the need for more regular sessions, and specific intervention guidelines/protocols that they could follow. As suggested by participants, ‘Having a ‘fast track’ in relation to psychiatry (...) there must be common work between psychology and psychiatry and emergency department’ (P7), ‘We would like to have more regular sessions’ (P8), ‘Giving clearer guidelines on how to deal with these situations’ (P2).
Most participants mentioned personal needs, such as needing to improve their emotional management skills, as it affects the therapeutic relationship. As stated by P2, ‘I need to improve this part of becoming concerned/distressed, because that can be passed to the person and may not be the best’.
Discussion
This study aimed to explore the experiences and perceptions of a group of Portuguese psychologists about their practice in suicidal ideation intervention. Regarding intervention strategies, few participants follow intervention guidelines/protocols and focus the intervention directly on suicidal ideation. Furthermore, most only address suicidal ideation if it is structured or if there is significant suffering. Clay (2022) emphasizes always prioritizing suicidal ideation in intervention, due to its strong predictor role in suicide risk (WHO, 2023).
Additionally, participants refer resorting to other professionals, especially the emergency department (in cases of structured suicidal ideation) and psychiatry, whenever possible, and sometimes complementing their intervention with psychotropic drugs. Indeed, research (e.g., Jacobs & Brewer, 2004) shows that combining psychotherapy and psychopharmacology (especially antidepressants) seems to be the best strategy to reduce suicidal ideation.
CBT is adopted by most participants, who mentioned techniques such as psychoeducation, behavioral activation, and cognitive restructuring. In fact, CBT has shown promising results in providing patients with new thought patterns and improving their emotional regulation strategies, making suicide no longer perceived as the only solution to problems (e.g., Jobes, 2020). Most participants also mentioned using non-suicide contracts, while some referred not agreeing with its use. Several studies (e.g., Betz et al., 2016) argue this contract lacks scientific evidence and is not effective in suicide prevention, as it may reduce vigilance over the patient’s risk.
The literature also supports Dialectical Behavioral Therapy as an effective approach (e.g., Mann et al., 2005), however, no participant in this study reported using it. Although these therapies have a positive effect on reducing suicidal ideation, there does not seem to be an approach that addresses suicidal ideation alone (Klonsky et al., 2016).
All participants identified the existence of gaps in academic training for suicidal ideation intervention. Therefore, it may be relevant to introduce this training into academic programs. Obstacles such as the patients’ resistance towards change were also mentioned, making participants feel their intervention capacity is limited. However, OPP (2022) suggests that people with suicidal ideation feel ambivalent - on the one hand, they see no alternative, on the other hand, they want to be helped -, which opens possibilities for intervention effectiveness. All participants also reported feeling emotional difficulties when intervening in these cases, which hinder their ability to intervene.
Furthermore, participants mentioned the importance of practice in minimizing their difficulties in intervening over time. While experience alone may contribute to greater competence and self-efficacy, deliberate practice may also help psychologists develop more effective strategies for managing demands and stress (Dorociak et al., 2017), thereby enhancing their competence and self-assurance.
Participants also mentioned the need for specialized and mandatory continuous training in suicidal ideation intervention for all psychologists, as they report feeling gaps in academic training. Likewise, they suggested the integration of psychologists into multidisciplinary teams, with a “fast track” to emergency departments, psychiatry, and supervision. This was also mentioned in Dubue and Hanson (2020) study, and seems important, especially in the private sector, as psychologists may have more difficulties referring their clients to these services.
Moreover, participants expressed the need for specific intervention guidelines/protocols, and more frequent sessions with these patients. Although OPP (2022) recommends frequent sessions to monitor suicide risk, public sector psychologists face difficulties due to the lack of human resources.
The therapeutic relationship was mentioned by participants as crucial for therapeutic success and is emphasized by the literature (e.g., Xanthopoulou et al., 2021) as the greatest predictor of therapeutic success with patients with suicidal ideation. Moreover, considering that there does not exist a single approach that, by itself, addresses suicidal ideation (Klonsky et al., 2016), focusing on building and maintaining the therapeutic relationship may be relevant. In fact, participants highlighted the need to improve emotional management to avoid transmitting negative emotions to patients and impairing the therapeutic relationship.
Limitations and future research
This study presents limitations, such as the participant’s heterogeneity in terms of workplaces and years of professional experience, which may have affected the gain of in-depth knowledge of the specifics of the intervention process. Additionally, the imbalance between the public and private sectors may have skewed our findings towards the private sector and limited our ability to identify sector-specific patterns. Future studies should analyze some aspects noted in the findings with a contrasting lens (e.g., between psychologists in public and private sectors). Moreover, replicating this study with suicidal ideation patients could provide insights into their experiences, perceptions, needs, and what intervention strategies work best for them.
Implications
This study is, to our knowledge, the first qualitative research, in Portugal, to explore mental health professionals’ experiences and perceptions about intervention in suicidal ideation and the first study, worldwide, to explore psychologists’ perspectives. Important recommendations can be outlined for psychologists, psychological associations, and healthcare services, which can address the difficulties and needs recognized in this study, enhancing psychologists’ resources and self-efficacy, ultimately improving clinical practices on suicide prevention. Namely, specialized training and specific guidelines/protocols should be developed and made accessible to psychologists at all levels of training and practice. These should emphasize the need to address and prioritize suicide risk assessment and treatment (Clay, 2022). Furthermore, integration of psychologists in multidisciplinary teams should be supported, employing ‘fast track’ to emergency departments, psychiatry, and supervision, especially in the private sector. In addition, services must ensure regular therapy sessions, which could be addressed by increasing human resources. Lastly, self-care is a professional imperative for psychologists (Ziede & Norcross, 2020). Thus, self-care practices, personal therapy, and supervision should be made available to psychologists to promote and maintain their well-being and that of those they support in their practice.
Conclusion
This study explored the strategies, difficulties, and needs faced by a group of psychologists in intervening with suicidal ideation. It highlights the lack of specific guidelines/protocols, leading to the implementation of random and loose strategies (some that align with the literature and others that do not). It also outlines an emphasis on techniques to build the therapeutic relationship. Key obstacles identified include gaps in academic training, patient’s resistance to change, and a lack of human resources, which prompt emotional difficulties in psychologists and hinder suicide intervention. This research also underscores the need for continuous and specialized training, the implementation/development of evidence-based guidelines/protocols, the integration of psychologists in multidisciplinary teams, and an increase of supervision and human resources in services. A patient’s suicide is the most catastrophic outcome, in a clinical context, for a psychologist (Airey & Iqbal, 2022). It is truly crucial to promote better practices in suicide intervention and therefore in psychologists’ training and well-being.

