











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
The COVID-19 pandemic has been found to be globally associated with multiple deleterious effects on mental health outcomes (Arslan et al., 2020), particularly amongst frontline healthcare professionals (Lai et al., 2020; Maben & Bridges, 2020).
While fulfilling their professional duties, nurses often engaged in closer proximity with COVID-19 confirmed cases. This increased exposure to the coronavirus significantly heightened the fears of contracting the disease, and inadvertently transmitting it to their significant others (Chen et al., 2021; Kisely et al., 2020; Lai et al., 2020; Maben & Bridges, 2020). Additionally, this group also faced a sudden overwhelming surge of workload, and a consecutive witnessing of escalating rates of morbidity and mortality associated with the coronavirus. Simultaneously, these healthcare professionals were also confronted with a series of professional burdens and challenges, such as: depletion of workforce, due to infection and self-isolation, scarcity of personal protection equipment, insufficient specific medical supplies, and inadequate support from their employers (Kisely et al., 2020; Lai et al., 2020; Maben & Bridges, 2020). Other factors, such as adjusting to new protocols, witnessing the suffering, and passing of a higher number of patients, fatigue, communication barriers, and stigma were also present (Maben & Bridges, 2020). Altogether, these factors may have contributed to rising levels of anxiety, depression, stress, insomnia, overall psychological distress (Kisely et al., 2020; Lai et al., 2020) and trauma symptoms (Chen et al., 2021). Findings also suggest that, when compared to other healthcare professionals, younger women, who were frontline nurses during the COVID-19 pandemic, were at a higher risk of developing worse psychological outcomes (Chen et al., 2021; Lai et al., 2020).
The traumatic nature of the COVID-19 pandemic outbreak
The definition of a traumatic event includes exposure to scenarios of death, or threat of death, occurring within the context of performing professional duties (American Psychiatric Association [APA], 2022). As for post-traumatic stress symptoms (PTSS), these consist of recurrent feelings of intrusiveness (e.g., upsetting thoughts or memories), frequent dreams or nightmares about the traumatic event, and physiological responses (e.g., surge in heart rate when recalling the event). Negative changes in mood and cognition, hyperactivation and hyperreactivity when faced with stimuli related to the traumatic event, and persistent avoidance of such stimuli can also be present. Symptoms of dissociation can also manifest. These encompass the sense of reexperiencing the traumatic event (flashbacks), the sense of detachment from oneself (depersonalization) and the sense of detachment from one’s environment (derealization) (APA, 2022). Accordingly, the COVID-19 outbreak represented a potential large-scale traumatic event, which may have resulted in increased levels of trauma symptoms (Chen et al., 2021). However, PTSS do not always manifest following the experience of a traumatic event (Chen et al., 2021; Yang et al., 2022). When a traumatic event is highly centralized (Berntsen & Rubin, 2006; Boykin et al., 2020; Yang et al., 2022), and when a person has difficulties in adjusting their thoughts and behaviors in response to these experiences (Arslan et al., 2020; Levin et al., 2014), it can negatively affect their mental health outcomes, and lead to the development of PTSS.
The role of event centrality and psychological inflexibility on PTSS
Event centrality refers to the extent to which a memory becomes a core part of one’s identity, and a reference to build deriving inferences upon. In this sense, when a traumatic event becomes central to one’s identity, it can influence the attribution of meaning and future expectations to other unrelated events. This can then lead to rumination, unnecessary worries, and avoidance attempts (Berntsen & Rubin, 2006). As such, these traumatic memories may become readily accessible in the autobiographical memory, triggering post-traumatic cognitions, and potentially lead to PTSS (Berntsen & Rubin, 2006; Boykin et al., 2020; Yang et al., 2022). For instance, a study found that high levels of event centrality of a traumatic event were associated with poorer adjustment levels, including higher levels of PTSS (Boykin et al., 2020). In another study, high centrality of the COVID-19 outbreak was found to lead to the onset of PTSS among college students (Yang et al., 2022).
Additionally, psychological inflexibility is a transdiagnostic feature composed of six interrelated processes. These processes are cognitive fusion, experiential avoidance, loss of contact with the present moment, overattachment to the conceptualized self, unclear values, and absence of value-driven actions (Hayes et al., 2006). This construct manifests as a rigid cognitive-behavioral pattern, with the aim to control and avoid unpleasant internal and external experiences. However, paradoxically, this maladaptive strategy intensifies and increases the frequency of these unpleasant experiences over time, leading to increased levels of psychological impairment (Arslan et al., 2020; Hayes et al., 2006; Levin et al., 2014). Moreover, it has been associated with anxiety and depressive disorders, eating disorders, and PTSS (Boykin et al., 2020; Levin et al., 2014).
In a study with a sample of college students, moderate correlations were found between event centrality, psychological flexibility, and trauma outcomes (Boykin et al., 2020). In another study, findings revealed that nurses perceived the coronavirus outbreak as a stronger reference point than the general population (Vitorino et al., 2023), suggesting that nurses could be at a higher risk of developing PTSS, due to the high event centrality of the COVID-19 pandemic, and to the exposure to its associated stress factors.
The current study
The present study targeted a sample of Portuguese nurses to assess the centrality of the COVID-19 pandemic outbreak, on the development of PTSS among nurses, via psychological inflexibility.
The literature has found evidence that frontline nurses have been significantly affected by the coronavirus outbreak and are at risk of developing deleterious psychological outcomes (Chen et al., 2021; Kisely et al., 2020; Lai et al., 2020; Maben & Bridges, 2020; Vitorino et al., 2023). However, despite these insightful contributions, research has yet to explore the mediating role of psychological inflexibility between the centrality of the emergence of the COVID-19 pandemic and PTSS in nurses, who were frontline workers during this outbreak.
Therefore, this study sought to: firstly, explore the relationship between the centrality of the emergence of the COVID-19 pandemic, psychological inflexibility, and PTSS in nurses; and, secondly, to examine the direct and indirect effects, via psychological inflexibility, of the centrality of the emergence of the COVID-19 pandemic, on PTSS in nurses.
Accordingly, two hypotheses were proposed in the current study: (1) a higher centrality of the emergence of the COVID-19 pandemic would be associated with greater psychological inflexibility levels, which would be associated with heightened levels of PTSS among nurses; and (2) psychological inflexibility would mediate the association between the centrality of the emergence of the COVID-19 and PTSS in nurses.
Method
Participants and procedure
This quantitative, cross-sectional, and correlational study is a part of a larger research project titled “Large-scale, longitudinal documentation of the impact of COVID-19 on mental health and wellbeing across Portuguese nurses and their families” (2020.07981.BD). The larger research project was approved by the Ethics Committee of the Faculty of Psychology and Educational Sciences of the University of Coimbra (CEDI - 21.04.2021). All procedures were in accordance with the ethical standards of the institutional research committee and with the Declaration of Helsinki (World Medical Association, 2013).
The project was publicized through social media, such as Facebook and Instagram. To facilitate the dissemination of the project, a collaboration protocol was formally established with the Portuguese Order of Nurses. Additionally, the Nursing Schools of Lisbon and Coimbra, and nursing Unions were contacted to publicize the project among their associate members.
The data for this study was exclusively collected via online self-report questionnaires, through the LimeSurvey® platform, starting on the 14th of September 2021 and finishing on the 2nd of June 2022. The forced answering strategy was employed to prevent missing values (i.e., respondents had to answer each question to proceed through the questionnaire). Seriousness check questions were incorporated to ensure participants’ involvement and to improve data validity (e.g., “is white a fruit?”) (Aust et al., 2012). Additionally, participants’ e-mail addresses and IP addresses were screened to guarantee there were no automatic survey-takers and to ensure bot detection (Bybee et al., 2022; Godinho et al., 2020; Storozuk et al., 2020).
On the first page of the survey, all participants were informed of the objectives, procedures, and the voluntary and anonymous nature of the study. After reading this information, participants gave their informed consent. No compensation was given for participating in this study. Privacy and data protection were in accordance with the European Union’s General Data Protection Regulation (GDPR). Only the core research team involved in the project had access to the database.
The inclusion criterion defined for the selection of the sample was to be a nurse working in Portuguese hospitals or primary healthcare institutions. The total sample of this study consisted of 672 Portuguese nurses, mean age 39.1 (SD = 9.68), with 92% women (n = 618), 7.9% men (n = 53) and .1% non-binary (n = 1). Detailed sociodemographic and clinical information is available in the Results section.
Measures
Sociodemographic and Clinical Questionnaire. This questionnaire was developed within the larger research project and includes questions about sociodemographic characteristics (e.g., age, gender), clinical data (e.g., psychological/psychiatric treatment history), and the level of exposure to COVID-19 disease (e.g., “Were you diagnosed with COVID-19?”, “Were you isolated from your close family?”).
Centrality of Event Scale (CES; Berntsen & Rubin, 2006; Matos et al., 2010). This unidimensional instrument aims to assess to what extent a memory has become a reference point for future inferences. In this study, participants were asked to “Think about the COVID-19 outbreak”. This scale consists of 20 items (e.g., “I feel that this event has become part of my identity”; “When I reflect upon my future, I often think back to this event”), each of which is rated on a 5-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree). The scores can vary from 20 to 100 points, where higher scores indicate a higher memory centrality. In the absence of a formally established cutoff score for the CES, the median value was used to aggregate the scores of the sample, as performed by Matos and colleagues (2010). As such, the cutoff score for this study was established at 62 points. In the present study’s sample, the scale demonstrated excellent internal consistency levels (ω = .95; α = .95).
Acceptance and Action Questionnaire-II (AAQ-II; Bond et al., 2011; Pinto-Gouveia et al., 2012). This unidimensional questionnaire measures the levels of experiential avoidance and psychological inflexibility. This questionnaire contains 7 items (e.g., “Emotions cause problems in my life”; “My painful memories prevent me from having a fulfilling life”). Each item is evaluated on a 7-point Likert scale, ranging from 1 (never true) to 7 (always true). Total scores can range from 7 to 49 points, with higher values indicating the presence of higher levels of experiential avoidance and psychological inflexibility. Cutoff scores are suggested between 24 and 28 points (Bond et al., 2011), or between 28 and 32 points (Ong et al., 2018). A cutoff score of 32 points was employed in the present study to maximize specificity (Ong et al., 2018). In the current study, this questionnaire revealed an excellent internal consistency (ω = .95; α = .95).
Impact of Event Scale-6 (IES-6; Lopes, 2013; Thoresen et al., 2010). This unidimensional scale assesses symptoms of intrusiveness, avoidance/dullness and hypervigilance related to post-traumatic stress disorder. This scale is composed by 6 items (e.g., “I felt watchful or on-guard”; “I tried not to think about it”). All items are rated on a 5-point Likert scale, ranging from 0 (never) to 4 (extremely). The total scores can vary from 0 to 35, with higher the scores indicating a greater impact of an event (in this case, of the COVID-19 pandemic). The cutoff score for the Portuguese population was established at 12.5 points (Lopes, 2013). In the present study the cutoff was established at 13 points. In this study, this instrument presented good levels of internal consistency (ω = .87; α = .86).
Data analysis
The sample dimension required to detect small to medium size effects was determined by G*POWER (Faul et al., 2007, 2009) and Monte Carlo Simulation (Schoemann et al., 2017). According to these programs, 314 and 52 subjects were respectively required for correlational analyses by G*Power, and for mediational analyses by Monte Carlo Simulation.
The Statistical Package for Social Science (SPSS) for Windows, version 27 was used for the remaining statistical analyses. The reliability of the measures was assessed by calculating Cronbach’s alpha and McDonald’s omega coefficients. In both measures, values equal or above to .80 and .90 are, respectively, considered as good, and as excellent indicators of internal consistency (McNeish, 2018; Nunnally & Bernstein, 1994).
Pearson’s correlation coefficients were calculated to assess the strength and direction of the associations between the variables under study (objective 1), and to identify potential covariates. These associations were classified as weak (± .10 to ± .29), moderate (±. 30 to ± .49), or strong (± .50 to ± 1.0) (Cohen, 1988).
Regression-based mediation analyses were performed to assess the mediating effects of psychological inflexibility in the relationship between the centrality of the emergence of COVID-19 pandemic and PTSS (objective 2). The statistical significance of these effects was examined through PROCESS macro (Hayes, 2012, 2022), model 4, with 10000 bootstrap samples. This resulted in 95% bias-corrected and accelerated confidence intervals (BCaCIs) (Tabachnick & Fidell, 2007). Effect sizes were interpreted according to the values of R 2 , as small (R 2 ≥ .02), medium (R 2 ≥ .13) or large (R 2 ≥ .26) (Cohen, 1992). These effects were considered statistically significant at a p-value lower than .001, and as the value of zero was not contained within the confidence intervals.
In the present study, the variables were defined as follows: the centrality of the emergence of the COVID-19 pandemic as the predictor, psychological inflexibility as a mediating variable and post-traumatic stress symptoms (PTSS) as the outcome. Four variables presented significant associations with the outcome and were introduced into the model as covariates (Tabachnick & Fidell, 2007). These were sociodemographic and clinical variables, which were statistically controlled to account for their additional variability in the outcome (MacKinnon & Luecken 2008). Specifically, age (r = -.12, p < .01) and gender (r = -.10, p < .01) were significantly associated with PTSS. The correlations between previous psychiatric/psychological treatment history (r = -.26, p < .01) and prophylactic isolation away from significant others (r = -.14, p < .01) with the outcome were also significant. In the end, age, gender, previous psychiatric/psychological treatment history, and prophylactic isolation away from significant others were entered as covariates in this model.
Results
Sociodemographic and clinical characteristics
The total sample of this study consisted of 672 Portuguese nurses, distributed by several national services and hospital units. The age of the participants ranged from 21 to 65 years old (M = 39.09, SD = 9.68), most of the participants were women (n = 618, 92%), and 75% of the total sample had a degree (n = 504). A significant part of the participants had already resorted to mental health services for psychological/emotional problems (n = 315, 46.9%) and more than half have been in prophylactic isolation away from significant others (n = 396, 58.9%). About 51% of the sample surpassed the cutoff scores for COVID-19 event centrality (n = 342), nearly a quarter of these nurses presented high levels of psychological inflexibility (n = 159, 23.7%), and approximately a third of the participants exhibited PTSS (n = 191, 28.4%). The sociodemographic and clinical characteristics of the sample are detailed in Table 1.
Table 1 Sociodemographic and clinical characteristics of the participants
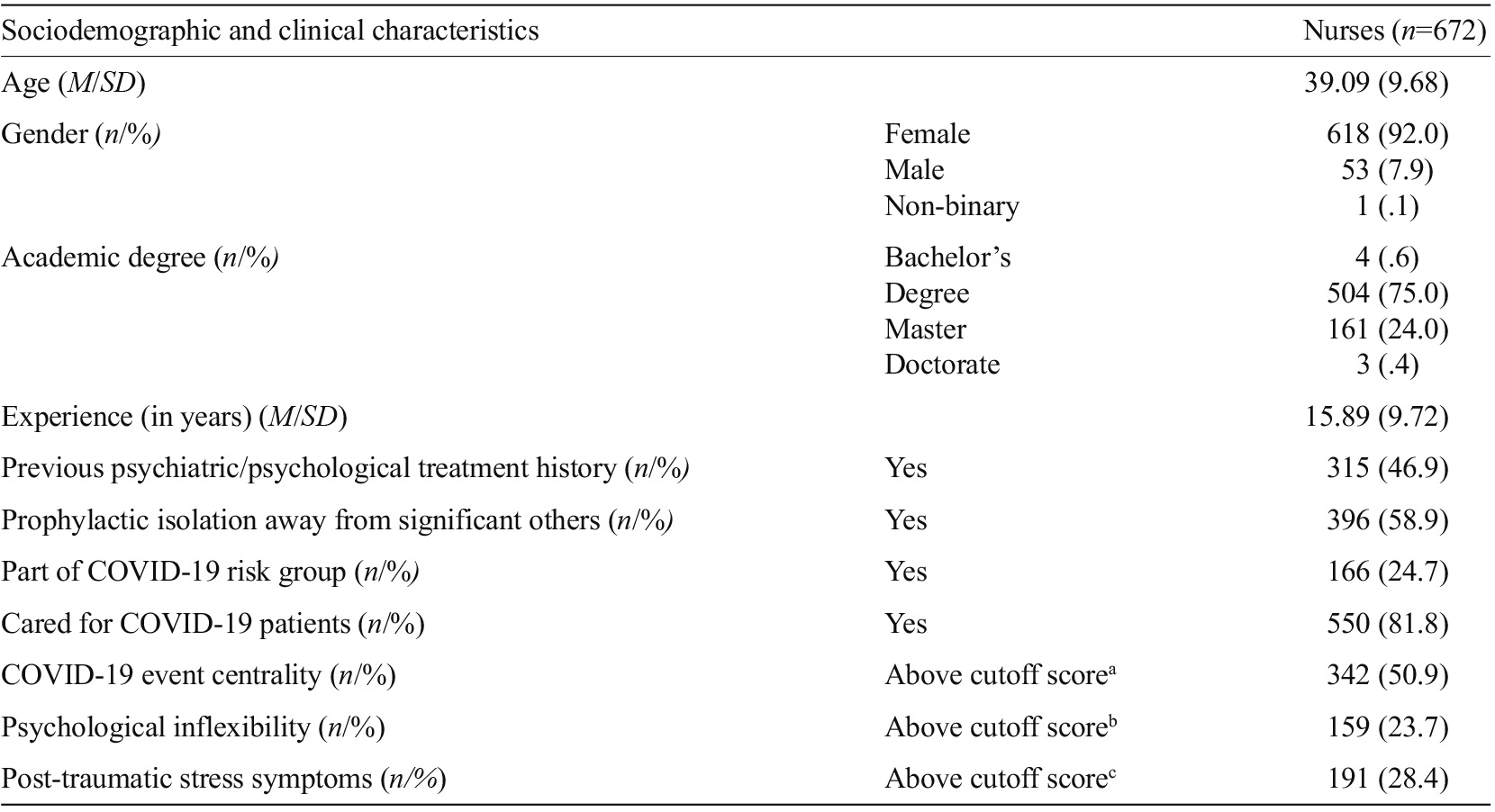
Note. The sample consists of 672 Portuguese nurses, who work in the main regions of the country; aThe cutoff score was considered at 62 points (median value in this study); bThe cutoff score was employed at 32 points for higher specificity; cThe cutoff score for the Portuguese population is established at 12.5. A score of 13 points was used as a cutoff point.
Correlations between variables
The centrality of the emergence of the COVID-19 pandemic displayed a strong and positive association with PTSS, and a moderate positive association with psychological inflexibility. There was also a strong positive association between psychological inflexibility and PTSS. Table 2 depicts the matrix of correlations between the variables under study, as well as their respective means and standard deviation values.

Mediation model
A simple mediation model was estimated to analyze whether the centrality of the emergence of the COVID-19 pandemic predicted PTSS in nurses, and whether psychological inflexibility mediated that relationship. The path model is depicted in Figure 1, and their respective unstandardized regression coefficients are present in Table 3.
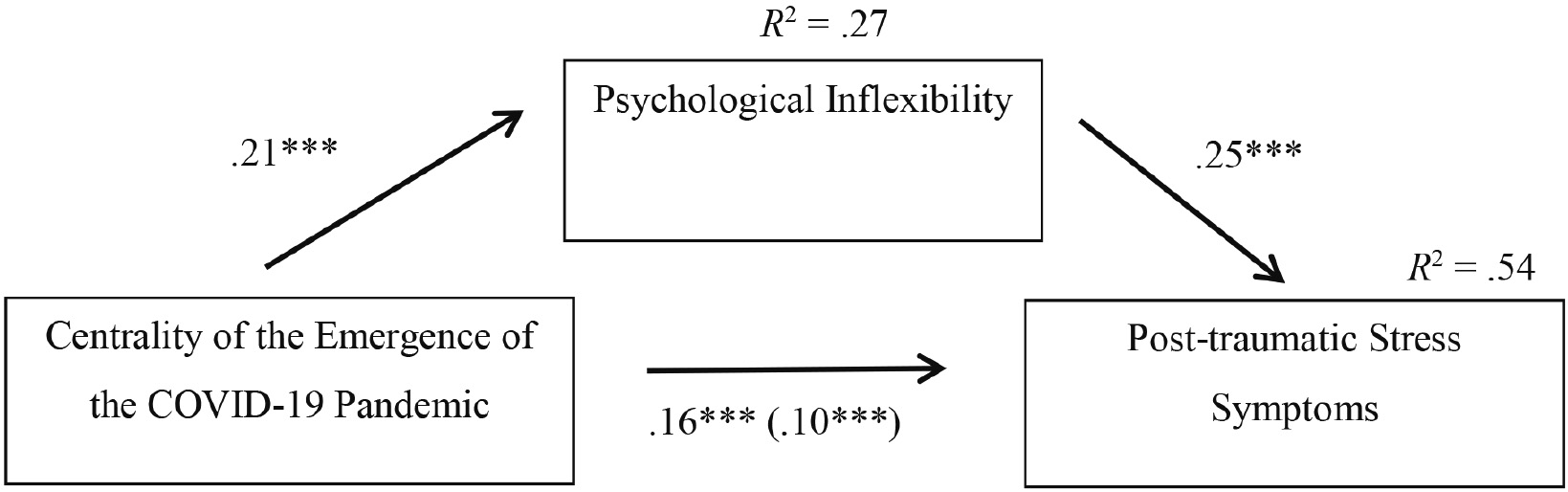
Note. The represented path values are unstandardized regression coefficients; ***p < .001
Figure 1 Path model of the centrality of the emergence of the COVID-19 pandemic as a predictor of post-traumatic stress symptoms in nurses, via psychological inflexibility
Table 3 Direct, indirect, and total effects

Note. PTSS = Post-traumatic stress symptoms; b = unstandardized regression coefficient; SE = standard error; t = t value; p = statistical significance; CI = confidence interval.
As depicted in Table 3, the centrality of the emergence of the COVID-19 pandemic was positively related to psychological inflexibility (b = .21, SE = .02, 95% CI [.17; .25]), and explained about 27% of the variance in the levels of psychological inflexibility (R 2 = .27). In its turn, psychological inflexibility was positively associated with PTSS (b = .25, SE = .02, 95% CI [.22; .28]). The direct effect of the centrality of the emergence of the COVID-19 pandemic on PTSS was significant (b = .10, SE = .01, 95% CI [.09; .12]). The indirect effect of the centrality of the emergence of the COVID-19 pandemic on PTSS was also significant (b = .05, [95% BCaCI = .04; .06]). This indicates that the relationship between the centrality of the emergence of the COVID-19 pandemic and PTSS in nurses was significantly mediated by psychological inflexibility.
The centrality of the emergence of the COVID-19 pandemic and psychological inflexibility, together, explained about 54% of the variance in PTSS (R 2 = .54). According to the values used to interpret these effect sizes in this study, these results indicate that the centrality of the emergence of the COVID-19 pandemic and psychological inflexibility have a large effect size on the development and maintenance of PTSS among nurses.
Discussion
To the best of our knowledge, the present study is the first to investigate the role of psychological inflexibility in the association between the centrality of the emergence of the COVID-19 pandemic and PTSS among nurses.
The main findings may be summarized as follows: firstly, centrality of the COVID-19 outbreak was moderately linked to psychological inflexibility and had a strong association with PTSS, and psychological inflexibility was also found to have a strong link with PTSS; secondly, psychological inflexibility was found to mediate the association between COVID-19 event centrality and PTSS.
In the present study, higher levels of COVID-19 event centrality were found to be linked to greater levels of psychological inflexibility, as well as to heightened PTSS. Additionally, greater levels of psychological inflexibility were also associated with graver PTSS. Taken altogether, our first hypothesis was confirmed.
The observed results also support the second hypothesis under examination in this study. A direct positive association was observed between COVID-19 event centrality and PTSS. Research has demonstrated that having a traumatic event as a reference point to one’s life is associated with an overall negative impact on mental health, including trauma symptoms (Berntsen & Rubin, 2006; Boykin et al., 2020; Yang et al., 2022). Consistent with the existing literature, this finding suggests that the more central the COVID-19 pandemic was to a nurse’s identity and personal narrative, the more likely they were to exhibit heightened signs of PTSS.
The COVID-19 pandemic event centrality was also indirectly associated with PTSS, via psychological inflexibility. Thus, psychological inflexibility was found to mediate the association between the COVID-19 pandemic event centrality and PTSS. The existing literature has established a connection between high event centrality of a traumatic event and rigid cognitive-behavioral patterns (Berntsen & Rubin, 2006), difficulties in adjustment, lower levels of psychological flexibility (Boykin et al, 2020) and with the development of trauma symptoms (Berntsen & Rubin, 2006; Boykin et al., 2020; Yang et al., 2022). Furthermore, some previous studies have also established an association between psychological inflexibility and worse psychological impairment (Arslan et al., 2020; Hayes et al., 2006; Levin et al., 2014), in which PTSS could be included.
These results suggest that not only do these variables seem to be associated, but the presence of psychological inflexibly may play a key mechanistic role in how event centrality and PTSS relate. Possible explanations for these associations could be related to the long-term effects of perceiving a traumatic event as central, a category under which the emergence of the COVID-19 pandemic could be classified. During the initial phase of the coronavirus pandemic outbreak, nurses faced multiple challenges. Isolation measures were enforced as an attempt to contain the virus’ spread; however, nurses were required to work longer shifts to ensure proper healthcare for the general population. As a result, isolation measures led nurses to take on the additional responsibility of facilitating communication between patients and their families, as well as providing end-of-life care more regularly (Kisely et al., 2020; Lai et al., 2020; Maben & Bridges, 2020). Additionally, given the novel nature of the virus at the emergence of the COVID-19 pandemic, information was initially unclear, and misinformation was spread. The exposure to media’s repetitive sensationalist information about the coronavirus pandemic, combined with the emerging fear, led to an overburdening of the already depleted healthcare facilities and medical resources, as well as to worse psychological outcomes (Garfin et al., 2020). Furthermore, as a highly transmissible and lethal virus, the COVID-19 pandemic also led to feelings of indecision and ethical dilemmas among nurses. Medical resources were finite, and criteria for patient prioritization had to be established. Nurses were also under the conflict between continuing to provide care or abandoning their workplace due to concerns about transmitting a potentially lethal virus to their significant others (Maben & Bridges, 2020). These healthcare professionals had to endure these conditions under the presence of frequent feelings of fear, for their lives and the lives of their significant others (Chen et al., 2021; Kisely et al., 2020; Lai et al., 2020; Maben & Bridges, 2020), and guilt due to the consequences of having to prioritize patients’ access to medical supplies (Maben & Bridges, 2020).
The high event centrality of such a traumatic event could lead to systematic negative interpretations and expectations of overall subsequent and non-related experiences, ruminations, and avoidance attempts (Berntsen & Rubin, 2006). Over time, the maintenance of this rigid maladaptive pattern could then evolve into or augment psychological inflexibility. Consequently, these low levels of psychological flexibility would limit one’s ability to adopt different perspectives, adapt to new situations, and overcome difficulties. In time, these limitations could potentially lead to the maintenance of psychological suffering, thereby culminating in deleterious mental health outcomes (Arslan et al., 2020; Hayes et al., 2006; Levin et al., 2014), such as PTSS.
Within this context, the present study has important implications for clinical practice. Nurses’ psychological health and wellbeing are crucial to ensure proper healthcare to the general population; however, this population has suffered deleterious mental health outcomes as a consequence of the COVID-19 pandemic outbreak.
First, given the high frequency of nurses who reported clinical scores for trauma symptoms, a stronger emphasis should be placed on screening traumatic symptomatology in this population to enable adequate intervention.
Second, younger nurses who identified as women presented heightened PTSS, consequently it is crucial to screen for these symptoms among the general nursing professional group, whilst directing special attention to more vulnerable subgroups in this population (e.g., women, nurses of younger age). Therefore, it is paramount to determine and implement adequate and tailored screening and treatment strategies for trauma-related symptoms among these healthcare professionals.
Third, more than half of these nurses highly centralized the emergence of the COVID-19 pandemic, and about a quarter of the sample exhibited psychological inflexibility levels above the cutoff score. These findings suggest that interventions should be aimed at assessing COVID-19 pandemic event centrality levels and enhancing psychological flexibility. This flexibility could be promoted by Acceptance and Commitment Therapy (ACT). This approach seeks to diminish the use of avoidance strategies in coping with unwanted internal experiences and, instead, increases the willingness to experience these private events while engaging in value-driven actions (Hayes et al., 2006). These processes seem to counteract the effects typically associated with high event centrality of a traumatic event, such as rumination, overidentification with the traumatic event, and avoidance attempts (Berntsen & Rubin, 2006). Therefore, fostering psychological flexibility among nurses could attenuate the deleterious effects of the centrality of the COVID-19 outbreak on trauma-related mental health outcomes.
Despite these contributions, the present study has some limitations that should be addressed when interpreting the results. First, the cross-sectional design of this study hinders the establishment of cause-effect relationships between variables, as correlation does not imply causation. Second, the use of a questionnaire protocol exclusively delivered in online-format may have excluded individuals with limited digital literacy or those who do not engage with social media. Third, the sample for our study was drawn from a Western European cultural context, which may limit the external validity and generalizability of these findings. The exclusive reliance on self-report measures poses another limitation, as these could be negatively impacted due to lack of self-awareness and social desirability bias. Additionally, the retrospective assessment of the experience could have been influenced by recall bias. The widespread impact of the coronavirus’ outbreak could have influenced individuals’ perceptions of the event due to factors like social interactions, media exposure, and infection, potentially compromising the accuracy of the reported data. Finally, despite the fact that the AAQ-II stands a reliable instrument to measure psychological inflexibility (Bond et al., 2011), some studies have questioned the discriminant validity of the AAQ-II and suggested that this measure may be more suitable to assess psychological distress (Tyndall et al., 2019), which, if that was the case, could contribute to inflated correlations between variables.
Future research should examine the proposed mediational model in a longitudinal study design to further ascertain these cross-sectional findings, and to seek to establish cause-effects relationships between the variables under study. This design would also be pertinent to assess the effectiveness and efficacy of the implementation of tailored ACT interventions in attenuating the impact of the COVID-19 outbreak centrality, or other potential future calamity outbreaks, and in decreasing trauma symptoms among nurses. Additionally, future studies could further explore the link between COVID-19 event centrality and PTSS, by analyzing other potential mediators, such as psychological resilience, coping strategies, and social support. Moderated mediation models could also examine the potential role of moderators in this association, such as gender, years of experience and psychological inflexibility. The effects of these mediators and moderators could be analyzed within both the nursing professional group and the general population. This comparison could provide further insights into which aspects are specific to the nursing professional group, and which are common across different populations.

