











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Cognitive functions are essential for maintaining autonomy, quality of life, and overall health across the lifespan. They encompass processes such as memory, attention, executive functions, and processing speed (Oschwald et al., 2020; Salthouse, 2019). Although there is robust evidence that some of these functions decline with age (e.g., working memory and processing speed) while others remain relatively preserved (e.g., language and verbal knowledge; Baghel et al., 2019; Ghisletta et al., 2019; Salthouse, 2019), the present study seeks to examine how depressive and anxious symptoms, even at subclinical levels, may influence cognitive functioning throughout aging.
Symptoms of depression and anxiety are among the most prevalent mental health problems worldwide and are leading contributors to disability and loss of quality of life (Chisholm et al., 2016). Although emotional manifestations are often emphasized, cognitive difficulties are also common and clinically significant among individuals with anxious and depressive symptoms (Lindert et al., 2021; McAllister-Williams et al., 2017).
According to the DSM-5 (American Psychiatric Association [APA], 2013), Major Depressive Disorder is diagnosed when at least five symptoms are present for a minimum of two weeks, and one of the symptoms must be depressed mood or loss of interest/pleasure. Other symptoms may include changes in appetite or weight, sleep disturbances, fatigue, feelings of worthlessness or guilt, difficulties with concentration, and recurrent thoughts of death. It is, however, essential to distinguish between a clinical diagnosis and subclinical depressive symptoms. Even below diagnostic thresholds, such symptoms are prevalent and have been associated with meaningful cognitive deficits, particularly in memory, attention, and executive functions (Lindert et al., 2021; McAllister-Williams et al., 2017).
Depression is a heterogeneous condition encompassing mood swings, anhedonia, psychomotor slowing, and reduced initiative, as well as a negative information processing bias, increased reactivity to negative information, and distorted perceptions of reality (Mulinari, 2012; Tartt et al., 2022). From a neurobiological perspective, depression has traditionally been explained by hypotheses of monoamine deficiency (e.g., serotonin and norepinephrine) in the synaptic cleft (Mulinari, 2012), but contemporary models highlight neuroplasticity deficits and structural alterations, particularly in the hippocampus and prefrontal regions (Sun et al., 2025). These alterations are associated with impaired episodic memory, reduced neurogenesis, and decreased cognitive flexibility (Berger et al., 2020). Neuroimaging studies also reveal dysfunctions in frontostriatal and corticolimbic circuits, associating depressive symptoms with executive deficits (e.g., working memory and inhibition) and attention difficulties (Dillon & Pizzagalli, 2018; Mulinari, 2012; Tartt et al., 2022; Zacková et al., 2021).
Its presentation varies across the lifespan: young adults tend to exhibit more affective-emotional symptoms, whereas midlife adults show greater functional impairment and higher rates of recurrence, medical comorbidity, and mortality (Diniz et al., 2013; Fiske et al., 2009; Perin et al., 2022). In older adults, somatic complaints such as sleep disturbance and fatigue are frequent (Fiske et al., 2009). Additionally, although late-life depression is associated with an increased risk of dementia (Diniz et al., 2013), longitudinal studies suggest that depressive symptoms in later life may reflect a prodrome of dementia rather than an independent risk factor (Singh-Manoux et al., 2017). This heterogeneity may differentially affect cognitive domains.
Anxiety, in turn, is characterized by excessive and difficult-to-control worry regarding a wide range of stimuli and activities, accompanied by cognitive and somatic symptoms such as restlessness, fatigue, difficulties in concentration, muscle tension, and sleep disturbances (APA, 2013; Del Giudice, 2018). As with depression, it is important to distinguish between subclinical anxious symptoms and clinically diagnosed anxiety disorders. Even below diagnostic thresholds, these symptoms may compromise essential cognitive functions, particularly attention, working memory, and executive functions (Eysenck et al., 2007; Shi et al., 2019).
According to Attentional Control Theory, anxiety disrupts the balance between goal-directed and stimulus-driven attentional systems, impairing inhibition, shifting, and updating, which are core components of executive functioning. As a result, anxious individuals tend to allocate disproportionate attentional resources to threat-related stimuli, which compromises performance in tasks requiring concentration, working memory, and cognitive flexibility in problem solving (Eysenck et al., 2007; Shi et al., 2019).
The cognitive effects of anxiety may vary across the lifespan. In young adults, significantly increased neuronal activity in the amygdala and insula has been associated with performance deficits in tasks requiring inhibitory control and cognitive flexibility, thereby heightening the tendency to worry and interfering with problem solving and decision-making (Etkin & Wager, 2007; Eysenck et al., 2007; Tempesta et al., 2013). In middle-aged adults, the presence of anxiety symptoms has been linked to a twofold risk of developing cognitive impairment over the following decade, ranging from mild to severe (Becker et al., 2018; Gimson et al., 2018). In older adults, however, anxiety is frequently underdiagnosed in comparison to depression, despite being one of the most common mental health problems in this age group and being associated with significant impairment in well-being and daily functioning (Bryant et al., 2008; Wolitzky-Taylor et al., 2010). In this population, anxiety symptoms predict episodic memory decline and are associated with poorer performance on verbal and executive tasks (Bunce et al., 2012; Fung et al., 2018).
From a biological perspective, elevated cortisol levels associated with prolonged anxiety symptoms contribute to poorer cognitive performance, particularly in memory tasks. However, the relationship between anxiety symptoms and cognitive decline depends on their severity and, unlike depression, the cognitive effects of anxiety appear to be more transient, tending to disappear after remission (Santabárbara et al., 2019). This pattern contrasts with depression, whose cognitive impact is frequently linked to more enduring neurobiological alterations, suggesting that anxiety may affect cognition through mechanisms that are potentially reversible yet clinically relevant (Chau et al., 2025; Lei et al., 2025).
Despite the extensive literature on depression and anxiety, our understanding remains limited regarding how symptom severity, even below diagnostic thresholds, affects cognitive performance across different stages of adulthood. This gap is particularly relevant because such symptoms are highly prevalent in the general population and may constitute cognitive vulnerability factors, especially among cognitively healthy older adults. Furthermore, it remains unclear whether depression and anxiety exert similar or distinct effects on cognition: some studies indicate that depression is primarily associated with deficits in executive functions and memory, whereas anxiety seems to particularly affect attention and working memory (Dillon & Pizzagalli, 2018; Tartt et al., 2022).
Against this backdrop, the present study aims to investigate the relationship between anxiety and depressive symptoms and cognitive performance in young, middle-aged, and older adults. Accordingly, we hypothesize that higher levels of depressive and anxiety symptoms will be associated with lower cognitive performance. We further expect these associations to vary across age groups.
Methods
Participants and procedures
The sample of this study includes 183 individuals recruited from the local urban community through study dissemination on social media (Facebook) and a snowball sampling procedure. Participants were eligible if they were 18 years of age or older, had at least four years of formal education, and Portuguese nationality. Individuals reporting uncorrected visual or motor impairments, as well as those who did not complete all neuropsychological tests, were excluded. Thus, 29 participants were excluded, resulting in a final sample of 154 individuals, divided into three groups according to age: 45 young adults (20-40 years; 23 men and 20 women), 61 middle-aged adults (40-60 years; 19 men and 44 women), and 48 older adults (60-80 years; 19 men and 29 women). Overall, the final sample comprised 61 men and 93 women. All participants were native European Portuguese speakers and confirmed full understanding of the procedures, informed consent, and task instructions.
This research was approved by the Ethics Committee of the Faculty of Psychology and Education Sciences of the University of Porto. Participants were individually assessed in a single experimental session of approximately 60 minutes, conducted by a trained neuropsychologist. The session aimed to confirm inclusion/exclusion criteria and collect sociodemographic and neuropsychological data.
All participants provided written informed consent and sociodemographic data through a semi-structured interview. The Montreal Cognitive Assessment (MoCA; Nasreddine et al., 2005; Portuguese version by Freitas et al., 2014) was administered first as a screening tool to characterize participants’ cognitive profiles. The remaining tests were then administered in random order, namely: Hospital Anxiety and Depression Scale (HADS; Snaith and Zigmond, 1994; Portuguese version by Pais-Ribeiro et al., 2007), Trail Making Test (TMT; Armitage, 1946; Portuguese version by Cavaco et al., 2013a), INECO Frontal Screening (IFS; Torralva et al., 2009; Portuguese version by Moreira et al., 2014), Corsi Block-Tapping Task (CBTT; Wechsler, 2008), Semantic (animals) and Phonemic (P, R, M) Fluency tests (Strauss et al., 2006; Portuguese version by Cavaco et al., 2013b), and the Brief Symptom Inventory (BSI; Derogatis, 1993; Portuguese version by Canavarro, 1999). Participants across the three age groups were equally distributed in the assessment schedule. Self-report measures (HADS, BSI) were completed directly by the participants.
Instruments
A semi-structured interview was developed that included questions about age, sex, marital status, native language, professional situation, years of education, bilingualism, proficiency in another language, hearing deficits, visual deficits, motor deficits, laterality, and a history of medical, psychiatric, and neurological illnesses.
Hospital Anxiety and Depression Scale. HADS is a 14-item scale divided into two self-report subscales that assess symptoms of anxiety (HADS-A) and depression (HADS-D) over the past two weeks. Each subscale comprises 7 items rated on a 4-point Likert scale (0 to 3). Scores range from 0 to 21 for each subscale, with higher scores reflecting greater symptom severity. In the present study, the validated Portuguese version was used, which maintains the original structure and scoring criteria. The Portuguese version has shown adequate internal consistency, with Cronbach’s alpha coefficients of .76 for the anxiety subscale and .81 for the depression subscale (Snaith and Zigmond, 1994; Portuguese version by Pais-Ribeiro et al., 2007).
Montreal Cognitive Assessment. MoCA is a brief cognitive screening tool designed to differentiate between normal cognitive aging and cognitive impairment, and is also useful for detecting mild cognitive impairment. It evaluates six domains: memory, visuospatial ability, executive function, language, orientation, attention, and working memory. Total scores range from 0 to 30, with higher scores indicating better performance. In this research, the Portuguese validated version was used, which has demonstrated high sensitivity and good internal consistency across cognitive domains, with a Cronbach’s alpha of .75 (Nasreddine et al., 2005; Portuguese version by Freitas et al., 2014).
Trail Making Test. TMT assesses attention, processing speed, and cognitive flexibility. It consists of two parts (A and B), in which participants connect sequences of stimuli as quickly as possible. Scoring is based on the completion time in seconds, with higher scores reflecting poorer performance. In addition to raw scores for Part A and Part B, a difference score (TMT-B minus TMT-A) can be calculated to evaluate divided attention without the influence of visuomotor speed. In the present study, the Portuguese version was used, which showed a Cronbach’s alpha of .89, indicating good internal consistency (Armitage, 1946; Portuguese version by Cavaco et al., 2013a). Furthermore, we used the difference score (TMT B-A) as the dependent variable, which provides a measure of divided attention and cognitive flexibility, minimizing the influence of visuomotor speed.
INECO Frontal Screening. IFS is a brief instrument for assessing executive dysfunction. It comprises eight subtests covering different executive domains, including motor programming, interference sensitivity, inhibitory control, verbal and spatial working memory, abstraction, and verbal inhibitory control. The total score ranges from 0 to 30, with higher scores indicating better performance. In this research, the validated Portuguese version was used, which reported a Cronbach’s alpha of .76, suggesting good internal consistency (Torralva et al., 2009; Portuguese version by Moreira et al., 2014).
Corsi Block-Tapping Task. CBTT is commonly used to assess visuospatial short-term and working memory, in both forward and backward versions. Maximum scores are 16 points for the forward version and 14 points for the backward version. Higher scores indicate better visuospatial memory performance (Wechsler, 2008).
Semantic and Phonemic Fluency Tests. Semantic and phonemic fluency tests are brief instruments that assess non-motor processing speed, verbal production, and executive functions. The total test score corresponds to the number of correctly produced words within the time established by the semantic category (animals) or initial phonemic (P, R, M) category, with higher scores corresponding to better performance. The Portuguese version used in this study demonstrated good internal consistency, with Cronbach’s alpha of .85 for semantic fluency and above .79 for phonemic fluency (Strauss et al., 2006; Portuguese version by Cavaco et al., 2013b). In this study, the measure of phonemic fluency used corresponded to the total number of words generated in the three letters (P + R + M), with higher scores indicating better performance.
Brief Symptom Inventory. BSI is a self-report instrument for screening psychological distress. It consists of 53 items distributed across nine symptom dimensions (somatization, obsessive-compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism) and three global indices (Global Severity Index, Positive Symptom Distress Index, and Positive Symptom Total). Items are rated on a scale from 0 (“never”) to 4 (“very often”), with higher scores reflecting greater symptom severity. In this study, the Portuguese version was used, which demonstrated Cronbach’s alpha coefficients ranging from .79 to .88 across the dimensions and indices, indicating good internal consistency (Derogatis, 1993; Portuguese version by Canavarro, 1999).
Statistical analysis
For statistical analyses, IBM SPSS Statistics, version 29.0 (IBM Corp, 2022), was used. Descriptive statistics were first conducted to characterize the groups in terms of sociodemographic and neuropsychological variables.
To compare groups with respect to educational level and neuropsychological test results, multivariate analysis of variance (MANOVA) was performed, with age group (young, middle-aged, older adults) as the between-subjects factor, and sex and years of education as covariates. Bonferroni post hoc tests were applied to explore group differences, and effect sizes (Cohen’s d) were calculated for each pairwise comparison, using the mean difference between groups divided by the pooled standard deviation.
To examine the relationship between emotional symptoms (depression and anxiety, assessed with the HADS) and cognitive performance, partial correlations were calculated, controlling for sex and years of education. Analyses were performed both for the complete sample and separately by age group. Considering that they already included the main covariates, in these analyses, unadjusted p-values were reported, without applying Bonferroni corrections.
The results were interpreted according to Cohen’s (1992) criteria: r between .10 and .29 was considered a weak association, r between .30 and .49 a moderate association, and r ≥ .50 a strong association. All analyses used a statistical significance threshold of α = .05 and were conducted using the raw scores of the instruments.
In addition, we report the number of participants who presented abnormal scores on the HADS: 21.4% of participants showed mild anxiety symptoms, 14.3% moderate, and 1.9% severe; in the depression subscale, 10.4% showed mild symptoms, 3.9% moderate, and 1.3% severe. Classification followed the standard HADS cut-off values (0-7 = normal, 8-10 = mild, 11-14 = moderate, 15-21 = severe; Pais-Ribeiro et al., 2007).
Results
Table 1 shows the descriptive results of each group regarding formal education, scores obtained in each test, and the self-report scale. A one-way ANOVA revealed a significant effect of age group on years of education, F(2,151) = 8.66, p < .001, ηp² = .103. Bonferroni post hoc comparisons showed that older adults had significantly fewer years of formal education than both younger (mean difference = -3.27, p = .001) and middle-aged adults (mean difference = -2.98, p = .001), whereas younger and middle-aged adults did not differ significantly (mean difference = .293, p = .937).
Table 1 Descriptive statistics of neuropsychological results
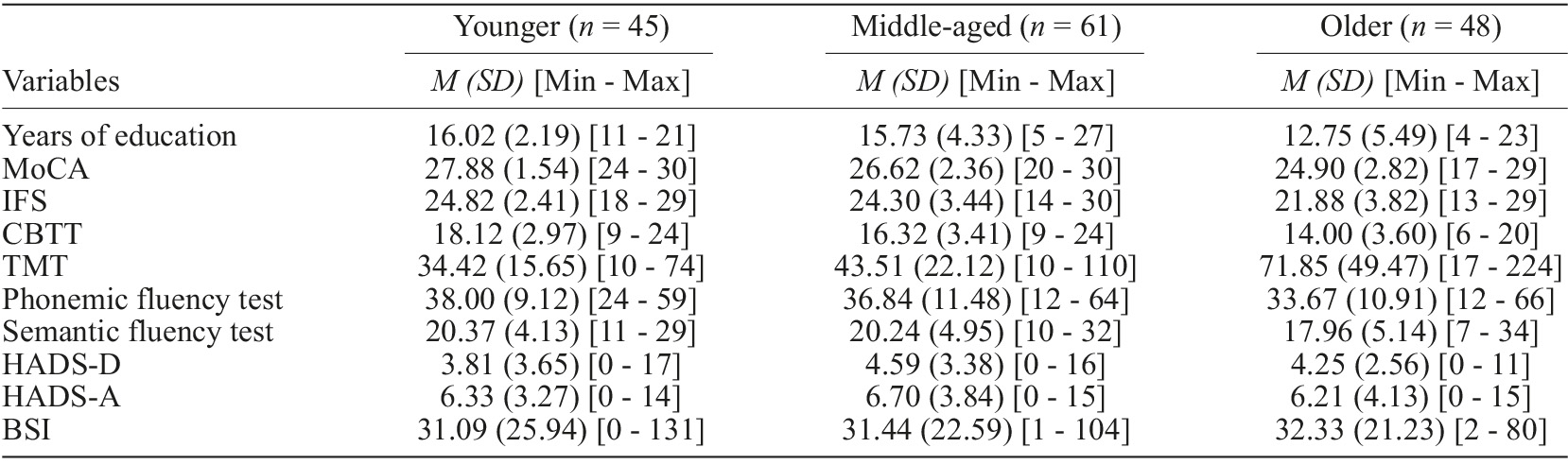
Note. M: mean, SD: standard deviation; Min: minimum; Max: maximum; MoCA: Montreal Cognitive Assessment; IFS: INECO Frontal Screening; CBTT: Corsi Block-Tapping Test; TMT: Trail Making Test; HADS: The Hospital Anxiety and Depression Scale; BSI: Brief Symptom Inventory.
To characterize the sample in all age groups, multivariate analyses (MANOVA) were performed, controlling for education and sex as covariates. Univariate analyses revealed differences between groups in MoCA with F (2,149) = 11.25, p < .001, η²p = .131; in IFS with F (2,149) = 4.18, p = .017, η²p = .053; in Corsi with F (2,149) = 11.15, p < .001, η²p = .130; and in the TMT with F (2,149) = 9.93, p < .001, η²p = .119. Bonferroni post hoc tests, including effect sizes (Cohen’s d), demonstrated that young and middle-aged adults performed better than older adults on all these measures. Detailed results of the pairwise comparisons are presented in Table 2. No significant differences were observed between groups in phonemic fluency, semantic fluency, HADS-D, HADS-A, or BSI (p > .05).
Table 2 Univariate analyses and bonferroni-corrected pairwise comparisons of cognitive measures across age groups (n = 154)
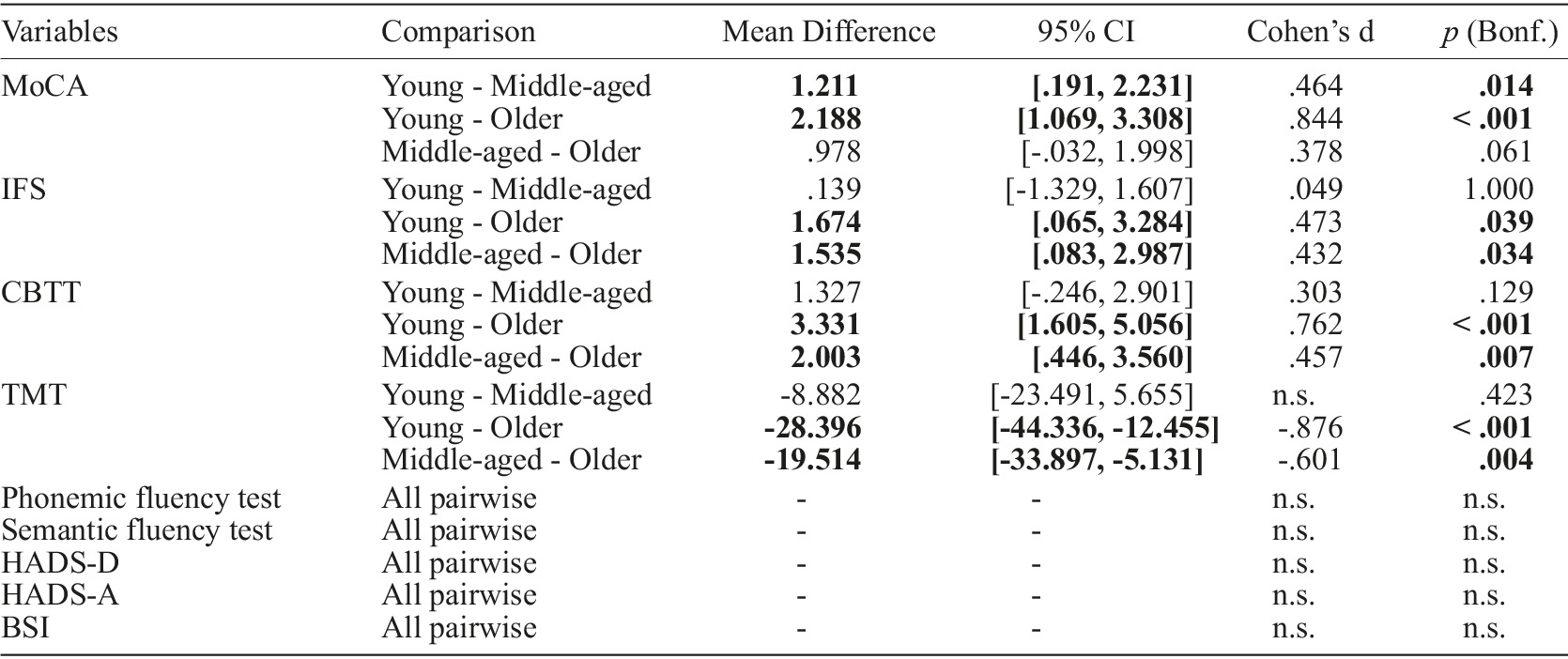
Note. Bold values represent significant correlations, 95% CI: 95% confidence intervals, p: significance Bonferroni-adjusted, n.s.: non-significant results; MoCA: Montreal Cognitive Assessment; IFS: INECO Frontal Screening; CBTT: Corsi Block-Tapping Test; TMT: Trail Making Test; HADS: The Hospital Anxiety and Depression Scale; BSI: Brief Symptom Inventory.
Correlation between psychological symptoms and cognitive functions
Table 3 presents the results of the correlation between mood symptoms and cognitive functions, controlling for sex and years of education. The results showed a significant, strong, and positive correlation between the HADS-D and HADS-A (r = .547, p < .001), as well as between both HADS subscales and the broader psychopathological symptoms assessed by the BSI (HADS-D: r = .619, p < .001; HADS-A: r = .675, p < .001). No significant associations were found between the HADS-D and the cognitive measures. However, anxiety symptoms (HADS-A) showed a significant negative correlation with IFS (r = -.160, p = .049), suggesting a potential trend toward poorer executive functioning with higher levels of anxiety. Additionally, a marginal negative correlation was observed between HADS-A and MoCA (r = -.140, p = .086).
Table 3 Partial correlations between HADS and cognitive performance, controlling for sex and education (n = 154)
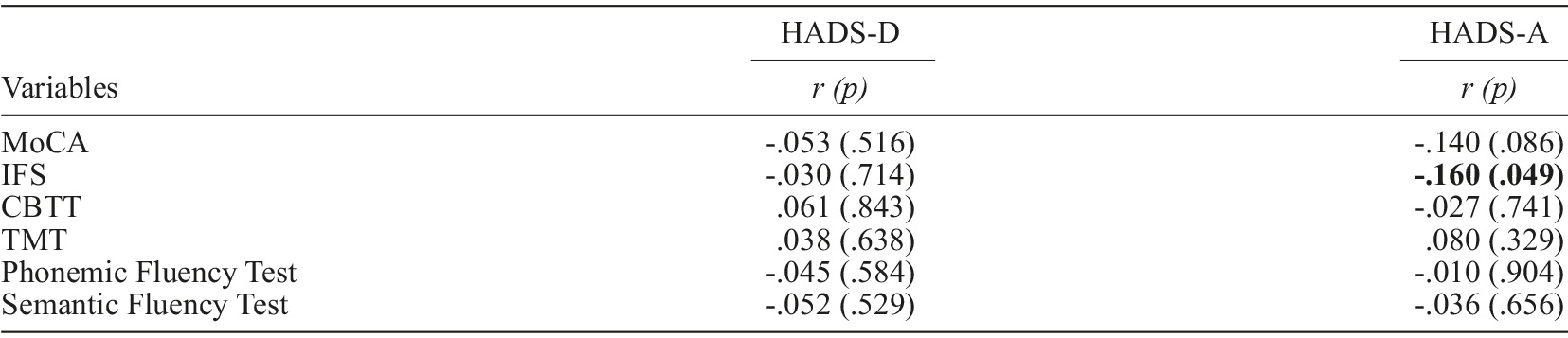
Note. Bold values represent significant correlations, r: Pearson correlation, p: significance. MoCA: Montreal Cognitive Assessment; IFS: INECO Frontal Screening; CBTT: Corsi Block-Tapping Test; TMT: Trail Making Test; HADS: The Hospital Anxiety and Depression Scale.
Correlation between psychological symptoms and cognitive functions by group
Controlling for sex and years of education, no significant partial correlations were observed between anxiety/depression symptoms and cognitive performance in young or middle-aged adults (all p ≥ .101).
In contrast, among older adults, anxiety symptoms (HADS-A) were associated with poorer performance on the MoCA (r = -.411, p = .005) and the IFS (r = -.483, p < .001). Marginal trends (.050 ≤ p < .100) were observed in older adults on the CBTT (r = -.271, p = .068) and TMT (r = .275, p = .064), both suggesting worse performance with higher levels of anxiety. No associations were found between HADS-A and semantic and phonemic fluency tests (both p > .600). Furthermore, depressive symptoms (HADS-D) did not correlate significantly with cognitive measures in any age groups (all p ≥ .270). Importantly, strong and positive correlations were consistently observed between both HADS subscales and the BSI across all age groups (r ≥ .365, all p ≤ .013), supporting the convergent validity of these measures (Table 4).
Table 4 Partial correlations between HADS and cognitive performance by age group, controlling for sex and education
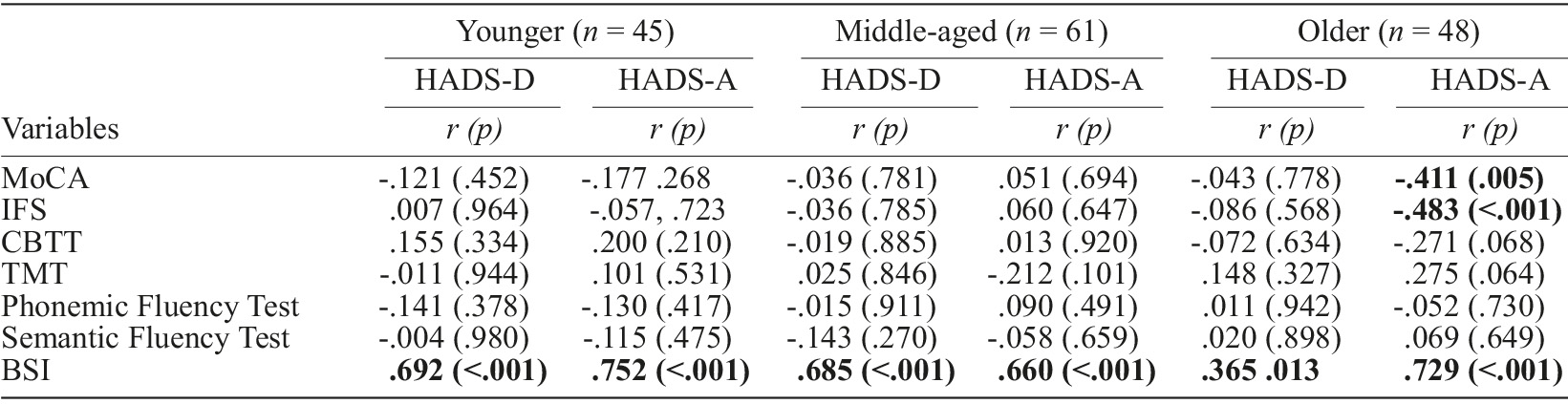
Note. Bold values represent significant correlations, r: Pearson correlation, p: significance; MoCA: Montreal Cognitive Assessment; IFS: INECO Frontal Screening; CBTT: Corsi Block-Tapping Test; TMT: Trail Making Test; BSI: Brief Symptom Inventory.
Discussion
The present study investigated the relationship between anxiety and depressive symptoms, even at subclinical levels, and cognitive performance across different stages of adulthood. In addition to examining the association between emotional symptomatology and cognitive functioning, the study also compared performance across distinct neuropsychological domains among young, middle-aged, and older adults, providing an essential context for interpreting the associations with anxiety and depressive symptoms.
According to the results, a significant difference was observed between young and middle-aged adults in global cognitive performance, as measured by the MoCA, with the younger group performing better. In addition, a marginal trend was observed in the CBTT, indicating slightly better visuospatial working memory performance among young adults, although this difference did not reach statistical significance. For the remaining tests (executive functions, processing speed, attention, cognitive flexibility, and verbal fluency), no significant differences were observed between the two groups.
When compared with older adults, young adults performed significantly better across multiple cognitive domains: global cognition (MoCA), executive functions (IFS), visuospatial working memory (CBTT), as well as attention, processing speed, and cognitive flexibility (TMT). These results confirm the pattern described in the literature, according to which aging is associated with marked declines in functions that rely on attentional and executive resources (Oschwald et al., 2020; Salthouse, 2019).
When comparing middle-aged and older adults, significantly higher performance was observed in middle-aged adults on tests assessing executive functions (IFS), visuospatial working memory (CBTT), and attention, processing speed, and cognitive flexibility (TMT). Furthermore, a marginal difference was observed in global cognition (MoCA), suggesting a trend toward higher performance in middle-aged adults compared to older adults. In contrast, across all age group comparisons, no significant differences were found in verbal fluency tests (semantic and phonemic), reinforcing the notion that these tasks, which rely on abilities associated with crystallized intelligence, remain relatively preserved throughout aging (Baghel et al., 2019; Ghisletta et al., 2019).
With regard to emotional symptomatology, self-report measures (HADS and BSI) did not reveal significant differences among the three age groups. This finding is consistent with studies suggesting that healthy aging may preserve affective regulation (Mather, 2016). However, when examining the descriptive data from the present sample, middle-aged adults presented slightly higher mean scores on both the HADS-D and HADS-A compared with young adults and older adults, although without reaching statistical significance. This result is in line with research reporting a higher prevalence of depressive and anxious symptoms in middle-aged adults (Perin et al., 2022), although other studies have documented higher rates in older adults (Bryant et al., 2008; Fiske et al., 2009). Methodological differences, sample heterogeneity, contextual factors, biological changes associated with aging, and underreporting of symptoms due to stigma or cognitive biases may all contribute to these discrepancies, highlighting the need to further investigate the effect of age on the prevalence of depression and anxiety.
The correlational analysis yielded relevant findings. First, no significant associations were found between depressive symptoms, as assessed by the HADS-D, and cognitive performance on any of the neurocognitive tests used in the present study after controlling for sex and years of education. When analyzed by age groups, no significant associations were found in any group, suggesting that in this non-clinical sample, subclinical levels of depressive symptomatology may not have an evident impact on cognitive functioning. This result is consistent with the literature, indicating that the most consistent cognitive deficits in depression tend to emerge in clinical conditions, often associated with more enduring neurobiological alterations, and are therefore less likely to manifest robustly at subclinical levels (Dillon & Pizzagalli, 2018; Zacková et al., 2021).
In contrast, anxiety symptoms, as assessed by the HADS-A, were significantly associated with the IFS, suggesting poorer executive functioning as anxiety levels increased, and showed a marginal trend with the MoCA, indicating a potential impact on global cognition. These findings align directly with the Attentional Control Theory, which proposes that anxiety destabilizes the balance between goal-directed and stimulus-driven attentional systems, impairing core processes such as inhibition, shifting, and updating, components assessed by the IFS (Eysenck et al., 2007). When correlations were analyzed by age group, anxiety symptoms proved to be particularly relevant among older adults. In this group, higher levels of anxiety were associated with poorer performance in measures of global cognition (MoCA) and executive functions (IFS), as well as marginal trends in visuospatial working memory (CBTT) and cognitive flexibility (TMT). This pattern was not identified among young or middle-aged adults, suggesting that the impact of anxiety on cognitive performance may become more evident with advancing age. Moreover, younger individuals may benefit from greater compensatory resources, whether through cognitive reserve or greater brain plasticity, which allow them to minimize or mask cognitive difficulties related to anxiety while maintaining normative performance. With increasing age, however, the decline in cognitive reserve and the greater fragility of neurobiological systems render the effects of anxiety on cognitive functioning more evident (Barulli & Stern, 2013; Reuter-Lorenz & Park, 2014).
With regard to the proposed hypothesis, no significant associations were found between depressive symptoms and cognitive performance in any of the age groups, which partially contradicted the initial expectation. By contrast, higher levels of anxiety were associated with poorer cognitive functioning among older adults, both in measures of global cognition and executive functions, as well as marginal trends in working memory and cognitive flexibility. This pattern suggests that while anxiety emerges as a cognitive vulnerability factor, its effects are more evident in later life. Thus, the hypothesis that associations between emotional symptoms and cognitive performance would vary across age groups was confirmed, albeit only in relation to anxiety. From a theoretical perspective, these findings reinforce the notion that anxiety, even at subclinical levels, may represent a modifiable risk factor for cognitive health in advanced age, whereas depression appears to require greater clinical severity to produce measurable impacts, often linked to more enduring neurobiological alterations.
Considering that the effects of anxiety symptomatology on cognition appear to be more transient and tend to disappear following symptom remission (Santabárbara et al., 2019), it can be hypothesized that reducing anxiety levels in older adults might attenuate or even minimize the cognitive performance differences observed between this group and younger adults. In this sense, the effective treatment of anxiety in older adults may not only promote emotional well-being but also represent a potential strategy for preserving cognitive health and functional autonomy in this population. However, this interpretation requires confirmation in future investigations.
This study presents some limitations that should be considered. The relatively small sample size, particularly after dividing participants into age groups, limits both the statistical power and the generalizability of the findings. In addition, the cross-sectional design does not allow for causal inferences between emotional symptoms and cognitive performance. Future longitudinal investigations with larger and more representative samples are needed to confirm and extend these findings.
In addition to the limitations already mentioned, it is important to highlight the difference in educational level across age groups. Education is a major factor influencing cognitive performance and is widely recognized as a central component of cognitive reserve (Stern et al., 2020). Indeed, in the present sample, older adults had, on average, fewer years of formal education compared with the younger groups, which could have influenced the results. To mitigate this effect, years of education were included as a covariate in the multivariate analyses, together with sex, in order to strengthen the robustness of group comparisons. Nevertheless, the educational discrepancy remains a limitation, as it is not possible to eliminate its influence on cognitive performance. Future investigations should consider samples that are more homogeneous with respect to education. Another aspect to consider is that, although none of the participants presented a clinical diagnosis of dementia or other neurological disorder, the MoCA was used only as a screening measure and not as an exclusion criterion. Thus, future studies could adopt more restrictive exclusion criteria to ensure greater sample homogeneity.
Despite these limitations, the findings highlight the relevance of examining anxiety and depressive symptoms as continuous variables, even below diagnostic thresholds, and of exploring their effects across different stages of adulthood. Specifically, the association between anxiety and cognitive performance in older adults suggests important practical implications for both psychological assessment and clinical intervention.

