










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkArquivos de Medicina
versão On-line ISSN 2183-2447
Arq Med vol.29 no.5 Porto out. 2015
PUBLICAÇÃO BREVE
Association between parity and breast cancer among women in north-central Nigeria: an exploratory case-control analysis
Musa Abubakar Kana1,2, Maikano Ari3, Poki Solomon4, Nuno Lunet2,5
1Department of Community Medicine, Faculty of Medicine, Kaduna State University, Kaduna, Nigeria
2 EPIUnit – Institute Of Public Health, University of Porto (ISPUP), Porto, Portugal
3Nasarawa State University, Keffi, Nigeria
4Taimako Cancer Screening Centre, Doma, Nigeria
5Department of Clinical Epidemiology, Predictive Medicine and Public Health, University Of Porto Medical School, Porto, Portugal
ABSTRACT
Background: Many studies conducted over the years have recognized the substantial epidemiologic evidence on the contribution of reproductive factors for the occurrence of breast carcinoma, including parity. However, most studies evaluated relatively homogeneous populations, with a small number of women with high fertility, and the association of very high parity with breast cancer remains poorly understood. Therefore, we addressed this topic in an African population characterized by high fertility rates.
Methods: We conducted a case-control analysis among women that were attending the Taimako breast and cervical cancer-screening centre, which is located in Nasarawa state of North-Central Nigeria.
Results: Among cases, 34.5% of the women were 39 years or less. About a quarter had ever used oral contraceptives, nearly half had attained menopause, and nearly two thirds had parity higher than 4 (parity 5-6, 32.1%; parity 7-8, 25.0%, parity =9, 7.1%). Compared to women with parity 1-4 the risk of breast cancer tended to be higher among nulliparous women (OR=3.44, 95%CI: 0.68-17.54), though it was lower among those aged =45 years (OR=1.43, 95%CI: 0.11-18.22) and higher in participants aged >45 years (OR=12.07, 95%CI: 0.62-233.00). For women with higher parity, the OR estimates were similar for those with parity 5-6 (OR=2.54, 95%CI: 0.80-8.01) and 7-8 (OR=2.65, 95%CI: 0.74-9.48).
Conclusion: Our results suggest that future increase in incident breast cancer cases in this setting may result from an improvement of screening and diagnostic services, rather than from a dramatic but unlikely reduction in parity.
Key-words: breast neoplasms, risk factors, parity, Nigeria
Background
Breast cancer is the most common cause of cancer death among women and the most frequently diagnosed cancer among women in 140 of 184 countries worldwide.1,2 In the past, African women comparatively had lower incidence of this cancer but, proportionately, a higher mortality rate.1 However, in general, the incidence of breast cancer is increasing globally, more rapidly in societies that hitherto enjoyed a low incidence of the disease, such as African countries.1-3
Many studies conducted over the years have recognized the substantial epidemiologic evidence on the contribution of reproductive factors for the occurrence of breast carcinoma, including parity.4-6 Nulliparous women were shown to be at a higher risk than parous women, especially above the age of 45.7 However, most studies evaluated relatively homogeneous populations, with a small number of women with high fertility, and the association of very high parity with breast cancer remains poorly understood. Therefore, we addressed this topic in an African population characterized by high fertility rates.
Methods
We conducted a case-control analysis among women that were attending the Taimako breast and cervical cancer-screening centre, which is located in Nasarawa state of North-Central Nigeria.8 The context and methodology of this centre has been described elsewhere.8 Briefly,it started operations in 2008, by providing free breast and cervical cancer screening and diagnostic services, and initiating sustained health education (community based and other media forms) activities to increase awareness of female cancers, to a catchment population in the state of about 1.8 million people.8,9 Between May 2009 and April 2010 a total of 2,095 women presented for breast cancer screening or diagnosis. We selected those with confirmed histological diagnosis of breast carcinoma as cases (n=29). Although, women were attending a screening and diagnosis centre, nearly all cases were symptomatic. Therefore, age-and education-matched controls (n=143) were randomly selected among women with no breast pathology that presented to the centre due to pain/ discomfort or palpable lump. We selected up to six controls per case, although for some cases, especially the younger and more educated women, there were less than six controls available in the sample. The Health Research and ethics Committee of Jos University Teaching Hospital, plateau state, Nigeria approved the study protocol and informed consent was obtained from all women that participated.
To estimate the relation between parity and breast cancer we computed odds ratios (OR) and corresponding 95% confidence intervals (95%CI) using unconditional logistic regression. The potential confounders were selected a priori among those available in the dataset and were included as adjustment variables in all the models, in addition to age and education. All analyses were performed using STATA, Version 11.2 (stata Corporation, College station, Texas).
Results
Among cases, 34.5% of the women were 39 years or less, nearly two-thirds did not have formal education, the mean (standard deviation) age at menarche was 14.5 (1.6), about a quarter had ever used oral contraceptives, nearly half had attained menopause, and nearly two thirds had parity higher than 4 (parity 5-6, 32.1%; parity 7-8, 25.0%, parity =9, 7.1%).
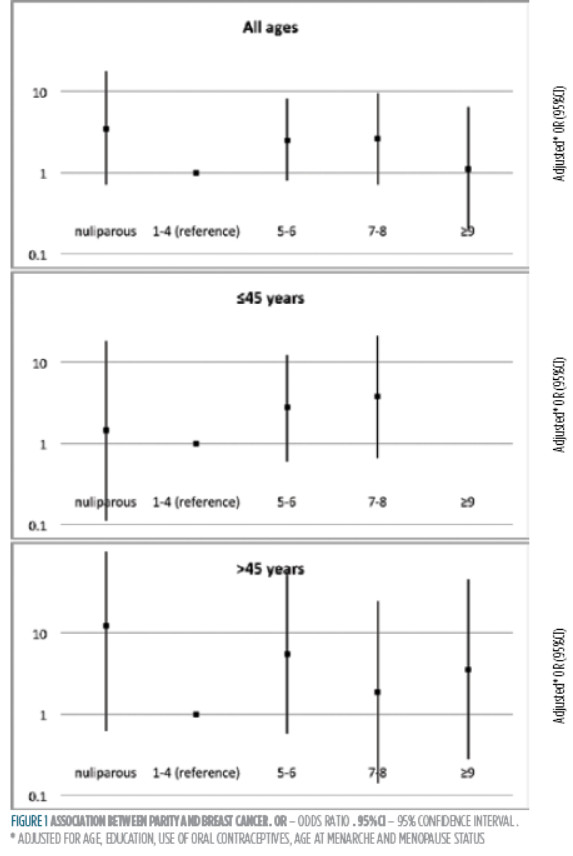
Figure 1 depicts the result of the adjusted regression models fitted to assess the role of parity in breast carcinogenesis. Compared to women with parity 1-4 the risk of breast cancer tended to be higher among nulliparous women (OR=3.44, 95%CI: 0.68-17.54), though it was lower among those aged =45 years (OR=1.43, 95%CI: 0.1118.22) and higher in participants aged >45 years (OR=12.07, 95%CI: 0.62-233.00). For women with higher parity, the OR estimates were similar for those with parity 5-6 (OR=2.54, 95%CI: 0.80-8.01) and 7-8 (OR=2.65, 95%CI: 0.74-9.48), and lower for those reported to have had 9 or more children (OR=1.09, 95%CI: 0.19-6.30). The association did not increase consistently with parity when the analysis was stratified by age.
Discussion
The analysis we conducted is constrained by a small number of cases, because of the low prevalence of breast cancer observed in this sample.8 However, our finding are consistent with those of studies that reported parity as compared to nulliparity being associated with lower breast cancer risk7,10, as well as a crossover in which no increased risk is observed among the younger nulliparous women, and higher risks among older nulliparous women.7 Our study adds to previous research on this topic evidence supporting that the risk of breast cancer does not vary consistently with increasing parity in a setting where fertility is very high (the total fertility rate in Nigeria is 5.5,11 though the paucity of cases precludes more robust conclusions.
The relation between parity and breast cancer can be confounded by other reproductive factors.4-6 Although information about some of these variables was unavailable in the dataset used for our analysis, we may expect a strong correlation between high parity and age at first birth, and recent demographic and health survey in Nigeria has shown that 95.5% of children less than 6 months were breast-fed,11 which minimizes the potential for uncontrolled confounding.
Projections have been made that if younger African-American women are now giving birth to fewer children than in the past, without a substantial increase in breast feeding, breast carcinoma rates may continue to increase at a more rapid rate in this population group than among white women.7 Our results suggest that such trends are less likely in our study setting; an increase in incident breast cancer cases recorded may result from an improvement of screening and diagnostic services, rather than from a dramatic but unlikely reduction in parity.
Finally, more studies with bigger sample sizes and conducted in similar settings are required. Future research on this subject should favour population-based data and analytical study designs that will spawn better evidence, in terms of generalization and ability to demonstrate causality.
References
1. Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F. GLOBOCAN 2012 v1.0, Cancer incidence and mortality worldwide: IARC Cancer Base No. 11. lyon, France: International Agency for Research on Cancer; 2013. Available from: http://globocan.iarc.fr , accessed on 30/10/2014 [ Links ]
2. Amaro J, Severo M, Vilela S, Fonseca S, Fontes F, Vecchia, Lunet N. Patterns of breast cancer mortality trends in europe. Breast. 2013 Jun; 22(3):244-53. doi: 10.1016/j.breast.2013.02.007. Epub 2013 Mar 9 [ Links ]
3. McCormack VA, Boffetta P. Todays lifestyles, tomorrows cancers: trends in lifestyle risk factors for cancer in low-and middle-income countries. Ann Oncol. 2011;22(11):2349-57. [ Links ]
4. Anderson KN, Schwab RB, Martinez Me. Reproductive risk factors and breast cancer subtypes: a review of the literature. Breast Cancer Res Treat. 2014;144(1):1-10. [ Links ]
5. Beral V, Bull D, Doll R, Peto R, Reeves G. Breast cancer and abortion: collaborative reanalysis of data from 53 epidemiological studies, including 83,000 women with breast cancer from 16 countries. Lancet. 2004;363(9414):1007-16. [ Links ]
6. Ma H, Bernstein L, Pike MC, Ursin G. Reproductive factors and breast cancer risk according to joint estrogen and progesterone receptor status: a meta-analysis of epidemiological studies. Breast Cancer Res. 2006;8:R43. [ Links ]
7. Palmer JR, Wise La, Horton NJ, Adams-Campbell Ll, Rosenberg L. Dual effect of parity on breast cancer risk in African-American women. J Natl Cancer Inst. 2003;95:478-83 [ Links ]
8. Ozoilo Kn, Chukwuogo O, Ozoilo JU, Ojo EO,Yakubu AA. Breast cancer screening in a resource poor setting: A preliminary report. J Med Trop. 2014;16(1):14-8. [ Links ]
9. National Population Commission [NPC]. Population and housing census of the Federal Republic of Nigeria 2006. Abuja, Nigeria: NPC; 2007 Available from: http://www.population.gov.ng , accessed 30/10/2014 [ Links ]
10. Huo D, Adebamowo CA, Ogundiran TO, et al. parity and breastfeeding are protective against breast cancer in Nigerian women. Br J Cancer. 2008;98(5):992-6. [ Links ]
11. National population Commission [NPC] [Nigeria] and ICF International. Nigeria Demographic and Health survey 2013. Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF International; 2014. Available from: http://dhsprogram.com/pubs, accessed 30/10/2014 [ Links ]
Musa Abubakar Kana
Instituto de Saúde Pública da Universidade do Porto (ISPUP), rua das taipas, 135 -4050-600 Porto, Portugal. E-mail: up201308483@med.up.pt
Data de recepção / reception date: 06/01/2015
Data de aprovação / approval date: 16/01/2015

