










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.26 no.1 Lisboa jan. 2012
Membranous nephropathy in three paediatric patients
Susana Nobre1, Raquel Santos1, Clara Gomes1, Fernanda X. Cunha2, António J. Correia1
1 Nephrology Unit, Hospital Pediátrico Carmona da Mota, Centro Hospitalar de Coimbra. Portugal.
2 Pathology Department, Hospitais da Universidade de Coimbra. Portugal.
ABSTRACT
Membranous nephropathy in childhood is usually secondary to an underlying cause. Idiopathic membranous nephropathy is a rare cause of paediatric asymptomatic proteinuria/nephrotic syndrome.
We reviewed the only three cases of membranous nephropathy followed in a paediatric hospital over the last ten years. All patients were female with mean age at diagnosis of 11.3 years (10-13 years). Patients 1 and 2 presented with steroid-resistant nephrotic syndrome. Patient 3 had a history of episodes of gross haematuria, and subnephrotic-range proteinuria refractory to enalapril and losartan. All patients had normal renal function. Patient 2 had hypertension and microscopic haematuria. Patients 1 and 2 underwent renal biopsy at an average of 51.5 days after initial symptoms; in patient 3, renal biopsy was performed seven years after initial presentation with episodes of gross haematuria, and five years after discovery of proteinuria. Histopathological features indicated membranous nephropathy; in patients 2 and 3, some findings suggested the coexistence of a systemic clinical condition.
Secondary causes were sought in all patients. Six months after diagnosis, patient 1 developed facial skin lesions suggestive of discoid lupus erythematosus and later had positive autoantibodies (ANA, ENA, anti-SSA).
Corticosteroids and angiotensin II receptor antagonists or angiotensin converting enzyme inhibitors were given to all patients. Those with nephritic syndrome required the addition of ciclosporin to achieve remission.
At the latest evaluation (mean follow-up 31.3 months), patients 1 and 3 were in remission, and patient 2 had sub-nephrotic range proteinuria as the result of poor adherence to medication. All had normal renal function and blood pressure. All were receiving treatment with prednisolone and enalapril, and patients 1 and 2 were also receiving ciclosporin.
Diagnosing idiopathic membranous nephropathy in children can be challenging. At least one of our patients had atypical features suggestive of an underlying cause so may have had secondary membranous nephropathy. Follow-up must continue, even after remission, with continued monitoring for underlying systemic disease. Treatment options are angiotensin converting enzyme inhibitors or angiotensin II receptor antagonists, corticosteroids and immunosuppressive drugs such as ciclosporin.
Key-Words: Ciclosporin; idiopathic membranous nephropathy; nephrotic syndrome; steroids.
INTRODUCTION
Membranous nephropathy (MN) is an immune complex mediated disease in which antibodies are believed to react in situ against endogenous antigens1. It has distinct pathologic features: normocellular glomerular wall thickening on light microscopy, subepithelial immune complex deposits that appear as granular deposits of immunoglobulin G on immunofluorescence, and subepithelial electron dense deposits on electron microscopy2,3.
Membranous nephropathy occurs in a primary or idiopathic form, or may be secondary to an underlying cause1. In a paediatric population, MN is usually associated with systemic lupus erythematosus (SLE), hepatitis B or C infection, sickle-cell disease, congenital syphilis, malaria, Epstein-Barr virus infection or administration of various medications (eg D-penicillamine and gold salts)2,4. Idiopathic MN is one of the most common causes of primary nephrotic syndrome (NS) in adults, but is rare in children2-4. In a paediatric population with glomerular disease (NS or asymptomatic proteinuria) selected for renal biopsy, the prevalence of MN is approximately 2%4 to 6.8%3. The International Study for Kidney Disease in Children demonstrated that the incidence of MN is less than 2% in children with NS biopsied at disease onset, and increases to 7.1% in those with steroid-resistant NS5. Owing to the relatively low incidence of MN in children, most data on its natural history and progression have been extrapolated from studies in adults. The clinical course is variable and spontaneous remissions and relapses may occur1,2.
Our unit deals with children up to the age of 14 years and we see an average of 1623 children per year (9% first consultations). Over the last 10 years, we have performed 21 renal biopsies for NS/nephroticrange proteinuria, and only the three children presented here (14%) had histopathological features of MN.
DEFINITIONS
Nephrotic-range proteinuria was defined as a 24-hour urinary protein >40 mg/m2/hour, or a random urine protein/creatinine ratio (Upr/Ucr)≥200 mg/mmol.
NS was defined as the association of nephrotic-range proteinuria, low serum albumin (<2.5 g/dL), oedema and hyperlipidaemia (total cholesterol >250 mg/dL).
Haematuriawas defined as more than five erythrocytes per high-power field on urinalysis.Hypertension was defined as systolic and/or diastolic blood pressure >95th percentile for age, gender and height.
Glomerular filtration rate (GFR) was estimated using the Schwartz formula.
Remission of proteinuria was defined as negative or trace urinary protein by dipstick test for three consecutive days, Upr/Ucr <20 mg/mmol or 24-hour urinary protein <4 mg/m2/hour.
CASE REPORTS
Patient 1(P1)
An eleven-year-old girl was found to have NS in February 2006 after presenting with bilateral eyelid oedema, weight gain (12 Kg in two months), normal blood pressure, nephrotic-range proteinuria without haematuria, low serum albumin and hypercholesterolaemia (Table I). Renal function and complement (C3, C4) were normal and Anti-DNA and ANA were negative. Renal ultrasound was normal. Secondary causes of NS were excluded.
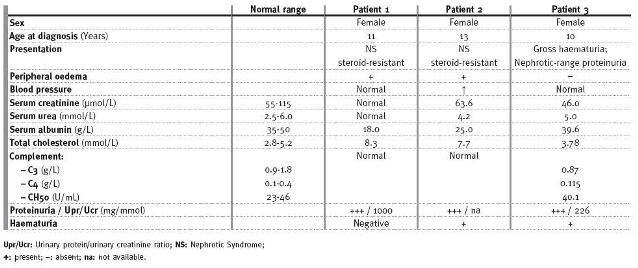
Table I
Membranous nephropathy in paediatric patients: clinical and laboratory data at the onset of the disease.
She was treated with oral prednisolone (60 mg/m2/day) for five weeks but nephrotic-range proteinuria (236 mg/m2/hour) persisted. She was then given six methylprednisolone pulses (750 mg every 48 hours) without a significant effect on proteinuria. Two months after diagnosis, a renal biopsy was performed which revealed MN with some findings suggestive of the presence of a systemic clinical entity (Table II). Dipyridamole (75 mg twice a day), enalapril (5 mg/day) and ciclosporin (200 mg/day) were added to the previous treatment with prednisolone (40 mg/48 hours). Two months later she was in remission. After a further four months, she developed facial skin lesions suggestive of discoid lupus erythematosus (DLE) and was treated with hydroxy chloroquine for three weeks. Thereafter, ANA, ENA and anti-SSA became positive but complement levels remained normal. She had no other manifestations of lupus erythematosus. One year after diagnosis (May 2007), she relapsed with proteinuria because of poor adherence to medication. She was advised to take the prescribed treatment and was in remission one year later.
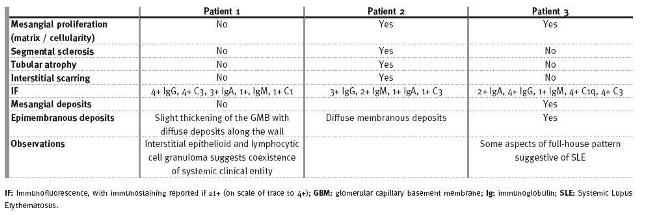
Renal biopsy features of patients with membranous nephropathy.
At the last follow-up (July 2011), five years after diagnosis, she was sixteen years old, had minimal proteinuria, no oedema and normal blood pressure (108/68 mmHg). Routine laboratory tests were normal(Table III). Serum complement C3 and C4 levels were normal. CH50 was high (57.8 U/mL, normal range: 23-46 U/mL) and autoantibodies were positive: ANA 1/640 U/ml (positive >1/160 U/mL), Anti-SSA 297 U/mL (positive >10 U/ml). She remained on treatment with low-dose prednisolone, ciclosporin, enalapril, dipyridamole and a salt-free diet (Table III).
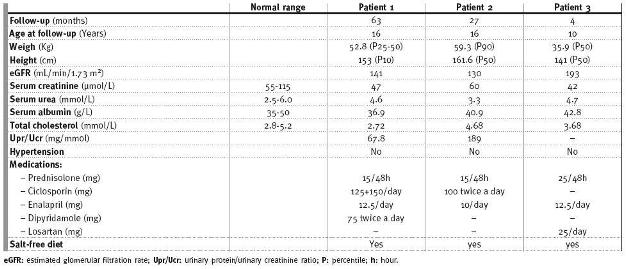
Patient outcomes (at last follow-up visit).
Patient 2(P2)
A thirteen-year-old girl with NS diagnosed in April 2009 after presenting with seven days of peripheral oedema (bilateral ankle and eyelid) and compatible abnormal laboratory tests: low serum albumin, high total cholesterol, urinalysis with 3+ proteinuria and only a trace of blood (Table I). Full blood count, renal function, serum electrolytes, serum complement levels, serum immunoglobulin levels, anti-streptolysin O titre were normal. ANA and anti-DNA were negative. At presentation, blood pressure was 134/96 mmHg (systolic 95-99th percentile, diastolic >99th percentile).
She was admitted to hospital and treated with a salt-restricted diet and corticosteroids. After five doses of methylprednisolone (750 mg every 48 hours), and five weeks of daily prednisolone (60 mg/m2/day) and enalapril (5 mg/day), proteinuria persisted. About eight weeks after diagnosis, she underwent renal biopsy that revealed histopathological features compatible with idiopathic MN (Table II). Ciclosporin (150 mg twice a day) was started and four months later her urine was negative for protein. During follow-up, she had two episodes of cystitis, both accompanied by gross haematuria, which were treated with cefuroxime axetil.
She remained in remission for 22 months and, at her last visit (July 2011), she was sixteen years old and was asymptomatic with normal blood pressure. However, proteinuria was detected (Upr/Ucr 189 mg/mmol) and the suspicion of poor adherence to medication was confirmed by a low serum ciclosporin level (16 ng/mL; therapeutic level: 100-400 ng/mL). She had normal C3 (1.14 g/L) and C4 (0.267 g/L), high CH50 (59.6 U/mL) and negative autoantibodies (ANA, ENA). Other laboratory tests, shown in Table III, were normal. She remained on treatment with prednisolone, ciclosporin, enalapril and a salt-free diet (Table III).
Patient 3(P3)
A nine-year-old girl followed in the Paediatric Nephrology clinic since the age of three (2006) with a history of four episodes of gross haematuria and persistent microscopic haematuria, and a probable diagnosis of IgA nephropathy. At five years of age, she developed nephrotic-range proteinuria with normal serum albumin, immunoglobulin A and renal function, marginally low complement C3, negative autoantibodies (ANA, ENA, ANCA) and normal renal ultrasound (Table I). After an initial response to enalapril (5 mg/day), proteinuria increased again. Enalapril dose was progressively increased (maximum 12.5 mg/day) and losartan (25 mg/day) was added but proteinuria persisted (minimum of 12 mg/m2/hour). She never had hypertension or oedema. Renal function remained normal, as did serum albumin and total serum cholesterol. The slightly low complement C3 level persisted but C4 and CH50 remained normal and autoantibodies remained negative.
In July 2010, because of persistent nephrotic-range proteinuria (53 mg/m2/hour) and low complement C3, it was decided to perform a renal biopsy. This procedure had to be delayed because of an episode of ventricular extrasystoles and bradycardia during induction of anaesthesia. Cardiac evaluation (echocardiogram, electrocardiogram and Holter) was normal. Seven months later (March 2011), it was possible to perform a renal biopsy. This revealed histopathological features of MN (Fig. 1 & Table II) with a full-house pattern on immunofluorescence microscopy suggestive of SLE. ANA remained negative. Oral prednisolone (36 mg/m 2/day) was added to enalapril and losartan therapy. Three months later she was in remission and prednisolone dose was decreased to 30 mg every 48 hours.
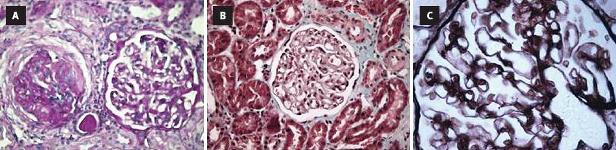
Figure 1
Histophatological features of renal biopst from Patient 3: A) Eosin staining showing glomerulus with sclerosis on the left, and glomerulus with thickening basement on the right; B) Trichrome staining showing thinckening of basement membrane and projection of podocytes into Bowman's space; C) Silver staining showing thinckening of glomerular basement membrane and double-contour appearance.
At her last visit (July 2011), she was ten years old, had no symptoms, normal blood pressure, no proteinuria (3 mg/m2/hour) and no haematuria. Laboratory tests were normal (Table III). She remained on treatment with prednisolone, enalapril and losartan (Table III).
DISCUSSION
MN can occur in the first decade of life and some paediatric series have an average age of 9.6>±4.6 years (range: 4-17 years )4. In our cases, mean age at diagnosis of MN was 11.7 years (range: 10-13 years), but if we consider the age at initial development of symptoms, MN may have occurred much earlier (at 3-5 years old) in P3. All our patients were female but there is usually no gender predominance2,4.
The majority of patients with idiopathic MN present with NS1,3, as occurred in two of our cases (P1 and P2). In previous paediatric series, the diagnosis of MN has been made in the context of NS in 74%-75% of cases1,5, oedema in 37%1, haematuria/proteinuria in 17%5 and asymptomatic proteinuria in 8%<5. At onset, P1 and P2 had NS, and P3 had a history of episodes of gross haematuria and nephrotic-range proteinuria. Patient 2, with NS, also had hypertension and microscopic haematuria. Hypertension at onset is uncommon in previous series3. The reported incidence of microscopic haematuria in children with MN is between 15% and 80%, and of gross haematuria is between 6% and 20%1.
In our patients, renal biopsy was performed because of steroid-resistant NS/persistent proteinuria. In two of the cases (P1 and P3), histopathological features were suggestive of an underlying systemic disease, although until that point there were no other clinical manifestations or laboratorial abnormalities suggestive of a secondary cause. All our patients had extensive screening for possible causes of secondary MN, as many infectious diseases (bacterial, viral or parasitic), immunological conditions (particularly SLE), abnormalities of the urinary tract, tumours and a variety of other pathologies have been associated with MN in childhood1.
In P1, with typical histopathological features of MN, there was the suspicion of DLE because of discoid skin facial lesions and positive autoantibodies that appeared several months after the initial diagnosis. This emphasises the importance of continuing to look for manifestations of underlying systemic diseases because there are other reported cases with typical pathologic features of idiopathic MN that turned out to have lupus membranous nephritis3. In P3, renal biopsy showed a full-house pattern suggestive lupus membranous nephritis, even though there were no other manifestations of SLE. We are continuing to monitor for signs of SLE.
There is no clear consensus about the most appropriate therapy for childhood MN. Treatment with immunosuppressive agents has not yet been studied adequately in children though it is used in adults with good results3. A small number of uncontrolled studies have reported that oral corticosteroids alone appear to be ineffective in childhood MN3 but P3 achieved remission after three months of oral prednisolone along with angiotensin converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs), although the follow-up period for this patient is limited. Some studies suggest that the combination of daily oral steroids and ciclosporin may be effective in patients with steroid-resistant idiopathic MN with NS3. Patients 1 and 2, with steroid-resistant NS, were treated in this way and achieved remission in less than three months. The use of ACE inhibitors and ARBs for persistent proteinuria is usually beneficial in MN5.Our patients were all treated with at least one of these drugs although benefits were uncertain as we had to add immunosuppressive agents.
The clinical course of childhood idiopathic MN is variable, with overall remission rate of 26%-52% and rates of progression to chronic renal insufficiency of 10%-28%3. Multiple studies have shown that the condition has a more favourable course in children than in adults1,2. A recent study showed that age less than nine years old and normal blood pressure at the time of onset were associated with a better prognosis but did not show any correlation between initial oedema, proteinuria, low serum albumin level or hypercholesterolemia and subsequent course of disease2. In several other uncontrolled studies in children, age, initial presentation with NS, hypertension at onset and high-grade pathological stages were considered to be poor prognostic factors3.
At last follow-up all our patients were asymptomatic and had normal blood pressure and normal renal function with a mean eGFR 154.6 mL/min/1.73 m2 (130-193 ml/min/1.73 m2). Only P2 had some degree of proteinuria (subnephrotic) due to poor adherence to medication. All were still on treatment with low dose of prednisolone, and P1 and P2, who had NS initially, were also taking ciclosporin. However, the achievement of remission should not be considered as a cure in idiopathic MN, and long-term follow-up is required3. Of our cases, at least one (P1) and possibly another (P3), had atypical features suggestive of an underlying cause and could have secondary MN.
CONCLUSION
MN is a common cause of NS in adulthood, but not in children. It should, however, be considered among the differential diagnoses in children or adolescents with asymptomatic proteinuria or NS which is unresponsive to steroid treatment. Making the diagnosis and managing idiopathic MN in children can be challenging as this is a rare entity with varying presentations and an inconsistent response to treatment. ACE inhibitors, ARBs, corticosteroids and other immunosuppressive drugs such as ciclosporin may be required. All patients with idiopathic MN should be monitored carefully for covert underlying systemic diseases.
References
1 De Giovanni EB, Madile BM. Síndrome nefrótico por glomerulonefritis membranosa en la infancia. Arch Argent Pediatr 2004;102:296-300 [ Links ]
2 Menon S, Valentini RP. Membranous nephropathy in children: clinical presentation and therapeutic approach. Pediatr Nephrol 2010 ;25:1419-1428 [ Links ]
3 Lee BH, Cho HY, Kang HG, et al. Idiopathic membranous nephropathy in children. Pediatr Nephrol 2006 ;21:1707–1715 [ Links ]
4 Chen A, Frank R, Vento S, et al. Idiopathic membranous nephropathy in pediatric patients: presentation, response to therapy, and long-term outcome. BMC Nephrology 2007 ;8:11 [ Links ]
5 Valentini RP, Tej K. Mattoo TK, Kapur G, Imam A. Membranous glomerulonephritis: treatment response and outcome in children. Pediatr ephrol 2009;24:301-308 [ Links ]
Hospital Pediátrico Carmona da Mota
Centro Hospitalar de Coimbra
Av. Afonso Romão
Santo António dos Olivais
3000-602 Coimbra, Portugal
E-mail: susananobre14@gmail.com
Conflict of interest statement None declared.
Received for publication:23/09/2011
Accepted in revised form:12/12/2011

