










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.27 no.1 Lisboa jan. 2013
Atheroembolic renal disease as a cause of allograft primary non-function
Doença ateroembólica como causa de disfunção primária do enxerto renal
Helena Viana1,2,3, Carina Ferreira2,3, Fernanda Carvalho1,3, Ana Rita Santos1, Maria João Galvão1, Francisco Remédio2, Fernando Nolasco2,3
1 Kidney Morphology Laboratory, Department of Nephrology, Hospital Curry Cabral, Lisbon, Portugal
2 Kidney Transplant Unit, Department of Nephrology, Hospital Curry Cabral, Lisbon, Portugal
3 CEDOC – Faculty of Medical Sciences, Universidade Nova de Lisboa, Lisbon Portugal
ABSTRACT
Atheroembolic renal disease, also referred to as cholesterol crystal embolization, is a rare cause of renal failure, secondary to occlusion of renal arteries, renal arterioles and glomerular capillaries with cholesterol crystals, originating from atheromatous plaques of the aorta and other major arteries. This disease can occur very rarely in kidney allografts in an early or a late clinical form.
Renal biopsy seems to be a reliable diagnostic test and cholesterol clefts are the pathognomonic finding. However, the renal biopsy has some limitations as the typical lesion is focal and can be easily missed in a biopsy fragment.
The clinical course of these patients varies from complete recovery of the renal function to permanent graft loss. Statins, acetylsalicyclic acid, and corticosteroids have been used to improve the prognosis. We report a case of primary allograft dysfunction caused by an early and massive atheroembolic renal disease. Distinctive histology is presented in several consecutive biopsies. We evaluated all the cases of our Unit and briefly reviewed the literature.
Atheroembolic renal disease is a rare cause of allograft primary non -function but may become more prevalent as acceptance of aged donors and recipients for transplantation has become more frequent.
Keywords: Allograft; atheroembolism; cholesterol; kidney.
RESUMO
A doença ateroembólica renal, é uma causa rara de falência renal, sendo secundária à oclusão das artérias renais, arteríolas e/ou glomérulos por cristais de colesterol com origem em placas de ateroma da aorta ou outras grandes artérias. Esta doença é, ainda mais raramente, causa de falência de enxerto renal, com manifestações precoces ou tardias.
A biópsia renal permite um diagnóstico específico, através da identificação das fendas de colesterol, patognomónicas desta patologia. No entanto, a biópsia apresenta limitações já que as lesões são focais e podem estar ausentes no fragmento renal.
A evolução clínica varia desde a completa recuperação até a permanente perda de função renal. As estatinas, o ácido acetilsalicílico e os corticóides têm sido utilizados de forma a melhorar o prognóstico. Descrevemos um caso de disfunção primária de enxerto renal causada por extensa doença ateroembólica. As lesões específicas desta patologia são apresentadas, em sucessivas fases de evolução e em diversas biópsias. Reavaliámos os casos da nossa unidade de transplantação e revemos brevemente a literatura.
A doença ateroembólica é uma causa rara de disfunção primária do enxerto mas provavelmente tornar-se-á mais prevalente com o aumento da idade dos dadores/receptores aceites para transplantação.
Palavras-chaves: Ateroembolismo; Colesterol; Enxerto; Rim.
INTRODUCTION
Atheroembolic renal disease (AD) also referred to as cholesterol crystal embolization (CE) is a renal failure form that is secondary to occlusion of renal arteries, renal arterioles, and glomerular capillaries with cholesterol crystals1. It may rarely occur in renal allografts, in association with atherosclerosis. The source of emboli may be either the donors or the recipients vessels. This disease can occur as an early or a late cause of impaired renal allograft function and can be a rare cause of primary allograft dysfunction2,3.
Renal biopsy is regarded as the definitive method for diagnosis1; however, the typical lesion (i.e., arterial and capillaries blockage) usually is focal and can easily not be included in the biopsy fragment4.
We report a case of primary kidney allograft dysfunction caused by AD. The distinctive histology is presented in several consecutive biopsies. We reevaluated the renal cases of our Unit and briefly reviewed the literature.
CASE REPORT
A 51-year-old white female, with end-stage renal failure secondary to chronic pyelonephritis, underwent her first renal transplant. She had been on haemodialysis for 10 years, with panel reactive antibody of 12%.
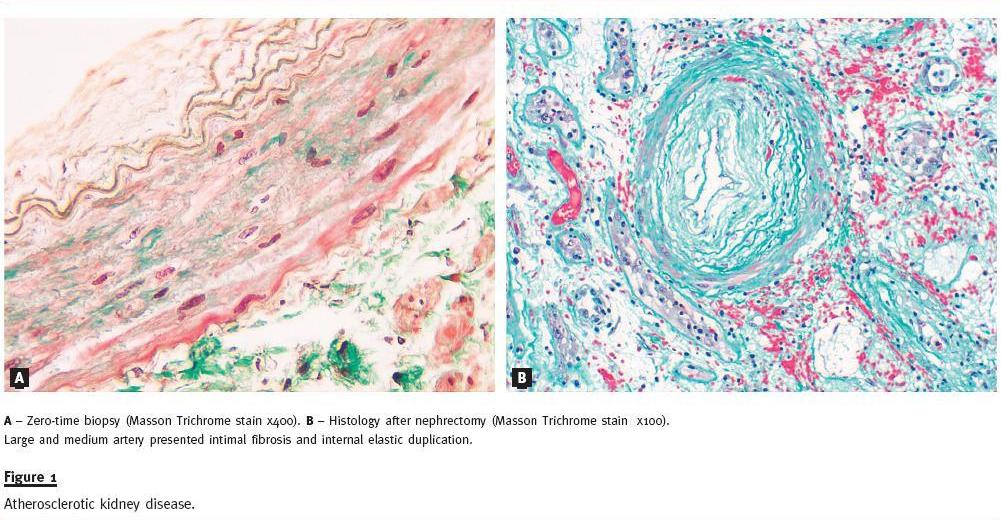
The donor was a 56-year-old male, heavy smoker, with uncontrolled hypertension, deceased for cerebrovascular accident with haemorrhagic transformation. The surgical procedure was uneventful with cold and warm ischemia times of 17 h.20 min and 45 min., respectively. The surgeon described immediate diuresis, but noted a normal venous filling with some reduced organ perfusion. Zero-time biopsy was done with a semi-automatic 16G needle after arterial anastomosis. This biopsy revealed three glomeruli: one globally sclerosed and two normal. The fragment showed normal tubule-interstitial structure and an arciform artery with important intimal fibrous proliferation (Fig. 1A). Basiliximab (20 mg IV once) and metilprednisolone (500mg IV for 3 days) were used for induction immunosuppression. Maintenance immunosuppression consisted of tacrolimus (0.15 mg/kg/day), mycophenolate mophetil (1000 mg 12/12 hours) and prednisolone (20 mg/day).
At 24 hours, the patient presented allograft pain with diuresis reduction. The creatinine remained high (6.5 mg/dl) and the white cell count showed 11300/mm3 leucocytes without eosinophylia. Doppler ultrasound revealed renal artery and interlobular arteries systolic flow reduction and total lack of end-diastolic perfusion. The renal vein was permeable. At this time, low molecular weight heparin at anticoagulant therapeutic range was started, and tacrolimus was replaced by anti-thymocyte globulin, in order to maintain immunosuppression and reduce nephrotoxicity.
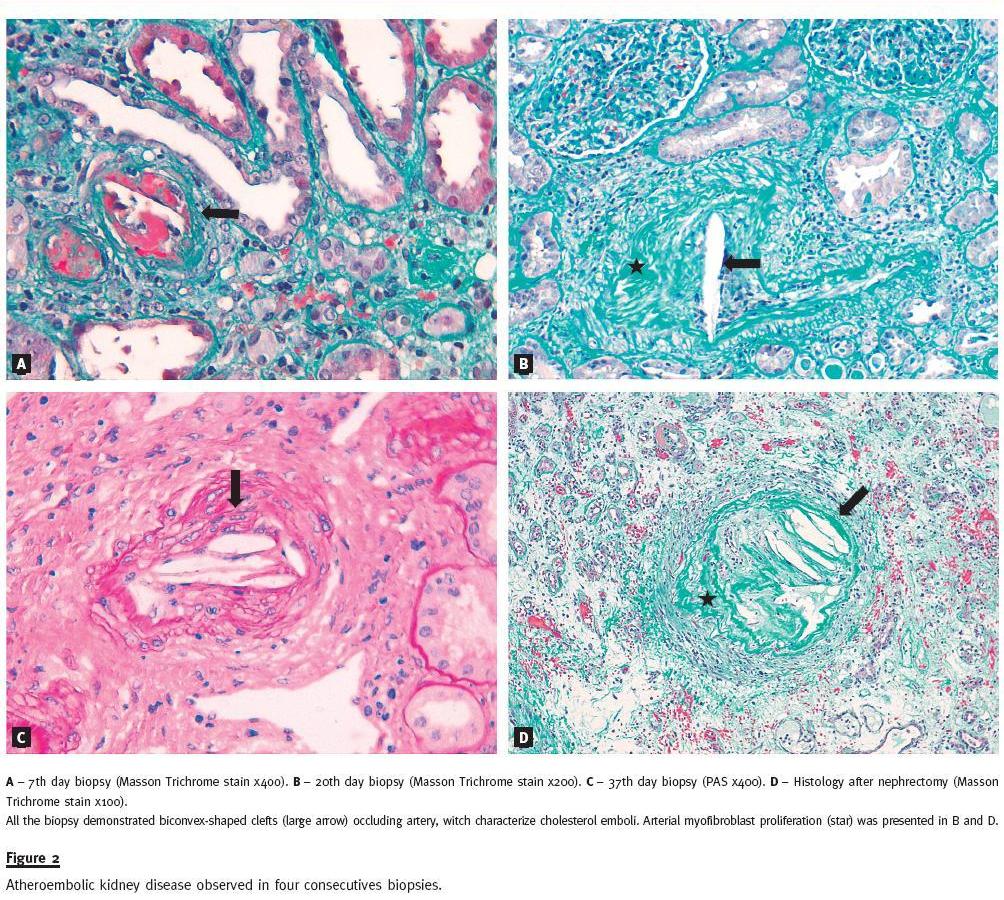
Seventh day biopsy revealed atheroembolic nephropathy (Fig. 2A) and acute tubular necrosis. The fifteenth day Doppler ultrasound showed a global reduction of allograft vascularization, with slight improvement of systolic and diastolic flow in the renal artery and interlobular arteries. At the eighteenth day, donor specific anti-HLA antibodies were detected by Luminex® with a negative crossmatch by flow cytometry. At day 20, a new allograft biopsy showed acute rejection mediated by T-cells Banff IA superimposed in atheroembolic nephropathy (Fig. 2B).
Methilprednisolone pulses (500mg/ IV in 3 consecutive days) were administrated, followed by seven days of intravenous immunoglobulin. The patient reached a diuresis of 1500 ml/day with 4.2 mg/dl of creatinine, requiring 2 haemodialysis sessions per week. The fourth biopsy, performed at the 37th day, demonstrated again cholesterol crystal embolization in medium arteries (Fig.2C). At this time, the fragment showed ischemic glomeruli, tubular atrophy and interstitial fibrosis around the occluded vessels. Some areas presented acute tubular necrosis. Tacrolimus was replaced by sirolimus. The patients clinical status did not change in the next two weeks and another biopsy at 54 post-transplant days was done before discharge. This biopsy showed cortical necrosis.
The patient returned to ambulatory haemodialysis (two sessions/week), under sirolimus, mycophenolate of mophetil, prednisolone, statins and aspirin. In the following weeks, there was increased diuresis with effective azotemia reduction.
Haemodialysis was stopped at day 120 after transplantation, with an estimated GFR of 20ml/min/1.73 m2.
Ten months after transplantation, the patient resumed haemodialysis. Nine months later, she was submitted to allograft nephrectomy for toxic rejection.
Microscopy confirmed severe atherosclerosis and the presence of cholesterol crystal embolization in major arteries (Figs Figure 2D and 1B).
DISCUSSION
Atheroembolic disease is rare in renal allografts.
Ripple et al. reported 7 cases among 1500 renal transplant biopsies (0.47%) performed at the Johns Hopkins Hospital, between 1984 and 19995, Modi et al.4 review 200 renal transplant biopsies carried out, between 1990 and 1995, and found 2 cases of cholesterol embolism (1%). Lai et al.6 reported that among 5435 renal allograft biopsies, 19 from 12 cadaveric transplants (median age = 63 years) had AD (0.2%).
In our Unit we found four AD diagnosis (0.21%) among 1841 allograft biopsies. Three of the four biopsies belong to this case. The other biopsy is from a patient with a chronic allograft dys function.
Some authors7-9 believe that cholesterol embolic disease is probably an under-reported cause of renal graft dysfunction. Meyrier7 postulates that allograft AD is more common in transplantation and often misinterpreted as acute/chronic rejection or calcineurin inhibitor toxicity.
Cholesterol embolization: early vs. late form; donor vs. receptor origin.
Renal cholesterol embolization can occur immediately before transplantation to 15 years post-transplantation7.
However, two important clinical presentations1 can be distinguished: early vs. late.
Primary dysfunction is commonly related to acute tubular necrosis; technical complications, such as arterial or venous renal thrombosis, ureteric obstruction or, rarely, hyperacute rejection. Nowadays, cholesterol embolization should also be considered in the differential diagnosis of early3 allograft dysfunction. In these early cases, emboli are frequently released from the donors arteries before or during organ harvesting. More rarely, early embolizations are originated from the recipients atheromatous vessels during anastomosis. The early cases are essentially confined to the allograft, with less systemic manifestations.
The late clinical presentation can arise several years after transplantation, in stable grafts, where emboli often originate in the recipients vessels. One of the largest known series of AD in renal allograft6, a clinicopathological study of 12 cases, recognizes a recipient vs. donor origin ratio of 3:1.The late form of the disease is usually associated with the same mechanisms and risk factors as for the general population. Ulcerated aortic atherosclerotic plaques are stabilized by thrombus formation10.
Therefore, any thrombus disruption increases the risk of embolization. The plaque trauma can result from direct instrumentation: angiographic catheters or surgical manipulation. Anticoagulants or thrombolytic agents that interfere with thrombus stability can also be responsible for cholesterol embolization1,4. Some times this late form can assume the same features of a systemic disorder, with multiple organ manifestations.Histology
The pathognomonic finding in biopsy specimens10 is the biconvex, needle-shaped cholesterol cleft. The crystals are normally dissolved during histological routine preparation, therefore, the cholesterol embolus3 appears as characteristic clefts or ghosts (Fig.2). The medium-sized arterioles (150 to 200 μ
We think that the primary allograft dysfunction of our patient was caused by an early cholesterol embolization.
The clinical data and the observation of zero-time biopsy suggested that the donor had severe and generalized atherosclerotic disease, so, probably the embolization originated in the donor. This atherosclerotic disease was later confirmed by nephrectomy.
The surgical manipulation of the pre-existing donor atherosclerotic vessels was almost certainly the cause of the cholesterol embolization to the kidney allograft. Early after arterial anastomosis, the surgeon noted a reduction of allograft perfusion.
The diagnosis of typical histological lesions at the first week confirms without doubt the early form of AD. The clinical disease was confined to the allograft, without systemic manifestations, which is more usual in the early form. The acute tubular necrosis described at the seventh day biopsy and not present in the zero-time biopsy could be a histological feature of AD. The presence of cholesterol emboli in kidney vessels was documented in three consecutive biopsies and in the microscopy of nephrectomy. These observations indicated massive embolization with a widespread area of disease.
Prognosis and therapy
In native kidney, AD has been associated with poor renal and patient survival. Scolari et al.13 followed 354 incident cases in native kidneys confirmed by histology or ophthalmoscopy until dialysis and death (mean follow-up time of 24 months). By the end of followup, 32.7% of patients were on dialysis; 1-year and 2-year patient survival were 83% and 75%, respectively.
In allograft kidney, the clinical course of the disease also varies from complete recovery of renal function to permanent graft loss3. Several authors7,11,12 conclude that AD with a recipient origin have better graft survival than AD with donor origin, that has a higher rate of graft dysfunction and subsequent graft loss. Graft failure is significantly associated with donor-derived and early AD3,6. The reason for this difference may be the more extensive AD developing in an atherosclerotic cadaveric donor during organ procurement or severe trauma leading to death5.
Since the current tendency is to accept older donors and older recipients, with more advanced atherosclerotic disease, this condition is likely to become frequent in the future3,11-13. Particular care must also be taken during the evaluation of organ donors13. The vast majority of atheroemboli appear to originate from aortic atherosclerotic plaques, and it seems reasonable to avoid manipulation of the aorta as much as possible at implantation time3,13.
The sources of therapeutic indications are from few longitudinal studies and some clinical data. There is no consistent data about therapy in allograft AD.
For the late manifestations, restricting indications for angiography and surgical procedures in atherosclerotic patients is important. Option for non-invasive diagnostic methods, such as MR angiography or computer-assisted tomographic angiography, could in part obviate the risk for catheter-induced embolization1. Scolari et al.13 demonstrated that statin use was associated with better outcome when already in place at the time of AD diagnosis and when initiated after diagnosis. These drugs mediate plaque stabilization and regression through lipidlowering and anti-inflammatory mechanisms, lowering risk for further embolization14. There is some rationale for the use of acetylsalicyclic acid, which attenuates platelet activation via cyclooxygenasedependent pathways. Activation of complement (particularly C5) by cholesterol crystals in vitro and the clinical observation of low serum complement and peripheral eosinophilia strongly suggest a possible role for inflammation in the pathogenesis of AD3. If inflammation surrounding the cholesterol emboli is indeed the cause of progressive renal failure, there could be a potential role for the use of steroids in this disease. Some authors recommended the usage of low-dose corticosteroids15,16.
Other authors17 noted improvement after the use of high-dose corticosteroids. However, use of steroids was not associated with outcome in the study of Scolari et al.13.
There are numerous reports in the literature from experiments clearly showing an atherogenic effect of cyclosporine (CsA), by induction of endothelial dysfunction, endothelial cell injury, and arterial arteritis18.
The literature regarding tacrolimus is sparse; nevertheless, a paper describes an important role for hydrogen peroxide in the tacrolimus nephrotoxicity19.
Calcineurin-inhibiting (CNI) agents have been shown to induce oxidative stress while mycophenolate mofetil (MMF) has been shown to even ameliorate oxidative stress20.
Consequently, application of CNI-free protocols in older patients receiving older organs appears to be the treatment of choice.
Autophagy is a protective mechanism involving degradation of oxidative intracellular material that occurs in atherosclerotic plaques. The regulation is dependent of mammalian target of rapamycin (mTOR), so that mTOR inhibitors activate autophagy and stabilize advanced atherosclerotic plaques21. These findings provide a rationale for the use of rapamycin or analogs in atheroembolic disease.
The use of protocol based in MMF and mTOR inhibitors without CNI seems more adequate in atherosclerotic patients receiving atherosclerotic organs.
Our patient presented extensive embolization of donor origin, in an allograft with chronic vascular lesions. The donor-derived and early AD dictated a poor prognosis and a diminutive probability of allograft recovery. The superimposed acute T-cell mediated rejection worsened the already poor basal allograft prognosis. The observations of cortical necrosis indicated lack of perfusions in some kidney areas. We used a statin, acetylsalicyclic acid and a more adequate immunosupressive protocol (high-dose corticosteroids, sirolimus and MMF without CNI) to improve allograft prognosis, without success.
CONCLUSIONS
In AD manifested as primary allograft dysfunction, emboli are frequently released from the donors arteries before or during organ harvesting. More rarely, early embolizations are originated from the recipients atheromatous vessels during the anastomosis.
Atheroembolic disease is liquely to become more frequent in the future since donors and receptors are more olders and have more advanced atherosclerotic disease.
The vast majority of atheroemboli appear to originate from aortic atherosclerotic plaques, and it seems reasonable to avoid manipulation of the aorta as much as possible at implantation time.
REFERENCES
1. Scolari F, Ravani P. Atheroembolic renal disease. Lancet 2010; 375(9726):1650-1660. [ Links ]
2. Bellamy CO, Paul AB, Fleming S. Primary non-function of a renal allograft due to atheromatous emboli. Nephrol Dial Transplant 1994; 9(2):182-184. [ Links ]
3. Bolander JE II, Carter CB. Cholesterol embolization in renal allografts. J Am Soc Nephrol 1996; 7(1):18-22. [ Links ]
4. Modi KS, Rao VK. Atheroembolic renal disease. J Am Soc Nephrol 2001; 12(8):1781-1787. [ Links ]
5. Ripple MG, Charney D, Nadasdy T. Cholesterol embolization in renal allografts. Transplantation 2000; 69(10):2221-2225. [ Links ]
6. Lai CK, Randhawa PS. Cholesterol embolization in renal allografts: a clinicopathologic study of 12 cases. Am J Surg Pathol 2007;31(4):536-545. [ Links ]
7. Meyrier A. Cholesterol crystal embolism: diagnosis and treatment. Kidney Int 2006; 69(8):1308-1312. [ Links ]
8. Scolari F, Tardanico R, Pola A, et al. Cholesterol crystal embolic disease in renal allografts. J Nephrol 2003; 16(1):139-143. [ Links ]
9. de Takats DL, Pollock LE, ODonnell PJ, Snowden S, Bewick M, Scoble JE. Is cholesterol embolic disease an unrecognized cause of renal graft dysfunction? Nephrol Dial Transplant 1996; 11(7):1325-1327. [ Links ]
10. Modi KS, Rao VK. Atheroembolic renal disease. N Engl J Med 1969; 280(15):812-818. [ Links ]
11. Modi KS, Rao VK. Atheroembolic renal disease. J Am Soc Nephrol 2001; 12(8):1781-1787. [ Links ]
12. Hammerschmidt DE, Greenberg CS, Yamada O, Craddock PR, Jacob HS. Cholesterol and atheroma lipids activate complement and stimulate granulocytes. A possible mechanism for amplification of ischemic injury in atherosclerotic states. J Lab Clin Med 1981; 98(1):68-77. [ Links ]
13. Scolari F, P, Gaggi R, et al. The challenge of diagnosing atheroembolic renal disease: clinical features and prognostic factors. Circulation 2007; 116(3):298-304.
14. Woolfson RG, Lachmann H. Improvement in renal cholesterol emboli syndrome after simvastatin. Lancet 1998; 351(9112):1331–1332. [ Links ]
15. Nakayama M, Nagata M, Hirano T, et al. Low-dose prednisolone ameliorates acute renal failure caused by cholesterol crystal embolism. Clin Nephrol 2006;66(4):232-239. [ Links ]
16. Dahlberg PJ, Frecentese DF, Cogbill TH. Cholesterol embolism: experience with 22 histologically proven cases. Surgery 1989; 105(6):737–746. [ Links ]
17. Takahashi T, Konta T, Nishida W, Igarashi A, Ichikawa K, Kubota I. Renal cholesterol embolic disease effectively treated with steroid pulse therapy. Intern Med 2003; 42(12):1206-1209. [ Links ]
18. Land WG. Ageing and immunosuppression in kidney transplantation. Exp Clin Transplant 2004;2(2):229-237. [ Links ]
19. Zhou X, Yang G, Davis CA, et al. Hydrogen peroxide mediates FK506-induced cytotoxicity in renal cells. Kidney Int 2004; 65(1):139-147. [ Links ]
20. Lui SL, Chan LY, Zhang XH, et al. Effect of mycophenolate mofetil on nitric oxide production and inducible nitric oxide synthase gene expression during renal ischemiareperfusion injury. Nephrol Dial Transplant 2001; 16(8):1577-1582. [ Links ]
21. Schrijvers DM, De Meyer GR, Martinet W. Autophagy in atherosclerosis: a potential drug target for plaque stabilization. Arterioscler Thromb Vasc Biol 2011; 31(12):2787-2791. [ Links ]
Helena Maria Morais de Sousa Viana
Department of Nephrology, Hospital Curry Cabral
Rua da Beneficência, nº 8, 1069-166
Lisboa, Portugal
E-mail: viana.helena@gmail.com
Conflict of interest statement: None declared
Received for publication: 06/01/2013
Accepted in revised form: 11/02/2013


{kind=link}
{kind=link}