










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.27 no.2 Lisboa abr. 2013
Management of hyperglycaemia in type 2 diabetic patients with Chronic Kidney Disease
Tratamento da hiperglicémia nos doentes diabéticos tipo 2 com Doença Renal Crónica
Sílvia Coelho, Patrícia Carrilho, Luís Inchaustegui
Department of Nephrology, Hospital Fernando da Fonseca EPE, Amadora, Portugal
ABSTRACT
Diabetes is an increasingly common disease with an important negative impact on patients morbidityand mortality, being the main cause of end stage renal disease. Management of the diabetic patient with chronic kidney disease poses additional challenges, namely with respect to defining glycaemic targets and in the therapeutics employed to achieve them. The authors review the state of the art evidence about the use of antihyperglycaemic agents in type 2 diabetes, from the perspective of a chronic kidney disease patients health care provider.
Keywords: Chronic kidney disease; diabetes; hypoglycaemic agents
RESUMO
A diabetes é uma patologia com uma prevalência crescente, que condiciona um importante impacto negativo na morbilidade e mortalidade dos doentes, sendo a principal causa de doença renal crónica terminal.
O tratamento da diabetes no doente com doença renal crónica implica desafios adicionais nomeadamente em relação à definição dos alvos glicémicos e da terapêutica utilizada para os atingir. Os autores fazem uma revisão sobre o estado da arte da utilização dos agentes hipoglicimiantes na diabetes tipo 2 na perspectiva do profissional de saúde responsável por doentes com doença renal crónica.
Palavras-chave: Agentes hipoglicemiantes; diabetes; doença renal crónica
INTRODUCTION
Diabetes is a global public health problem and epidemiologists estimate an increase in world prevalence from 6.4% to 7.7% in the next 20 years, accounted particularly by developing countries1. In Portugal, the prevalence of diabetes was estimated at 11.7%, being more frequent in men (14.2%) than women (9.5%) and increasing with age2.
Diabetes has an important negative impact in morbidity and mortality, remaining a leading cause of cardiovascular disorders, blindness, amputations, and hospitalizations3. Data suggest that the risk of nephropathy is currently equivalent in the two types of diabetes, affecting approximately one third of diabetics and being the most common cause of end-stage renal disease (ESRD) worldwide4. The treatment approach to diabetes should be multidisciplinary, implying lifestyle modifications, control of body weight, blood pressure, dyslipidaemia, associated comorbidities and, of course, glycaemic blood values3. It poses an increasing economic burden in an increasingly economically fragile society, and optimization of resources is mandatory.
Chronic kidney disease (CKD) patients, for reasons that will be detailed below, have contraindications to many of the currently available oral antihyperglycaemic agents, making glycaemic control even more challenging. Knowledge of these absolute and relative contraindications allows us to make a more rational use of the available drugs, achieving the most favourable risk/benefit profile and, concomitantly, better clinical outcomes.
In this paper, we will review the optimal glycaemic targets for the CKD type 2 diabetic patient and discuss the therapeutics currently available to achieve them.
WHAT IS THE GLYCAEMIC GOAL IN CKD PATIENTS?
Two primary techniques are available to assess the effectiveness of the management plan on glycaemic control: self -monitoring of blood glucose and haemoglobin A1c3.
Evidence that achieving an haemoglobin A1c (HbA1c) level of 7.0% is able to prevent the microvascular complications of types 1 and 2 diabetes in the general population, has long been evident from studies, such as the Diabetes Control and Complications Trial (DCCT)5 and the United Kingdom Prospective Diabetes Study (UKPDS)6,7. Three recent studies (ADVANCE, ACCORD, VADT)8-10 have revealed that even more intensive glycaemic control (HbA1c 6.5%) further reduces the development of elevated albuminuria in patients with type 2 diabetes, although none showed significant benefits on creatinine-based estimates of glomerular filtration rate (eGFR).
Less is known about appropriate glycaemic control in patients with diabetes and more advanced CKD, because no prospective, randomized clinical trials evaluating the level of glycaemic control on health outcomes have been carried out in patients with CKD stages 3 -5. Nevertheless, several observational studies showed that higher levels of haemoglobin A1c were associated with higher death rates in patients with diabetes and chronic kidney disease after adjusting for markers of inflammation and malnutrition11,12. Therefore, although there is need for a much better understanding of the CKD-related characteristics of diabetes mellitus, glycaemic control can still be argued to be beneficial in preventing complications, even in dialysis-dependent patients13.
However, another important factor to be taken into account is the inaccuracy of the HbA1c measurement in reflecting serum glucose concentrations in this population. Studies have shown that glucose levels in CKD patients are higher than expected for given HbA1c levels, and this is most marked in those on dialysis14,15. Factors that may contribute to falsely decreased values of HbA1c include a reduced red blood cell lifespan, transfusions, and haemolysis.
On the other hand, falsely increased values may occur, less commonly, due to carbamylation of the haemoglobin and acidosis16. Therefore, when targeting for the ideal HbA1c in our CKD patients (mainly those on stages 4 and 5), we should bear in mind that a result of 6.5% may be equivalent to a higher value. However, care not to overtreat hyperglycaemia is particularly important in a population at increased risk of hypoglycaemia: they have a decreased clearance of insulin and of most oral agents used to treat diabetes; renal gluconeogenesis is impaired with reduced kidney mass; and many advanced CKD patients are frail, malnourished, non -ambulatory and may be less able to respond appropriately to hypoglycaemia17.
Although alternatives to HbA1c have been searched (i.e., glycated albumin, which reflects glycaemic control over a shorter period16), it still remains the best clinical marker of long -term glycaemic control despite its limitations, particularly if combined with self -monitoring of blood glucose.
In light of this knowledge, the last update of KDOQI recommendations (2012) first introduced the notion of individualized HbA1c targets. They recommended: 1) a target HbA1c of~ 7.0% to prevent or delay progression of the microvascular complications of diabetes; 2) not treating to an HbA1c target of < 7.0% in patients at risk of hypoglycaemia (advanced CKD patients were considered to be included in this group); 3) target HbA1c be extended above 7.0% in individuals with co-morbidities or limited life expectancy and risk of hypoglycaemia16.
WHAT IS THE BEST THERAPEUTIC APPROACH?
Metformin has long been recommended as the initial pharmacological therapy for type 2 diabetes, in the absence of specific contraindications, along with lifestyle interventions. This position has not been changed in the last guidelines16. However, the consensus algorithm for the initiation and adjustment of therapy proposed by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes published in 2012 was less prescriptive than prior algorithms with respect to second line therapies. The limited data on this issue was acknowledged and combination therapy with additional oral or injectable agents was considered reasonable, with the specific choice based on an integrated approach to the patient (medical, social and economical factors)18. Insulin is still frequently used, due to the progressive β-cell dysfunction that characterizes type 2 diabetes18.
Diabetic patients with chronic kidney disease (CKD) have more limited therapeutic options. The most important reason is because a reduced GFR may lead to the accumulation of renally excreted drugs and/or their metabolites and this can induce severe side effects. Moreover, uraemia differentially affects absorption and metabolic pathways in the gastrointestinal tract and liver and, therefore, can change the systemic bioavailability of drugs in a not always predictable way. The hypoalbuminaemia commonly seen in CKD patients may also interfere with protein binding-drugs total clearance and half-life19.
For these reasons, insulin therapy was previously commonly seen as the (only?) agent of choice to achieve glycaemic control in patients with CKD.
However, and albeit the persistent lack of evidence in this field, several agents, including some of the most recent drugs available, were found to be effective and safe even in patients on dialysis and may be useful therapeutic options in this population.
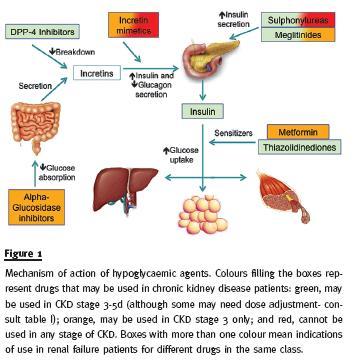
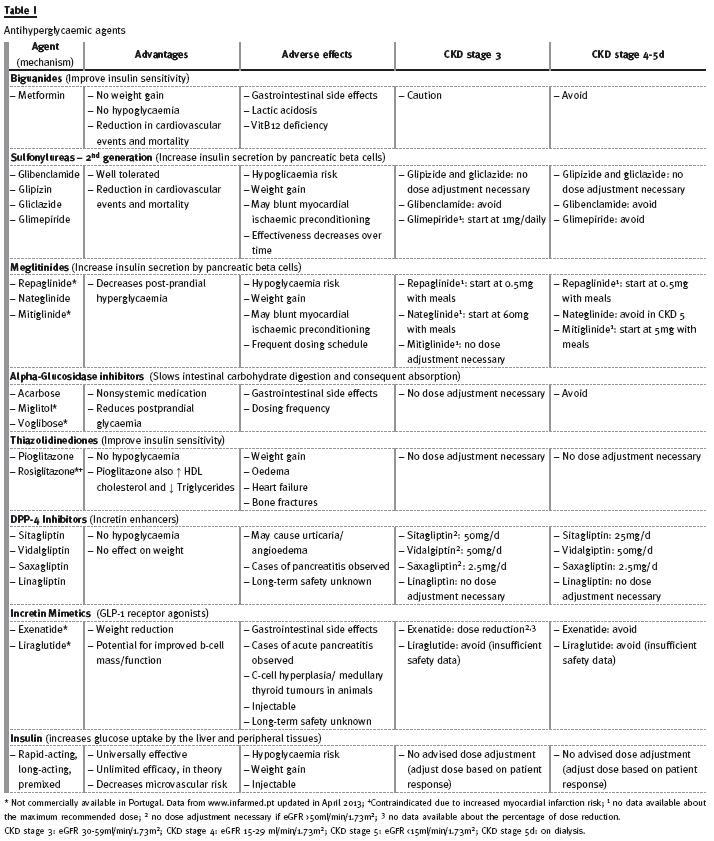
In the next section, we will review the available hypoglycaemic agents from the perspective of a type 2 diabetic CKD patients health care provider. Table I and figure 1 provide a practical summary of the mechanism of action, advantages, adverse effects and use in renal failure of antihyperglycaemic agents, discriminating those currently commercially available in Portugal.
Table I
BIGUANIDES
Nowadays, metformin is the only commercially available biguanide used in the treatment of diabetes, having been first introduced in the UK in 1957.
It acts by improving insulin sensitivity what, consequently, decreases hepatic gluconeogenesis and enhances peripheral glucose uptake. Importantly, it does not increase the risk of hypoglycaemia20.
Metformin is recommended as the first line therapy for diabetes by the international consensus guidelines due to its efficacy combined with a favourable side effect profile and low cost3,16. The UK Prospective Diabetes Study first revealed its superiority by showing a lower mortality from cardiovascular disease in overweigh patients with diabetes treated with metformin rather than sulphonylureas or insulin7. Metformin is mainly associated with minor gastrointestinal symptoms (anorexia, nausea, vomiting, diarrhoea and abdominal pain) and it may impair absorption of vitamin B12 and folic acid20.
However, it is the perceived risk of lactic acidosis in the presence of renal, hepatic, respiratory, or cardiac failure that remains one of the most important causes for patients being denied this medication21. Metformin associated lactic acidosis (MALA) is defined as the presence of lactic acidosis associated with a lactate > 5mmol/l in a patient medicated with metformin22.
Most of the evidence for the association between biguanides and lactic acidosis is historical data from phenformin21. Phenformin was in fact withdrawn from the market because of an association with fatal lactic acidosis, which was calculated to be 10-20 times greater than for metformin20. The physiopathology of MALA is complex and mostly unclear.
Metformin has been proposed to increase lactate production through an intracellular shift to anaerobic metabolism and impair lactate clearance by the liver23. This would become particularly relevant in cases of accumulation of metformin (i.e., in renal insufficiency, as the drug main route of elimination is renal tubular secretion) or increased lactate production (i.e., inadequate tissue delivery of oxygen or excessive tissue oxygen demand).There are many published case reports that describe an association between metformin and lactic acidosis22, 24 -26.
However, they have been highly criticised because it remains difficult to establish the exclusive role of metformin as the cause of lactic acidosis, as most patients were admitted with other causes of increased lactate, such as sepsis, dehydration or cardiac heart failure. Moreover, the lack of a relation between lactic acid/metformin concentrations and mortality and the absence of an association between metformin concentration and lactic acid concentration (that was proved to exist in the case of phenformin) made some investigators suggest that the association between lactic acido sis and metformin is coincidental27-29. A Cochrane review of 206 comparative trials and cohort studies in patients with type 2 diabetes who were treated with metformin, found no evidence of increased risk of develop ing fatal or non-fatal lactic acidosis in the subgroup of metformin treated patients. However, these studies did not include patients who had contraindications for the use of metformin and so nothing could be concluded about the risk of MALA in this subpopulation30.
Nevertheless, there are clinical studies that corroborate the association of metformin with higher lactate levels. A Chinese study describes the result of a cross sectional measurement of lactate in 1024 diabetics in an outpatient clinic that had normal renal function and no increased risk of elevated lactate (i.e., excluded patients with chronic liver disease and cardiac insufficiency). They showed that patients medicated with metformin had a slightly but significant higher level of lactate than patients who were not on this medication31. Another retrospective French study compared patients admitted to an intensive care unit for MALA who had an intentional versus accidental intoxication with metformin.
They showed that metformin can, in fact, lead to lactic acidosis, although mortality was primarily associated with underlying health status and organ dysfunction32.
In conclusion, causality between metformin and lactic acidosis cannot be ruled out, although its real impact in the prognosis and morbidity/mortality of diabetic patients is difficult to account for. The challenge is to differentiate who would benefit from being denied the first line medication for diabetes.
The European, American, Canadian and many other national guidelines agree to contraindicate metformin in patients with CKD class 4 or higher and most suggest a cautious use in CKD class 316, 18,33. While there are no randomized controlled trials (RCTs) that evaluate the safety and potential benefit of this medication, all patients should be educated to contact a health care provider and hold metformin (as well as angiotensin-converting enzyme inhibitor, angiotensin II receptor blockers, diuretics, and non-steroidal anti-inflammatory drugs), if diarrhoea or vomiting together with inability to tolerate oral liquids intake develops24.
SULFONYLUREAS
Sulfonylureas reduce blood glucose by stimulating the pancreatic beta cells to increase insulin secretion34.
Therefore, their effectiveness tends to decline over time, as there is a reduction in the number of viable pancreatic beta cells35. The major risk associated with its use is hypoglycaemia19.
The first -generation sulfonylureas (acetohexamide, chlorpropamide, tolazamide and tolbutamide), the oldest oral hypoglycaemic agents, are almost exclusively excreted by the kidney and are, therefore, contraindicated in CKD due to the risk of hypoglycaemia16.
Second-generation agents (gliclazide, glimepiride, glipizide and glibenclamide) are metabolized in the liver, but some of the drugs (glimepiride and glibenclamide) excrete their active metabolites in the urine and, therefore, should be avoided in renal failure.
Glipizide and gliclazide are the preferred agents and do not need dose adjustment16,19. They are primarily metabolized in the liver and although more than 60% of their metabolites are excreted in the urine, these have no hypoglycaemic activity19.
MEGLITINIDES
Meglitinides are insulin secretagogues that stimulate pancreatic beta cells. Compared with sulfonylureas they are shorter-acting, have modest glycaemic efficacy and a relatively low risk of hypoglycaemia18.
There are three meglitidines (nateglinide, repaglinide, and mitiglinide) currently in clinical use but only nateglinide is available in Portugal19. Although hypoglycaemia has not been demonstrated to increase substantially with progressive falls in GFR, renal dose adjustment is recommended as drug accumulation (repaglinide) or of their active metabolites (nateglinide and mitiglinide) can occur in renal failure36-38. Accumulation of active metabolites is particularly notorious with nateglinide, that should therefore be avoided in ESRD19.
ALPHA- GLUCOSIDASE INHIBITORS
The antihyperglycaemic action of alpha-glucosidase inhibitors (acarbose, miglitol and voglibose) results from the reversible inhibition of membrane-bound intestinal alpha-glucoside hydrolase enzymes. Alpha-glucosidase inhibitors decrease the rate of breakdown of complex carbohydrates so that less glucose is absorbed and postprandial hyperglycaemia is lowered19.
Acarbose is metabolized exclusively within the gastrointestinal tract and approximately a third of these metabolites are absorbed and subsequently excreted in the urine, one of them with alpha-glucosidase inhibitory activity. Although normally less than 2% of the total administered dose is excreted in the urine as active drug, patients with severe renal impairment (creatinine clearance < 25 mL/min) can attain peak plasma concentration of acarbose about 5 -fold higher39.
Miglitol is absorbed without metabolization and is eliminated by renal excretion as unchanged drug40.
As these drugs act locally, dose adjustment to correct for the increased plasma concentrations is not feasible19. Although important adverse side effects have not been described, data are scarce and its generalized use in advanced renal failure is not recommended16,41.
THIAZOLIDINEDIONE
Thiazolidinediones (TZDs) are peroxisome proliferator–activated receptor gamma (PPAR γ) agonists that improve insulin sensitivity in skeletal muscle and reduce hepatic glucose production42. They do not increase the risk of hypoglycaemia and may be more durable in their effectiveness than sulfonylureas and metformin18.
There are currently two available agents from this class: pioglitazone and rosiglitazone. Pioglitazone, which seems to also act like a partial PPARα agonist, appears to decrease triglycerides, increase HDL cholesterol and have a modest benefit on cardiovascular events42,43. Rosiglitazone, an apparently pure PPARγ agonist, is no longer widely available owing to concerns of increased myocardial infarction risk44,45.
Drugs in this class do not need renal dose adjustment because they have predominant hepatic metabolism and their pharmacokinetic profile is independent of renal function46,47. However, because their side effect profile includes weight gain, fluid retention that may lead to oedema and/or heart failure, and increased risk of bone fractures, they should be used with caution in the chronic kidney disease population3,16,18. Moreover, pioglitazone has been associated with a possible increased risk of bladder cancer48.
DPP- 4 INHIBITORS
The oral dipeptidyl peptidase 4 (DPP-4) inhibitors decrease the breakdown of the incretin hormones, such as glucagon-like peptide 1 (GLP -1).
GLP -1 is an intestinal hormone with a meal-induced secretion that stimulates insulin secretion and suppresses glucagon release in a glucose–dependent manner49.
They are generally well tolerated, weight neutral and do not cause hypoglycaemia3,18. All can be used in CKD patients, but sitagliptin, saxagliptin, and vildagliptin need dose adjustments, as opposed to linagliptin that can be used in the normal doses16.
INCRETIN MIMETICS
Incretin mimetics (exenatide and liraglutide) are subcutaneously injectable GLP-1 receptor agonists that thereby stimulate pancreatic insulin secretion and suppress pancreatic glucagon output in a glucose dependent manner, slow gastric emptying, and decrease appetite19. Their main advantage is weight loss18. Exetanide has a renal excretion and should be avoided in patients with eGFR < 30ml/min/1.73m2 16. Liraglutide is not significantly eliminated by the kidneys and pharmacokinetic studies suggest blood levels are not affected by renal failure50. However, there is still insufficient safety data to recommend its use in CKD patients16.
SODIUM- GLUCOSE CO- TRANSPORTER 2 (SGLT2) INHIBITORS
SGLT 2 inhibitors are the most recent class of drugs approved by the United States Food and Drug Administration (FDA) for the treatment of diabetes, still not available in Portugal. They are currently represented by canagliflozin and improve glycaemic control in an insulin-independent fashion through inhibition of glucose reuptake in the kidney51.
Phase III clinical trials have shown improved glycaemic control in type 2 diabetes associated with a relatively low hypoglycaemia risk and weight loss-promoting effect. The major side effects appear to be urinary and mycotic genital infections and adverse effects related to osmotic diuresis and reduced intravascular volume51,52.A phase III RCT with canagliflozin against placebo was performed in 272 CKD 3 patients, concluding that this new agent was generally well tolerated and might be a possible therapeutic option for this subpopulation.
However, they did report a higher decrease in eGFR at 26 weeks in the canagliflozin arm compared to placebo, for which statistical significance was not performed. While data are still scarce, caution should be taken before using them in CKD patients53.
OTHER NON- INSULIN HYPOGLYCAEMIC DRUGS
There are many other agents that are being investigated as potential therapeutic weapons in diabetes.
Bile acid sequestrants (i.e., colesevelam)54, dopamine-2 agonists (i.e., bromocriptine)55 and amylin mimetics (i.e., pramlintide)56 are some of the most promising drugs that are now defining their potential role in the treatment of diabetes.
INSULIN
Exogenous insulin is the most potent antihyperglycaemic agent, with a theoretically universal and unlimited effectiveness. However, because it is an injectable drug associated with hypoglycemia risk and weight gain, it is most commonly considered a second or third line therapy18.
Due to the progressive Beta-cell dysfunction that characterizes type 2 diabetes, insulin replacement therapy is frequently required, alone or in combination with other agents18. This is particularly true in the renal failure population, where the therapeutic options are more limited.
There are a variety of insulin preparations, which specific indications and pharmacokinetics go beyond the scope of this review. None of them is contraindicated in CKD patients and dose should be adjusted based on patient response16. Due to the fact that the kidneys metabolize 25% of circulating insulin, progressive declines in eGFR are expected to increase the exogenous (and residual endogenous) blood levels and thus decrease the requirement dose of exogenous insulin41.
SUGGESTED SCHEDULES IN THE RENAL FAILURE PATIENT
Guidelines for the treatment of diabetes are becoming less strict and, as previously stated, should be based upon clinical, social and economical criteria18.
Having this in mind, and according to the review above, we recommend the use of the following drugs in chronic kidney disease patients in monotherapy or, if necessary, in 2 or 3 drug -combinations:
CKD 3: Metformin + second generation sulphonylureas (gliclazide or glipizide)/meglitidines (any) + DPP4 inhibitors (any)/Incretin mimetics (exenatide) + Thiazolidinediones (pioglitazone) + alpha -Glucosidase inhibitors (any) + insulin.
CKD 4-5d: Second generation sulphonylureas (gliclazide or glipizide)/Meglitidines (repaglidine or mitiglinide) + DPP4 inhibitors (any) + Thiazolidinediones (pioglitazone) + insulin.
The order does not mean to indicate any specific preference. However, clinicians should not forget the advantages and possible side effects of each class of drugs when prescribing. Namely, thiazolidinediones can cause fluid retention, heart failure and bone fractures and, therefore, may be contraindicated in the subgroup of renal failure patients with cardiovascular and/or mineral bone disease. Additionally, renal patients that have previously been exposed to cyclophosphamide would have a cumulative risk of bladder cancer if given rosiglitazone. Metformin should be used cautiously, as explained in the former section. When prescribing drug combinations, agents with the same mechanism of action should not be favoured (these agents are separated above by a slash).
CONCLUSION
Diabetic patients with chronic kidney disease are a particular challenging population to treat. While glycaemic targets are still not well validated, HbA1c and daily finger-stick blood glucose measurements seem to be the most reasonable measure of glycaemic control. Metformin, the fist -line therapeutic agent in the general population, should be used with caution in CKD class 3 and is contraindicated when eGFR < 30ml/min/1.73m2. Alternatives to be used alone or in combination, without dose adjustment, include some second generation sulphonylureas, thiazolidinediones and insulin. Nevertheless, thiazolidinediones may cause oedema and heart failure and should be used with caution in this population. Meglitinides, DPP-4 inhibitors and some incretin mimetics can also be used with dose adjustment.
In conclusion, although there are still many open questions about the ideal treatment of diabetic CKD patients, there are now many available therapeutic options, that if used with knowledge, can improve the quality and quantity of life of these patients.
References
1. Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract 2010;87(1):4-14 [ Links ]
2. Gardete-Correia L, Boavida JM, Raposo JF, et al. First diabetes prevalence study in Portugal: PREVADIAB study. Diabet Med 2010;27(8):879-881 [ Links ]
3. American Diabetes Association. Standards of medical care in diabetes. Diabetes Care 2012;35(Suppl 1):S11 -S63 [ Links ]
4. Reutens AT, Atkins RC. Epidemiology of diabetic nephropathy. Contrib Nephrol 2011;170:1-7 [ Links ]
5. The DCCT Research Group. The effect of intensive treatment of diabetes on the development and progression of long -term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993;329:977-986 [ Links ]
6. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood -glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998;352:837-853 [ Links ]
7. UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet 1998;352:854 -865 [ Links ]
8. Patel A, MacMahon S, Chalmers J, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med 2008;358:2560-2572 [ Links ]
9. Ismail -Beigi F, Craven T, Banerji MA, et al. Effect of intensive treatment of hyperglycaemia on microvascular outcomes in type 2 diabetes: an analysis of the ACCORD randomised trial. Lancet 2010;376:419-430 [ Links ]
10. Duckworth W, Abraira C, Moritz T, et al. Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med 2009;360(2):129-139 [ Links ]
11. Kalantar-Zadeh K, Kopple JD, Regidor DL, et al. A1C and survival in maintenance hemodialysis patients. Diabetes Care 2007;30(5):1049-1055 [ Links ]
12. Morioka T, Emoto M, Tabata T, et al. Glycemic control is a predictor of survival for diabetic patients on hemodialysis. Diabetes Care 2001;24(5):909-913 [ Links ]
13. Kovesdy CP, Sharma K, Kalantar -Zadeh K. Glycemic control in diabetic CKD patients: where do we stand? Am J Kidney Dis 2008;52(4):766-777 [ Links ]
14. Freedman BI, Shihabi ZK, Andries L, et al. Relationship between assays of glycemia in diabetic subjects with advanced chronic kidney disease. Am J Nephrol 2010;31(5):375-379 [ Links ]
15. Inaba M, Okuno S, Kumeda Y, et al. Glycated albumin is a better glycemic indicator than glycated hemoglobin values in hemodialysis patients with diabetes: effect of anemia and erythropoietin injection. J Am Soc Nephrol 2007;18(3):896-903 [ Links ]
16. National Kidney Foundation. KDOQI Clinical Practice Guideline for Diabetes and CKD: 2012 update. Am J Kidney Dis 2012;60(5):850-886 [ Links ]
17. Ix JH. Hemoglobin A1c in Hemodialysis patients: should one size fit all? Clin J Am Soc Nephrol 2010;5(9):1539-1541 [ Links ]
18. Inzucchi SE, Bergenstal RM, Buse JB, Diamant M, Ferrannini E. Management of hyperglycemia in type2 diabetes: a patient -centered approach: position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2012;35:1364-1379 [ Links ]
19. Abe M, Okada K, Soma M. Antidiabetic agents in patients with chronic kidney disease and end-stage renal disease on dialysis: metabolism and clinical practice. Curr Drug Metab 2011;12(1):57-69. [ Links ]
20. Bailey CJ, Turner RC. Metformin. N Engl J Med 1996(9);334:574-579 [ Links ]
21. Tahrani AA, Varughese GI, Scarpello JH, Hanna FW. Metformin, heart failure, and lactic acidosis: is metformin absolutely contraindicated? BMJ 2007;335:508-512 [ Links ]
22. Misbin RI, Green L, Stadel BV, Gueriguian JL, Gubbi A, Fleming GA. Lactic acidosis in patients with diabetes treated with metformin. N Engl J Med 1998;338(4):265-266 [ Links ]
23. Owen MR, Doran E, Halestrap AP. Evidence that metformin exerts its anti-diabetic effects through inhibition of complex 1 of the mitochondrial respiratory chain. Biochem J 2000;348:607-614 [ Links ]
24. Prikis M, Mesler EL, Hood VL, Weise WJ. When a friend can become an enemy! Recognition and management of metformin -associated lactic acidosis. Kidney Int 2007;72(9):1157-1160 [ Links ]
25. Gómez -Navarro L, de Arriba G, Sánchez -Heras M, et al. The nephrologists role in metformin-induced lactic acidosis. Nefrologia 2011;31(5):587-590 [ Links ]
26. Peters N, Jay N, Barraud D, et al. Metformin -associated lactic acidosis in an intensive care unit. Crit Care 2008;12(6):R149 (doi:10.1186/cc7137) [ Links ]
27. Stades AM, Heikens JT, Erkelens DW, Holleman F, Hoekstra JB. Metformin and lactic acidosis: cause or coincidence? A review of case reports. J Intern Med 2004;255(2):179-187 [ Links ]
28. McCormack J, Johns K, Tildesley H. Metformins contraindications should be contraindicated. CMAJ 2005;173(5):502-504 [ Links ]
29. Holstein A, Stumvoll M. Contraindications can damage your health–is metformin a case in point? Diabetologia 2005;48(12):2454-2459. [ Links ]
30. Salpeter SR, Greyber E, Pasternak GA, Salpeter EE. Risk of fatal and nonfatal lactic acidosis with metformin use in type 2 diabetes mellitus (Review). Cochrane Database Syst Rev 2010 Apr 14;(4):CD002967. doi: 10.1002/14651858.CD002967.pub4. [ Links ]
31. Liu F, Lu JX, Tang JL, et al. Relationship of plasma creatinine and lactic acid in type 2 diabetic patients without renal dysfunction. Chin Med J 2009;122(21):2547-2553 [ Links ]
32. Seidowsky A, Nseir S, Houdret N, Fourrier F. Metformin -associated lactic acidosis: A prognostic and therapeutic study. Crit Care Med 2009;37(7):2191-2196 [ Links ]
33. Canadian Diabetes Association 2008 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diabetes 2008;32(suppl 1) [ Links ]
34. Bryan J, Crane A, Vila -Carriles WH, Babenko AP, Aguilar -Bryan L. Insulin secretagogues, sulfonylurea receptors and K(ATP) channels. Curr Pharm Des 2005;11(21):2699-2716 [ Links ]
35. Holman RR. Long-term efficacy of sulfonylureas: a United Kingdom Prospective Diabetes Study perspective. Metabolism 2006;55:S2–S5 [ Links ]
36. Nagai T, Imamura M, Iizuka K, Mori M. Hypoglycemia due to nateglinide administration in diabetic patient with chronic renal failure. Diabetes Res Clin Pract 2003;59(3):191-194 [ Links ]
37. Inoue T, Shibahara N, Miyagawa K, et al. Pharmacokinetics of nateglinide and its metabolites in subjects with type 2 diabetes mellitus and renal failure. Clin Nephrol 2003;60(2):90-95 [ Links ]
38. Schumacher S, Abbasi I, Weise D, et al. Single - and multiple -dose pharmacokinetics of repaglinide in patients with type 2 diabetes and renal impairment. Eur J Clin Pharmacol 2001;57(2):147-152 [ Links ]
39. PRECOSE (acarbose tablets) [Internet] 2008 [updated 2011; cited 2013 May 8]. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/020482s025lbl.pdf [ Links ]
40. Glyset (miglitol) tablets. [Internet] 2012 [updated 2012 Sep; cited 2013 May 8]. Available from: http://www.pfizer.com/files/products/uspi_glyset.pdf [ Links ]
41. Shrishrimal K, Hart P, Michota F. Managing diabetes in hemodialysis patients: Observations and recommendations. Cleve Clin J Med 2009;76(11):649-655 [ Links ]
42. Yki -Järvinen H. Thiazolidinediones. N Engl J Med 2004;351(11):1106-1118 [ Links ]
43. Dormandy JA, Charbonnel B, Eckland DJ, et al. Secondary prevention of macrovascular events in patients with type 2 diabetes in the PROactive Study (Prospective pioglitazone Clinical Trial In macroVascular Events): a randomized controlled trial. Lancet 2005;366:1279-1289 [ Links ]
44. Nissen SE, Wolski K. Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N Engl J Med 2007;356(24):2457-2471 [ Links ]
45. Nissen SE, Wolski K. Rosiglitazone revisited: an updated meta -analysis of risk for myocardial infarction and cardiovascular mortality. Arch Intern Med 2010;170(14):1191-1201 [ Links ]
46. Budde K, Neumayer HH, Fritsche L, Sulowicz W, Stompôr T, Eckland D. The pharmacokinetics of pioglitazone in patients with impaired renal function. Br J Clin Pharmacol 2003;55(4):368-374 [ Links ]
47. Thompson-Culkin K, Zussman B, Miller AK, Freed MI. Pharmakokinetics of rosiglitazone in patients with end stage renal disease. J Int Med Res 2002;30(4):391-399 [ Links ]
48. Lewis JD, Ferrara A, Peng T, et al. Risk of bladder cancer among diabetic patients treated with pioglitazone: interim report of a longitudinal cohort study. Diabetes Care 2011;34(4):916-922 [ Links ]
49. Drucker DJ, Nauck MA. The incretin system: glucagon -like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes. Lancet 2006;368:1696-1705 [ Links ]
50. Jacobsen LV, Hindsberger C, Robson R, Zdravkovic M. Effect of renal impairment on the pharmacokinetics of the GLP-1 analogue liraglutide. Br J Clin Pharmacol 2009; 68(6):898-905 [ Links ]
51. Nisly SA, Kolanczyk DM, Walton AM. Canagliflozin, a new sodium -glucose cotransporter 2 inhibitor, in the treatment of diabetes. Am J Health Syst Pharm 2013;70(4):311-319 [ Links ]
52. Schernthaner G, Gross JL, Rosenstock J, et al. Canagliflozin compared with sitagliptin for patients with type 2 diabetes who do not have adequate glycemic control with metformin plus sulfonylurea: A 52 -week randomized trial. Diabetes Care 2013;Apr 5. [Epub ahead of print] [ Links ]
53. Yale JF, Bakris G, Cariou B, et al. Efficacy and safety of canagliflozin in subjects with type 2 diabetes and chronic kidney disease. Diabetes Obes Metab 2013;15(5):463-473 [ Links ]
54. Fonseca VA, Handelsman Y, Staels B. Colesevelam lowers glucose and lipid levels in type 2 diabetes: the clinical evidence. Diabetes Obes Metab 2010;12(5):384-392 [ Links ]
55. DeFronzo RA. Bromocriptine: a sympatholytic, D2 -dopamine agonist for the treatment of type 2 diabetes. Diabetes Care 2011;34(4):789-794 [ Links ]
56. Singh-Franco D, Robles G, Gazze D. Pramlintide acetate injection for the treatment of type 1 and type 2 diabetes mellitus. Clin Ther 2007;29(4):535-562 [ Links ]
Sílvia Coelho
Department of Nephrology
Fernando da Fonseca Hospital EPE, IC 19
2720-376 Amadora
Portugal
E-mail: silvia.coelho.nephro@gmail.com
Conflict of interest statement. None declared
Received for publication: 13/03/2013
Accepted in revised form: 08/05/2013


{kind=link}