










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.27 no.3 Lisboa set. 2013
Pancreas-Kidney Transplantation: Analysis of 150 patients from one Centre in Portugal
Transplantação Reno-Pancreática: Análise de 150 doentes de um Centro em Portugal
La Salete Martins1,2, Isabel Fonseca1, Pedro Aguiar1, Ana Rocha1, Rui Costa1, Clara Santos1, Jorge Malheiro1, Sofia Pedroso1,2, Manuela Almeida1,2, Leonidio Dias1,2, Antonio C Henriques1,2, Antonio Cabrita1,2, Jose Davide2
1 Departments of Nephrology and 2 Transplantation
Hospital Santo António, CHP – Porto – Portugal
ABSTRACT
Introduction: Simultaneous pancreas-kidney transplantation (SPKT) outcomes are conditioned in the short-term mostly by post-operative complications. In the long-term, cardiovascular (CV) disease and immunological loss are the main limitations to transplant survival. Aims: To analyse retrospectively the results from 150 SPKT performed at our centre. Patients and Methods: The 81 females and 69 males had a mean age of 35 ±6 years; they were diabetic for 24 ±6 years and had been on dialysis for 30±21months (except 5 preemptive). Anti-lymphocyte globulin, tacrolimus, mycophenolate and steroids were used as immunosuppressive therapy. Deceased-donor mean age was 28 ±11 years. In 28.7% the transplant was performed with 6 HLA-mismatches. Results: Acute rejections incidence was 16%. Ten SPKT patients died; infection was the leading cause of death (five cases), followed by Cardiovascular/cerebrovascular disease (three cases). In 21 patients the pancreas failed, mainly due to thrombosis or bleeding (11 cases), and infection (five cases); in two it was due to late acute rejection. In four patients only the kidney failed, due to chronic rejection. Five patients lost both grafts, from late acute rejection in four and thrombosis in one. We analyzed the 110 SPKT patients (73.3%) with both grafts functioning. Their mean serum creatinine was 1.2 ±0.4mg/dl; creatinineclearance was 76±24 ml/min; fasting glycaemia was 81 ±10mg/dl; and HbA1c was 5.3±0.4%. Hypertension has been treated in 47.2% of patients, in the majority (28.2%) with only one drug. Hyperlipidaemia was observed in 19.1% and excessive weight (>25kg/m2) in 17.3%. Conclusions: From our cohort of SPKT, 93.3% of patients are alive, 73.3% have both grafts functioning. Rejection was the main cause of late pancreas loss. Early mortality was due to infection (3.3%). CV/cerebrovascular disease was the main cause of late mortality (2%). The prevalence of hyperlipidaemia and overweight was inferior to 20%. Hypertension was the most frequently found CV risk factor.
Key-words: graft loss; long-term results; pancreas-kidney transplantation; patient death
RESUMO
Introdução: A sobrevivência do transplante de rim-pâncreas (TRP) e condicionada na fase precoce pelas complicações inerentes ao próprio acto cirúrgico. A sua perda tardia deve-se essencialmente a morte por doença cardiovascular (CV), ou imunológica. Objectivos: Analisamos retrospectivamente os resultados dos 150 TRP realizados no nosso centro. Doentes e métodos: Os 81 doentes do sexo F e 69 do sexo M, tinham uma idade media de 35 ±6 anos; eram diabéticos ha 24±6 anos; e estavam em dialise ha 30 ±21meses (excepto 5 preemptive). A terapêutica imunossupressora consistiu em globulina antilinfocitica, tacrolimus, micofenolato e corticoides. A media de idades do dador (cadáver) foi 28 ±11 anos. Em 28.7% o transplante foi realizado com 6 incompatibilidades HLA. Resultados: A incidência de rejeição aguda foi de 16%. Faleceram 10 doentes: a causa mais frequente foi a infecciosa (5 casos), seguida da CV/cerebrovascular (3 casos). Em 21 casos houve falência isolada do pâncreas maioritariamente por trombose ou hemorragia (11 casos) e por infecção (5 casos), em 2 casos por rejeição aguda tardia. Em 4 TRP ocorreu falência isolada do rim, por rejeição cronica. Em 5 casos ambos os enxertos faliram: por rejeição aguda tardia 4 doentes; trombose 1 doente. Os 110 TRP (73.3%) que mantem ambos os enxertos funcionantes, tem creatinina de 1.2±0.4mg/dl; clearance da creatinina de 76±24 ml/min; glicemia em jejum de 81±10mg/dl; e HbA1c de 5.3 ±0.4%. Apresentam hipertensão 47,2%, a maioria (28,2%) requerendo apenas 1 fármaco. Hiperlipidemia verificou-se em 19,1% e excesso de peso (>25kg/m2) em 17,3% dos doentes. Conclusões: Deste grupo de TRP estudado, estão vivos 93.3% e 73.3% tem ambos os enxertos funcionantes. Rejeição foi a principal causa de perda tardia do pâncreas. A mortalidade precoce deveu-se a infeção (3.3%). Doença CV/cerebrovascular foi a causa mais frequente de mortalidade tardia (2%). A prevalência de hiperlipidemia e excesso de peso foi inferior a 20%. Hipertensão foi o factor de risco CV mais frequentemente encontrado.
Palavras-chave: morte do doente; perda de enxerto; resultados a longo-prazo; transplantação reno-pancreática
INTRODUCTION
Simultaneous pancreas-kidney transplantation (SPKT) is the best treatment for type 1 diabetic patients with end-stage renal disease who have the conditions for this kind of transplant. The results of SPKT are better than those obtained from other modalities of pancreas transplantation, such as pancreas after kidney (PAK), or pancreas transplantation alone (PTA)1. A successful SPKT frees the patient from insulin and dialysis-dependence and avoids the life-threatening hypoglycaemic episodes. This may represent a significant improvement on their impaired quality of life. It is unquestionable that SPKT leads to a significant improvement in patient survival, when compared to those staying under dialysis and insulin, or even compared to those who underwent a cadaveric kidney alone transplant2.
Moreover, the pancreas transplant may stop the progression or even ameliorate the various secondary diabetic complications1,2.
Outcomes of SKPT have improved over time, in parallel with other organ transplants1,2,3. However, patient and graft loss after SPKT, namely in the early phase after surgery, is higher than in kidney transplantation alone. Thrombotic and infectious complications are the leading causes of graft failure or even patient death in the short-term1. Cardiovascular or cerebrovascular disease2,3 and also infection1,2 are the main limitations for long-term SPKT patient survival.
Immunological loss3 and death with a functioning graft3 represent the main causes of graft failure in the long-term. It is well known for these patients the increase in mortality after graft loss: the relative risk of death increased more than 17-fold in recipients whose kidney failed and more than 3-fold in recipients whose pancreas failed1.
The aim of this study was to analyze the outcome of the SPKT performed at our centre and to search for possible factors associated with the outcome.
PATIENTS AND METHODS
From May 2000 to October 2012, 150 type 1 diabetic patients underwent SKPT at the Transplantation Department of our Hospital. All the procedures were performed using grafts form deceased donors, both grafts from the same donor, and using systemicenteric drainage (venous drainage to the iliac vein; exocrine drainage through an enteric anastomosis of the pancreatic-duodenal arch). Only patients with a minimum follow-up of 3 months were considered for this retrospective analysis.
Results are presented as mean ± standard deviation for continuous, normally distributed variables, and as percentages for categorical data. Patient survival was determined from the time of SPKT until death or end of follow-up. Death-censored kidney graft survival was determined from the time of kidney transplantation until kidney retransplantation, return to dialysis, or end of follow-up. Death-censored pancreas graft survival was determined from the time of SPKT until pancreas failure or end of follow-up.
Survival analysis was performed using the Kaplan-Meier (product-limit) estimator of survival.
These 150 patients, 81 females and 69 males, had a mean age of 35±6 years at transplantation date.
They were diabetic for 24±6 years; and had been on dialysis for 30±21months, excepting five patients who received a pre-emptive transplant. Anti-lymphocyte globulin, tacrolimus, mycophenolate and steroids were used as induction therapy. Deceased-donor mean age was 28±11 years. In 28.7% of the patients the transplant was performed with 6 HLA-mismatches.
RESULTS
The median admission time was 20 days. Global acute rejection incidence (for kidney, pancreas or both grafts) was 16%. Delayed kidney graft function, defined for dialysis need in the first week, occurred in 16%.
In the vast majority of patients whose pancreas did not have complications, insulin administration could be stopped during the first hours after transplantation (median 0 days).
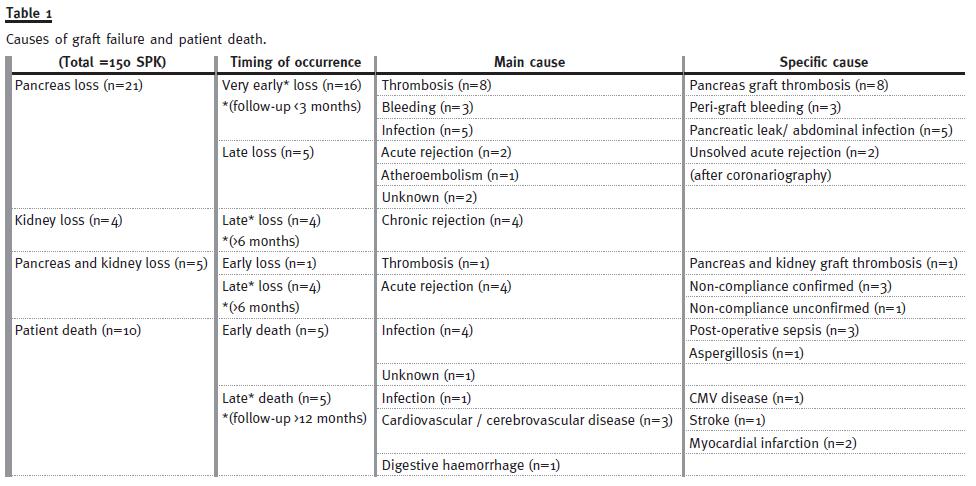
In 21 patients the pancreas failed, mainly (16 cases) in the very early period (<3 months) due to thrombosis (eight cases) or bleeding (three cases) and local infection leading to graft removal (five cases); late pancreas loss was due to late acute rejection (two cases), atheroembolism after coronary angiography using lower limb access (one case) and due to unknown cause in two cases.
In four patients only the kidney failed, due to chronic rejection, and these were late losses. In five others, both grafts failed: in one case it was an early loss due to thrombosis of both grafts; and in four it was due to late (> 6 months) acute rejection – in three cases we have confirmed patient non-compliance to medication. Tacrolimus trough levels were undetectable or markedly below the expected for this follow-up time (7-9 ng/ml).
Death occurred in 10 patients: in five during the early period, and later in five others. Analyzing the causes of patient death from the point of view of the different periods (< 12months vs. > 12 months): early deaths were due to post-operative sepsis (three cases), aspergillosis (one case), and unclear cause (one case); late deaths were caused by myocardial infarction (two cases), stroke (one case), CMV disease (one case) and digestive haemorrhage (one case).
Globally, infection was the leading cause of death (five cases), followed by cardiovascular (CV) or cerebrovascular disease (three cases). Table 1 summarizes the causes of graft failure and patient death.
At the last visit, 110 SPKT patients (73.3%) maintained both grafts functioning. Their mean serum creatinine is 1.2±0.4mg/dl; creatinine clearance is 76±24 ml/min; fasting glycaemia is 81±10mg/dl; and HbA1c=5.3±0.4%. Hypertension has been treated in 52 SPKT (47.2%), in the majority (31SPKT – 28.2%) with a single drug, mostly a beta-blocking agent. Hyperlipidaemia was observed in 23 patients (20.9%) and excessive weight (> 25kg/m2) in 19 patients (17.3%).
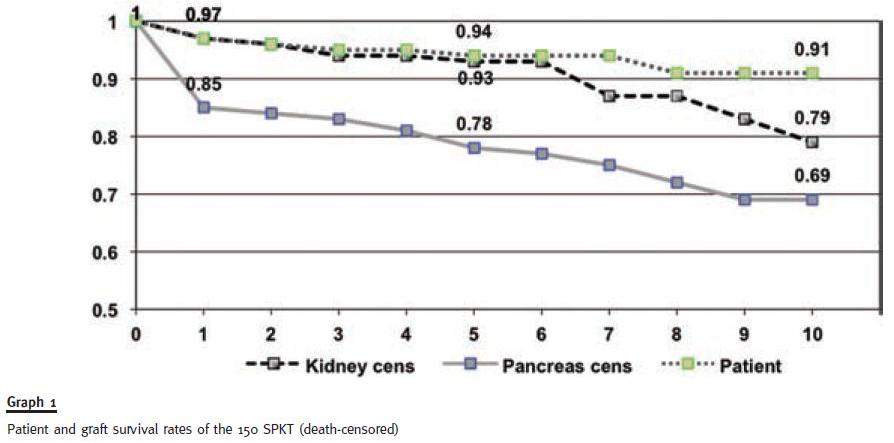
Survival rates (death-censored) obtained for this cohort of SPKT at our centre for patient, kidney and pancreas, respectively, were: at 1 year 97%, 97% and 85%; at 5 years 94%, 93% and 78%; and at 10 years 91%, 79% and 69% (Graph 1).
DISCUSSION
There are no longer any doubts that SPKT offers the best results to treat type 1 diabetic patients with end-stage renal disease. The last position statement of the American Diabetes Association4 has confirmed, again, their previous recommendation5 of pancreas transplantation for these patients, preferably done simultaneously to a kidney transplant, given the better pancreas survival of SPKT4,5. Also from a point of view of quality of life, SPKT can provide significant benefit6,7. The successive International Pancreas Transplant Registry (IPTR) reports have confirmed the progressive improvement in SPKT outcome over the past decades1,8,9. However, it seems that a maximum and a plateau was reached in the survival curves, because no further significant improvements have been observed in the last 10 years1.
Pancreas graft outcome is determined mostly by the success in early post-operative period. Thrombosis, bleeding, pancreatic leaks and infection after surgery are normally defined as technical failures. In the last IPTR1, near 9% of the losses were reported as due to technical failure. It is 10.7% in our own experience (16/150 patients), not too different from the international results recorded on 25000 SPKT1.
Thrombosis remained the main cause of early pancreas graft loss, as reported by large centers2,3.
Pancreas losses due to acute rejection were observed in our study group in 6 SPKT (4%), but in half of them non-compliance of the patients to immunosuppression was verified. Blindness or very impaired vision may be a real problem for these patients to strictly follow the medication and this was the case in at least one patient. Thus, if we exclude the expected losses associated with confirmed/confessed non-compliance, we obtain a rate of 2% of unexpected acute rejection loss, similar to that observed in large series1,8.
Kidney graft loss occurred in the late period in all but one of the 9 patients of our study group with kidney failure. Rejection was the main cause of these late losses and this has also been observed by others2,3.
Systemic vascular disease, CV and cerebrovascular disease are strongly associated with an increased risk of patient death2. In our own experience, infection in the early period (3.3%) and CV/cerebrovascular disease (2%) in the late period were the leading causes of patient death. These same reasons for patient death were reported by the IPTR1; and the authors observed that death due to infection peaked between 3 and 12 months.
Hypertension was the most frequently found CV risk factor, although its prevalence was inferior to 50% and in only 28.2% requiring more than one drug. Beta-blocking agents were the most often prescribed drugs with anti-hypertensive properties, even when the goal is not necessarily to treat hypertension.
In fact, in some of these patients high blood pressure was not recorded. However, it is our policy to maintain this medication, given its cardio-protective effects, especially if the patients had previously been under this drug. The prevalence of hyperlipidaemia and excessive weight was inferior to 20% in our SPKT patients.
Compared to kidney transplantation alone, SPKT is known to have more complications: a higher rate of readmissions10 and early surgical complications that may lead to relaparotomy in more than 30% of cases3,11. Despite these feared complications and the initial increased risk (compared with those patients in the waiting list for transplant), transplanted patients perform better at 1 year12. Moreover, and against initial concerns, 10-year results do not confirm a higher mortality of diabetics after SPKT versus kidney transplantation alone13. The improvement in quality of life and the effect on long-term diabetic complications justify the option for surgery12.
The developed LYFT scores (life years from transplant), which assess life enhancement achieved by each transplant, was greater for diabetics with a SPKT than with kidney transplantation alone14. Thus, it is currently stated that SPKT is the most costeffective treatment for patients with type 1 diabetes and end-stage renal disease15.
The authors of the latest IPTR reported a 10-year patient survival over 70%16. Considering only SPKT recipients who reached the 1-year mark with both grafts alive, they reported a 10-year survival rate around 66 % for the kidney and 62% for the pancreas grafts. In a more recent analysis, the 10-year pancreas graft function for SPKT was 68%16. We have published the 10-year results of SPKT at our centre two years ago17 and they were not inferior to the international results. Those good outcomes and survival rates are validated by remain confirmed in this cohort of patients with extended follow-up.
References
1. Gruessner AC. 2011 Update on pancreas transplantation: comprehensive trend analysis of 25,000 cases followed up over the course of twenty-four years at the International Pancreas Transplant Registry (IPTR). Rev Diabet Stud 2011;8(1):6-16. [ Links ]
2. Sutherland DE, Gruessner RW, Dunn DL, et al. Lessons learned from more than 1,000 pancreas transplants at a single institution. Ann Surg 2001;233(4):463-501. [ Links ]
3. Sollinger HW, Odorico JS, Becker YT, DAlessandro AM, Pirsch JD. One thousand simultaneous pancreas-kidney transplants at a single center with 22-year follow-up. Ann Surg. 2009;250(4):618-630 [ Links ]
4. Robertson RP, Davis C, Larsen J, Stratta R, Sutherland DE; American Diabetes Association. Pancreas and islet transplantation in type 1 diabetes. Diabetes Care. 2006;29(4):935. [ Links ]
5. Robertson P, Davis C, Larsen J, Stratta R, Sutherland DE; American Diabetes Association. Pancreas transplantation in type 1 diabetes. Position statement. Diabetes Care 2004; 27(Suppl 1): S105. [ Links ]
6. Robertson RP, Davis C, Larsen J, Stratta R, Sutherland DE. Pancreas and islet transplantation for patients with diabetes. Diabetes Care. 2000;23(1):112-116. [ Links ]
7. Scalea JR, Cooper M. Current concepts in the simultaneous transplantation of kidney and pancreas. J Intensive Care Med 2012;27(4):199-206. [ Links ]
8. Gruessner AC, Sutherland DE. Pancreas transplant outcomes for United States (US) cases as reported to the United Network for Organ Sharing (UNOS) and the International Pancreas Transplant Registry (IPTR). Clin Transplant 2008;45-56. [ Links ]
9. Gruessner A C, Sutherland DE. Pancreas transplant outcomes for United States (US) and non-US cases as reported to the United Network for Organ Sharing (UNOS) and the International Pancreas Transplant Registry (IPTR) as of June 2004. Clin Transplant 2005;19(4):433-455. [ Links ]
10. Martins L, Henriques AC, Dias L, et al. Pancreas-kidney transplantation: complications and readmissions in 9-years of follow-up. Transplant Proc 2010;42(2):552-554. [ Links ]
11. Gruessner RW, Sutherland DE, Troppmann C, et al. The surgical risk of pancreas transplantation in the cyclosporine era: an overview. J Am Coll Surg. 1997;185(2):128-144. [ Links ]
12. White SA, Shaw JA, Sutherland DE. Pancreas transplantation. Lancet. 2009;373:1808-1817. [ Links ]
13. Tyden G, Bolinder J, Solders G, Brattstrom C, Tibell A, Groth CG. Improved survival in patients with insulin-dependent diabetes mellitus and end-stage diabetic nephropathy 10 years after combined pancreas and kidney transplantation. Transplantation 1999;67(5):645-648. [ Links ]
14. Wolfe RA, McCullough KP, Schaubel DE, et al. Calculating life years from transplant (LYFT): methods for kidney and kidney-pancreas candidates. Am J Transplant 2008; 8(4 Pt2):997-1011. [ Links ]
15. Douzdjian V, Ferrara D, Silvestri G. Treatment strategies for insulin-dependent diabetics with ESRD: a cost-effectiveness decision analysis model. Am J Kidney Dis. 1998;31(5):794-802. [ Links ]
16. Gruessner AC, Sutherland DE, Gruessner RW. Long-term outcome after pancreas transplantation. Curr Opin Organ Transplant. 2012;17(1):100-105. [ Links ]
17. Martins L, Henriques AC, Dias L, et al. One hundred eleven simultaneous pancreaskidney transplantations: 10-year experience from a single center in Portugal. Transplant Proc. 2011;43(1):205-208. [ Links ]
Dra La Salete Martins
Servico de Nefrologia e Transplantacao
Centro Hospitalar do Porto – Hospital de Santo Antonio
Largo Prof. Abel Salazar 4099-001 Porto, Portugal
E-mail: lasalet@gmail.com
Conflict of interest statement: none declared
Received for publication: 05/06/2013
Accepted in revised form: 09/07/2013


{kind=link}
{kind=link}