










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.27 no.4 Lisboa dez. 2013
CASE REPORT
Nephrotic proteinuria in a patient with Rhupus
Proteinúria nefrótica num doente com Rúpus
Ricardo Santos, Rui Silva, Beatriz Malvar, Pedro Pessegueiro, Carlos Pires
Department of Nephrology, Hospital do Espírito Santo de Évora, E.P.E. Évora, Portugal.
ABSTRACT
The kidney is often affected by connective tissue diseases and their treatments. We report the case of a 45-year-old Caucasian female who presented to our nephrology department with nephrotic proteinuria (maximum 6200 mg per day) and a history of rheumatoid arthritis (RA) treated with antimalarial, corticotherapy and non-steroidal anti-inflammatory drugs (NSAIDs). Furthermore, on clinical assessment we identified four criteria for systemic lupus erythematosus (SLE). We promptly withdrew the NSAIDs and, after 3 months without significant reduction in proteinuria, we decided to perform a renal biopsy. The histological examination found a stage 1 membranous nephropathy (suggestive of class V lupus nephritis). After less than six months without NSAIDs, there was spontaneous complete clinical remission of the nephrotic syndrome. In this paper we discuss the aetiology of the glomerular disease in this patient as an adverse effect of NSAIDs treatment versus glomerular disease associated to RA/ SLE (Rhupus).
Key-Words: Lupus Nephritis; Membranous Nephropathy; Nephrotic Syndrome; Non-steroidal Anti-inflammatory Drugs; Rheumatoid Arthritis; Rhupus; Systemic Lupus Erythematosus
RESUMO
O rim é frequentemente atingido por doenças do tecido conjuntivo e pelos seus tratamentos. Apresentamos o caso de uma doente leucodérmica de 45 anos referenciada à consulta de Nefrologia por proteinúria nefrótica (máximo 6200 mg por dia), com história de artrite reumatóide (AR) tratada com anti-malárico, corticoterapia e anti-inflamatórios não esteróides (AINEs). A avaliação clínica permitiu adicionalmente identificar quatro critérios de Lúpus Eritematoso Sistémico (LES). Suspenderam-se os AINEs e após 3 meses sem redução significativa da proteinúria decidiu-se efetuar biópsia renal. O exame histológico revelou nefropatia membranosa estádio 1 (sugestiva de nefrite lúpica classe V). Em menos de seis meses sem AINEs houve uma remissão completa da síndrome nefrótica. Neste artigo discutimos a etiologia da doença glomerular desta doente como efeito adverso do tratamento com AINEs versus doença glomerular associada a AR/LES (Rúpus).
Palavras-chave: Anti-inflamatórios não esteróides; Artrite Reumatóide; Lúpus Eritematoso Sistémico; Nefrite Lúpica; Nefropatia Membranosa; Síndrome Nefrótica; Rúpus.
INTRODUCTION
Connective tissue diseases are a family of closely related disorders, which include rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), systemic sclerosis, Sjogrens syndrome and others. They have a number of common features and sometimes overlap with each other, sharing certain clinical symptoms, signs and laboratory abnormalities1.
The majority of people with lupus have lupus alone. Although between 5% and 30% of people with lupus report having overlap symptoms, the likelihood of a person with lupus having a superimposed rheumatoid arthritis is 1%1,2.
Among the multisystemic manifestations of connective diseases there are a number of possibly associated renal manifestations. Particularly, 30% to 50% of patients with lupus will have clinically evident renal disease at presentation and approximately 10% to 20% of patients with lupus nephritis will have membranous nephropathy (MN), which takes the designation of class V lupus nephritis3.
There are some histologic findings which are suggestive of underlying lupus, both in immunofluorescence (deposits of IgG, IgA, IgM, C3 and C1q, known as full house staining) and in electron microscopy (subendothelial and subepithelial immune deposits and tubuloreticular inclusions in the glomerular endothelial cells)4.
Moreover, patients with connective diseases are prone to develop other forms of glomerular diseases related to treatment. Exposure to a variety of agents has been implicated in the development of MN, including penicillamine, parenteral gold salts, nonsteroidal anti-inflammatory drugs (NSAIDs) and possibly anti-tumour necrosis factor agents. Discontinuation of the responsible drug leads to resolution of the proteinuria in virtually all cases5.
CASE REPORT
We present a 45-year-old Caucasian female with a 4-year diagnosis of rheumatoid arthritis, fulfilling more than 4 criteria of the 1987 American College of Rheumatology classification criteria for RA, namely symmetrical polyarthritis of more than 3 joints with hand involvement, morning stiffness, rheumatoid nodules and elevated serum rheumatoid factor (RF) (126 UI/ mL) with positive anti-cyclic citrullinated peptide antibodies (ACPA). She lacked any relevant radiographic findings.
Since the diagnosis, her disease was partially controlled with low dose prednisolone (less than 10 mg per day), methotrexate (which she did for less than a year due to herpes zoster infection and leukopenia) and diclofenac. Recently, in a global medical evaluation, the presence of double strand DNA antibodies (21 UI/ mL), antinuclear antibodies (1:640) and isolated proteinuria (3300 mg per 24 hours) was detected. Furthermore, complement C3 levels, which were initially normal, started to slightly decrease (minimum 73 mg/dL). Accordingly, a nephrologic work-up was requested. She had hypoalbuminemia (2.0 g/dL), but no significant peripheral or periorbital oedema and a normal serum creatinine (0.8 mg/dL).
Urine sediment revealed rare leucocytes and the absence of erythrocytes. Serological viral markers (HBV, HCV and HIV) were negative.
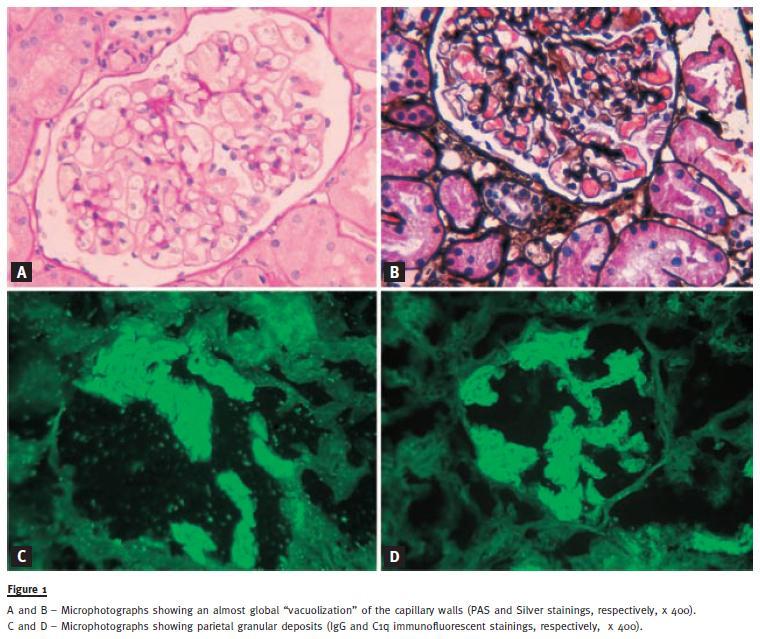
The patient was under hydroxychloroquine 400 mg/day, prednisolone 7.5 mg/day and diclofenac 50 mg thrice daily when she was first observed. One of our first measures was to stop the intake of nonsteroidal anti-inflammatory drugs (diclofenac) and started ramipril 2.5 mg/day, titrated to the maximum tolerated dose. Laboratory revaluation at 3 months showed an increase in proteinuria (6200 mg/day), which led us to perform a kidney biopsy. Surprisingly, the histological exam revealed a membranous nephropathy stage 1 with immunohistology showing positive staining for IgG (++), C3 (+/-), C1q (+/++) and IgM (+/-). The nephropathologist suggested an eventual class V lupus nephritis (Fig.1).
This latest finding led us to definitely rethink the diagnosis of RA and assume an overlapping syndrome RA/ SLE (Rhupus). One month after biopsy, unexpectedly, the proteinuria dropped to 450 mg/day with sustained decreases afterwards until complete remission (less than 300 mg/day), which is maintained after a year and counting. The titres of ANA (1:640), Anti-dsDNA (18-27 UI/ mL) and ACPA remained elevated afterwards, and there was a mild reduction of C3 (75-90 mg/dL). Again this led us to reconsider the aetiology of the glomerular disease responsible for the nephrotic syndrome presented on admission.
DISCUSSION
When the kidney is affected in RA, we can expect mainly three renal lesions responsible for proteinuria: membranous nephropathy, secondary amyloidosis and minimal change disease6,7. Membranous nephropathy is the most common glomerular lesion found in RA patients with proteinuria and it can be due to the disease itself or its therapy (mainly gold, penicillamine and NSAIDs). The course of RA associated membranous nephropathy is similar to that of the idiopathic disease, although spontaneous remissions appear to be highly unlikely. However, MN associated with RA treatment is most likely to remit after discontinuance of the drug8.
Secondary amyloidosis (AA) is found in 5 to 20% of patients with RA undergoing a renal biopsy6,9. However, this would not be our first guess in our patient, since there is not a so prolonged history of inflammation. Lastly, minimal change disease is usually associated with NSAID therapy but it is associated to higher degrees of proteinuria7.
Our patient fulfils RA criteria and has immunologic markers that favour that diagnosis, RF and ACPA, the latter being highly specific. This does not mean that she cannot have lupus too. In fact, she has polyarthritis, abnormal ANA and anti-dsDNA titres and a renal biopsy with an immunofluorescence pattern suggestive of lupus nephritis. Thus, we recognize we are facing a case of overlap syndrome RA and LES, known by many authors as Rhupus1,2. The exact definition of Rhupus is still in debate.
Most suggest a clinical condition in which clinical signs and symptoms of both SLE and RA occur. This hypothesis is supported by the coexistence of specific autoantibodies for SLE (anti-dsDNA and anti-SM) and RA (ACPA)10,11. On the other hand, other authors claim that Rhupus syndrome should be regarded as an erosive subset of lupus arthropathy12. There have been about 140 patients reported in the literature to date1. In Rhupus patients, extrarticular SLE manifestations are traditionally considered as less severe and less frequent. However, more recent studies showed that the frequency of glomerulonephritis (7.7-37.5%), for instance, is similar to that reported in SLE patients1,2.
Very few data are available on the treatment of Rhupus. The suggested regimens are the same used to prevent progression of erosive arthritis in RA, including corticosteroids, methotrexate and leflunomide.
Mycophenolate mofetil and cyclosporin A have also been reported to be effective in anecdotal cases13,14.
The glomerular lesion found in our patient, responsible for her proteinuria, is undoubtedly a membranous nephropathy, but the question here is its aetiology. The almost full house pattern found in the biopsys immunofluorescence favours a lupus nephritis, as suggested by the nephropathologist report.
Apart from lupus, the full house immunofluorescence pattern may also be seen in patients with endocarditis, HIV, hepatitis C, a portosystemic shunt, and post-streptococcal glomerulonephritis15-18, none of which was the case. Against lupus nephritis is that spontaneous remission of heavy proteinuria occurs in only a minority of class V lupus nephritis19. Thus, this is epidemiologically a remote possibility.
On the other hand, a reasonable, and our best hypothesis to explain this patients membranous nephropathy is its association to an adverse effect of NSAIDs, diclofenac, to be precise.
Although initial reports found that most cases of NSAID-induced nephrotic syndrome that were biopsied had minimal change disease, it is now evident that MN can also occur. The association of NSAIDs with MN was illustrated in a study of 125 patients with a biopsy diagnosis of MN20,21. Twentynine patients were taking a NSAID and 13 (10,4% of the study population) fulfilled three criteria suggesting that the NSAID was responsible: no other apparent cause for the MN, resolution of proteinuria within 1 to 36 weeks of discontinuing NSAIDs and no recurrence of proteinuria at follow-up (5 months to 13 years). In our patient we found the last two criteria. We admit that non-immunosuppressive therapy with angiotensin system inhibition and the corticotherapy used to treat extra-renal manifestations might have accelerated proteinurias resolution.
Many of the patients who developed MN associated with NSAIDs had been treated with diclofenac, but probably any NSAID can be involved, including COX-2 inhibitors21,22.
We can integrate the immunofluorescence here as a mere incidental finding explained by a deposition of circulating immunocomplexes in the glomerular tuft in a patient with lupus (only c1q and IgG were present at significant levels). We do not even know its exact location on the capillary wall, since electron microscopy evaluation was not performed. We believe they were there but not truly affecting the glomerular filtration barrier. We could have done a new biopsy once the remission was achieved, believing the same deposits would have been found, but for ethical reasons we did not do it.
Ultimately, we can hypothesize that this patient has asymptomatic membranous lupus nephritis with a superimposed minimal change disease due to NSAIDs which was responsible for the renal manifestations and resolved on their discontinuation.
Once again an electron microscopy specimen would probably help to clarify this situation. Apart from all the diagnostic considerations we have done, this case highlights that simple therapeutic actions like removing NSAIDs to this patient, can obviate the need for more aggressive treatments such as immunosuppression (needed to treat lupus nephritis class V) and its potential severe adverse effects.
References
1. Iaccarino L, Gatto M, Bettio S, t al. Overlap connective tissue disease syndromes. Autoimmun Rev 2013;12(3):363-373
2. Tani C, DAniello D, Delle Sedie A, et al. Rhupus syndrome: assessment of its prevalence and its clinical and instrumental characteristics in a prospective cohort of 103 SLE patients. Autoimmun Rev 2013;12(4):537-541 [ Links ]
3. Waldman M, Appel GB. Update on the treatment of lupus nephritis. Kidney Int 2006;70(8):1403-1412 [ Links ]
4. Jennette JC, Iskandar SS, Dalldorf FG. Pathologic differentiation between lupus and nonlupus membranous glomerulopathy. Kidney Int 1983;24(3):377-385 [ Links ]
5. Beck LH, Salant DJ. Causes and diagnosis of membranous nephropathy. UpToDate B, DS (Ed), editor: UpToDate, Waltham, MA; 2013 [ Links ]
6. Helin HJ, Korpela MM, Mustonen JT, Pasternack AI. Renal biopsy findings and clinicopathologic correlations in rheumatoid arthritis. Arthritis Rheum 1995;38(2):242-247 [ Links ]
7. Nakano M, Ueno M, Nishi S, Shimada H, et al. Analysis of renal pathology and drug history in 158 Japanese patients with rheumatoid arthritis. Clin Nephrol 1998;50(3):154-160 [ Links ]
8. Whelton A. Nephrotoxicity of nonsteroidal anti-inflammatory drugs: physiologic foundations and clinical implications. Am J Med 1999;106(5B):13S-24S [ Links ]
9. Gertz MA, Kyle RA. Secondary systemic amyloidosis: response and survival in 64 patients. Medicine (Baltimore) 1991;70(4):246-256 [ Links ]
10. Amezcua-Guerra LM, Springall R, Marquez-Velasco R, Gomez-Garcia L, Vargas A, Bojalil R. Presence of antibodies against cyclic citrullinated peptides in patients with rhupus: a cross-sectional study. Arthritis Res Ther 2006;8(5):R144 [ Links ]
11. Simon JA, Granados J, Cabiedes J, Morales JR, Varela JA. Clinical and immunogenetic characterization of Mexican patients with rhupus. Lupus 2002;11(5):287-292 [ Links ]
12. Fernandez A, Quintana G, Matteson EL, et al. Lupus arthropathy: historical evolution from deforming arthritis to rhupus. Clin Rheumatol 2004;23(6):523-526 [ Links ]
13. Artifoni M, Puechal X. How to treat refractory arthritis in lupus? Joint Bone Spine 2012;79(4):347-350 [ Links ]
14. Fernandez A, Quintana G, Rondon F, t al. Lupus arthropathy: a case series of patients with rhupus. Clin Rheumatol 2006;25(2):164-167
15. Haas M, Kaul S, Eustace JA. HIV-associated immune complex glomerulonephritis with lupus-like features: a clinicopathologic study of 14 cases. Kidney Int 2005;67(4):1381-1390 [ Links ]
16. Lee LC, Lam KK, Lee CT, Chen JB, Tsai TH, Huang SC. Full house proliferative glomerulonephritis: an unreported presentation of subacute infective endocarditis. J Nephrol 2007;20(6):745-749 [ Links ]
17. Ramos-Casals M, Font J, Garcia-Carrasco M, t al. Hepatitis C virus infection mimicking systemic lupus erythematosus: study of hepatitis C virus infection in a series of 134 Spanish patients with systemic lupus erythematosus. Arthritis Rheum 2000;43(12):2801-2806
18. Smet AD, Kuypers D, Evenepoel P, t al. Full house positive immunohistochemical membranoproliferative glomerulonephritis in a patient with portosystemic shunt. Nephrol Dial Transplant 2001;16(11):2258-2262
19. Gonzalez-Dettoni H, Tron F. Membranous glomerulopathy in systemic lupus erythematosus. Adv Nephrol Necker Hosp 1985;14:347-364 [ Links ]
20. Campistol JM, Galofre J, Botey A, Torras A, Revert L. Reversible membranous nephritis associated with diclofenac. Nephrol Dial Transplant 1989;4(5):393-395 [ Links ]
21. Radford MG, Jr, Holley KE, Grande JP, t al. Reversible membranous nephropathy associated with the use of nonsteroidal anti-inflammatory drugs. JAMA 1996;276(6):466-469 [ Links ]
Dr Ricardo Santos
Department of Nephrology,
Hospital do Espirito Santo de Evora, E.P.E.
Largo Senhor da Pobreza
7000-811 Evora
Portugal
E-mail: r.oliveira.santos@gmail.com
Conflict of interest statement. None declared.
Acknowledgments: The authors gratefully acknowledge Dr Fernanda Carvalho and Dr Helena Viana for the kidney biopsy figures Department of Renal Morphology, Hospital Curry Cabral, Lisbon, Portugal).
Received for publication: 28/08/2013 Accepted in revised form: 18/11/2013


{kind=link}