










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.28 no.2 Lisboa jun. 2014
ORIGINAL ARTICLE
Peritoneal dialysis in patients with vascular access problems
Diálise peritoneal em doentes com problemas de acesso Vascular
Cristina Silva1, Cristina Pinto Abreu2, Sofia Jorge2, Nuno Afonso1, Armando Carreira1, Antonio Gomes da Costa2
1Department of Nephrology, Centro Hospitalar e Universitário Coimbra – Hospital Geral. Coimbra, Portugal.
2 Department of Nephrology and Renal Transplantation, Centro Hospitalar Lisboa Norte – Hospital de Santa Maria. Lisboa, Portugal.
ABSTRACT
Vascular access problems are an important cause of compulsory transfer to peritoneal dialysis. Surprisingly, little is known about the effect of these transfers on peritoneal dialysis adequacy, patient or technique survival.
We have analysed retrospectively a cohort of 75 patients treated at the Peritoneal Dialysis Unit of Centro Hospitalar Lisboa Norte – Hospital de Santa Maria during the year 2011. Vascular access problems were defined clinically. Patient characteristics, peritoneal dialysis features and survival were compared between patients with (group 1, n = 14) and without vascular access problems (group 2, n = 61).
In group 1, significantly more patients were Black and had been transferred from haemodialysis, with a considerably longer time spent on this technique. These patients were more likely to be anuric, with an inferior daily total fluid removal, lower renal and total creatinine clearance, and poorer Kt/V for urea. Peritoneal clearance and peritoneal membrane transport type did not differ between groups.
Group 1 had a considerably higher exit site infection and peritonitis rate, and a lower albumin level. No significant differences were observed in unadjusted patient or technique survival between the two study groups. In the Cox multiple regression model, only a higher total creatinine clearance significantly and positively influenced the technique survival.
In conclusion, the prevalence of vascular access problems of the Peritoneal Dialysis Unit was 18.7% and it justified 78.6% of transfers from the Haemodialysis Unit. These were not the ideal patients for peritoneal dialysis. Nonetheless, our data suggest that the outcome (patient and technique survival) of patients with mandatory transfer to peritoneal dialysis because of vascular access problems is similar to that achieved in patients without vascular access problems. Total creatinine clearance appeared as an independent protective factor of technique survival.
Key-Words: Haemodialysis; peritoneal dialysis; survival; vascular access problems.
RESUMO
Os problemas de acesso vasculares sao uma causa importante de transferencia obrigatoria para dialise peritoneal. Surpreendentemente, pouco e conhecido sobre os efeitos destas transferencias na adequação da dialise peritoneal, sobrevida do paciente ou da tecnica.
Analisamos retrospetivamente um grupo de 75 pacientes tratados na Unidade de Dialise Peritoneal do Centro Hospitalar Lisboa Norte – Hospital de Santa Maria no ano 2011. Os problemas de acesso vascular foram definidos clinicamente. As caracteristicas e sobrevida dos pacientes foi comparada entre os doentes com (grupo 1, n = 14) e sem problemas de acesso vascular (grupo 2, n = 61).
No grupo 1 havia um numero maior de doentes de raca negra e transferidos de hemodialise, com um tempo dispendido nesta tecnica consideravelmente superior. Estes doentes eram mais propensos a anuria, menor remocao total de fluidos/dia, menor depuracao de creatinina renal e total, e inferior Kt/V da ureia. A depuracao de creatinina peritoneal e o tipo de transportador de membrana peritoneal nao divergiu entre os grupos. As taxas de infeccao do orificio de saida e peritonite foram superiores no grupo 1, a albuminemia era menor nestes doentes. Nao se verificaram diferencas na sobrevida dos doentes ou tecnica (metodo >Kaplan-Meier). No modelo de regressao >Cox, apenas valores superiores de depuracao de creatinina total influenciaram de forma significativa e positiva a sobrevida da tecnica.
Em conclusao, na Unidade a prevalencia de problemas de acesso vascular foi 18.7%, e isso justificou 78.6% das transferencias da Unidade de Hemodialise. Estes nao seriam os doentes ideais para dialise peritoneal. No entanto, os dados sugerem que a sobrevida (paciente e tecnica) de doentes com transferência obrigatoria para dialise peritoneal por problemas de acesso vascular e similar a de doentes sem problemas de acesso vascular. A depuracao de creatinina total surgiu como fator protetor independente da sobrevida da tecnica.
Palavras-chave: Dialise peritoneal; hemodialise; problemas do acesso vascular; sobrevida.
INTRODUCTION
In the concept of integrated care, haemodialysis (HD) and peritoneal dialysis (PD) are regarded as complementary methods of renal replacement therapy and these two modalities should be used to achieve the best patients outcome1,2.
In an integrated care model, it is well recognized that the technique survival remains unsatisfactory in PD, with as many as 10–20% of PD patients being transferred annually to HD3,4. The major causes of PD technique failure are peritonitis and ultrafiltration failure3,5-9. Technique failure in HD is far less common.
However, as HD is more prevalent than PD, a substantial percentage of PD patients have been transferred from HD, ranging from 15 to 25% in many PD programmes3,7,10,11. The main reasons for such transfers are vascular access problems, cardiac disease and patient preference12.
The clinical course of patients entering PD therapy because of vascular access problems is scarcely known. Based on this concern, the aim of this work was to assess patient characteristics, PD adequacy and outcome in this group of patients.
SUBJECTS AND METHODS
Study design
This observational cross -sectional study enrolled 75 patients attending the PD unit of Centro Hospitalar Lisboa Norte – Hospital de Santa Maria, Portugal, from January to December 2011. No patients treated during that time were excluded from the analysis or were lost to follow-up.
Patient characteristics, PD features and outcome (patient and technique survival) were compared between PD patients with and without vascular access problems (group 1 and 2, respectively).
Definitions
Patients transferred from HD were defined as those who had been treated with HD for ≥ 3 consecutive months and HD had been chosen initially as a long-term therapy. Patients who were treated temporarily with the use of central vein catheters in a bridge-in period before starting PD were not included in this group. Patients with vascular access problems were defined clinically (≥ 2 cases/patient of primary failure of arteriovenous fistula, ≥ 2 cases/patient of arteriovenous fistula or graft thrombosis and patients with vascular access exhaustion). Patient comorbidity was assessed according to Charlson comorbidity index13 (not age adjusted). Patient priority in kidney transplantation was defined through clinical classification as super-urgent (only ABO blood group compatibility and negative crossmatch required) and U1 or U2 (1 or 2 human leukocyte antigen locus compatibility required). Clinical and laboratory parameters were evaluated at the end of the observation period. Total fluid removal was calculated from the sum of 24 hours peritoneal ultrafiltration and diuresis. The latest clearance studies and peritoneal equilibration tests with 3.86% glucose were analysed. The Watson formula14 was used to estimate total body water in the Kt/V calculations, and the Du Bois equation15 was employed for calculation of body surface area in normalized creatinine clearance.
Survival analysis
In patient survival analysis, only death was considered as a final event and patients were censored at transplantation, transfer to HD, recovery of renal function or at the end of the observation period.
In the technique survival analysis, both transfer to HD and super-urgent transplantation were regarded as final events, and patients were censored at U1 or U2 transplantation, recovery of renal function, death or at the end of the study. Short -term treatment switch to HD following catheter removal due to peritonitis or other technical problems, with a subsequent return to PD, was ignored in the analysis.
Statistical analysis
Parametric variables were expressed as mean ± standard deviation (SD) and were compared using students t -test. Non -parametric variables were expressed as median and interquartile range (IQR) and compared using Mann -Whitney test. Categorical variables were expressed in percentages and were compared using the chi -squared test. Survival was analysed by Kaplan - Meier and Cox proportional hazards modelling. All p-values were 2-tailed and values < 0.05 were considered statistically significant.
Confidence intervals included 95% of predicted values. Analyses were carried out using SPSS software (version 20; SPSS Inc. Chicago IL, USA).
RESULTS
Population
Of 75 patients enrolled in the study, 25 were incident patients. Peritoneal dialysis was the initial method of renal replacement therapy in 52 patients, 18 had been transferred from HD to PD (owing to vascular access problems in 11, patient preference in six and Heparin-induced thrombocytopenia in one), and five patients had come into PD after a renal allograft loss.
The median observation period was 10.8 months (interquartile range 6.2–12 months). During the time of observation, 10 patients were transferred to HD, kidney transplantation was performed in seven patients (super -urgent in two), recovery of renal function occurred in four patients and there was one death. Fifty-three patients were still on PD at the end of the study.
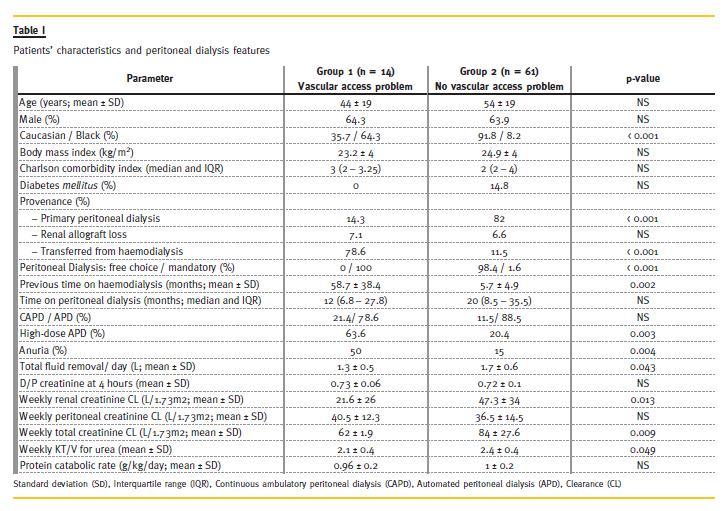
The prevalence of vascular access problems of the Peritoneal Dialysis Unit was 18.7% (group 1, n = 14). Patient characteristics and PD features of the two groups are given in Table I.
Patients with vascular access problems
In group 1, relatively more patients were Black and had been transferred from HD, with a considerably longer time spent on this technique. As expected, group 1 had an appreciably higher prevalence of anuria, lower renal creatinine clearance and daily total fluid removal. The D/P values for creatinine at 4 hours did not differ between groups. Peritoneal clearance did not reach a significant difference even though the greater frequency of high -dose automated peritoneal dialysis (APD) in group 1. Both weekly Kt/V for urea and total creatinine clearance were much lower in this group (Table I).
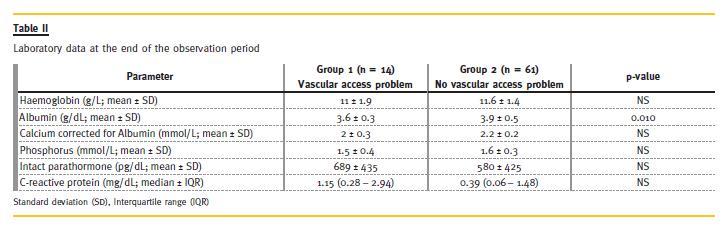
Group 1 had a considerably lower albumin level (Table II). The prevalence of peritoneal catheter exit site infection was significantly higher in group 1 when compared to patients on group 2 (0.70 versus 0.24 episode/patient. year, p < 0.001), as well as the rate of peritonitis (0.80 versus 0.23 episode/patient.year, < 0.001).
Patient survival
The single patient who died during the study was from group 2. There was no significant difference in unadjusted patient survival between groups (p = 0.796).
In the Cox proportional hazard model (adjusted for age, Charlson comorbidity index and previous HD), the relative risk of death was not significantly higher in patients who had vascular access problems (p = 0.994).
Technique survival
Of patients from group 2, four recovered renal function, 10 were transferred to HD and five underwent U1 or U2 transplantation. In group 1, there were two exits for super -urgent transplantation. There was no difference in unadjusted technique survival between the two study groups (Fig. 1).
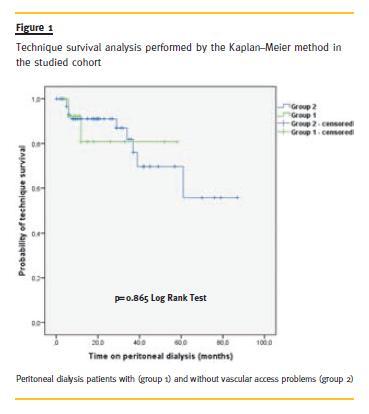
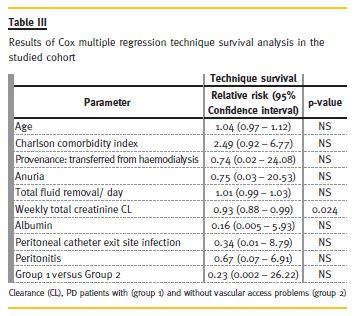
In Cox multiple regression technique survival analysis, PD patients with and without vascular access problems (group 1 or 2) were included into the model together with age, Charlson comorbidity index, previous HD, anuria, daily total fluid removal, weekly total creatinine clearance, serum albumin, peritoneal catheter exit site infection and peritonitis rate. In this model, there was no difference in technique survival between groups, and only weekly total creatinine clearance significantly and positively influenced technique survival (Table III).
DISCUSSION
Both HD and PD are interchangeable and complementary renal replacement therapy modalities, along with kidney transplantation. Patients can be transferred from one modality to another for various reasons, and the cause of the transfer may strongly affect the outcome11. Vascular access problems are an important reason of mandatory transfer to PD.
In this single centre observational study, PD was the primary therapy for the majority of patients. For the remaining, 24% had been treated previously with HD and 6.7% had entered PD after a failed transplant.
The prevalence of vascular access problems was 18.7%, and it was the cause of transfer from HD to PD in 78.6% patients, with mandatory transfer to PD in all cases.
The elevated percentage of patients transferred from HD was probably due to the fact that the Centre receives HD patients from Portuguese-speaking African countries. These patients had long-standing complications in HD, predominantly vascular access problems.
In some studies11,12,16 most of the patients were transferred from HD to PD as a result of vascular problems. Similarly to our study, Koc et al.11 has reported a 70% frequency of compulsory transfer to PD due to vascular problems.
In our PD Unit, the two study groups did not differ substantially, except for more Black patients and a significantly higher prevalence and median time on HD in group 1. Therefore, it was not surprising that these patients were more likely to be anuric, with an inferior daily total fluid removal and lower renal creatinine clearance. Despite the greater frequency of high-dose APD in patients with vascular problems, peritoneal clearances did not differ significantly. Both weekly Kt/V for urea and total creatinine clearance were much lower in these patients, because of reduced residual renal function.
Peritoneal catheter exit site infection and peritonitis rate were higher in group 1. Black race17,18, transfer from HD to PD18 and loss of residual renal function19 were independent predictors of peritonitis.
Given the prevalence of all these features in the case-mix of group 1, it might explain their elevated peritonitis rate.
The lower albumin level in group 1 was possibly secondary to the inflammatory state. These patients had higher C -reactive protein levels, although it did not reach statistical significance in the analysis.
It has to be taken into account that patients who are transferred between renal replacement therapy modalities due to problems with one technique are often negatively selected and are predisposed to lower survival, irrespective of the direction of transfer10.
However, the selection may also be positive, as many fragile patients might have not survived to the point of transfer, leaving the more healthy population12.
In our study, there was no difference in survival between patients with and without vascular access problems. Liberek et al.12 also did not detect any influence of previous HD on patient survival, in contrast to most papers3,10,11,16,20-22.
In our series, technique survival did not diverge between patients with and without vascular access problems. A higher total creatinine clearance was found to be independently associated with a longer PD technique survival. None of the other predictor variables influenced technique survival, namely peritoneal dialysis -related infections. This latter fact is in disagreement with the literature12 and can be explained by the short follow-up of the study.
Peritoneal dialysis was a mandatory choice for all our PD patients with vascular access problems, and many of these patients were not obviously the ideal candidates for PD.
In our view, these results should be interpreted within the context of the studys limitations. As in all observational studies, the possibility of residual confounding or misclassification of outcomes cannot be excluded. Our case -mix was small, a joint analysis of incident and prevalent patients was performed, patients with vascular access problems (from primary PD, after renal allograft loss and transferred from HD) were analysed altogether, and our follow-up was short. Finally, there was only one death in the study period, which could compromise the evaluation of patient survival.
Future prospective multicentre studies should be ideally conducted in order to confirm the findings presented herein.
In conclusion, the prevalence of vascular access problems of the PD Unit was 18.7% and it justified 78.6% of transfers from HD. These were not the ideal patients for PD (lower residual renal function and fluid removal, higher peritoneal dialysis-related infections rate). Nonetheless, our data suggest that the outcome (patient and technique survival) of patients with mandatory transfer to PD because of vascular access problems is similar to that achieved in patients without vascular access problems. Finally, total creatinine clearance appeared as an independent protective factor of PD technique survival.
References
1. Coles GA, Williams JD. What is the place of peritoneal dialysis in the integrated treatment of renal failure? Kidney Int 1998;54(6):2234–2240. [ Links ]
2. Lameire N, Van Biesen W, Vanholder R. The role of peritoneal dialysis as first modality in an integrative approach to patients with end -stage renal disease. Perit Dial Int 2000;20(Suppl 2):134–141. [ Links ]
3. Guo A, Mujais S. Patient and technique survival on peritoneal dialysis in the United States: evaluation in large incident cohorts. Kidney Int Suppl 2003;88:S3–12. [ Links ]
4. Afolalu B, Troidle L, Osayimwen O, Bhargava J, Kitsen J, Finkelstein FO. Technique failure and center size in a large cohort of peritoneal dialysis patients in a defined geographic area. Perit Dial Int. 2009;29(3):292 -296. [ Links ]
5. Davies SJ, Phillips L, Griffiths AM, Russell LH, Naish PF, Russell GI. What really happens to people on long -term peritoneal dialysis? Kidney Int 1998;54(6):2207–2217. [ Links ]
6. Lupo A, Tarchini R, Carcarini G, et al. Long -term outcome in continuous ambulatory peritoneal dialysis: a 10 -year -survey by the Italian Cooperative Peritoneal Dialysis Study Group. Am J Kidney Dis 1994;24(5):826–837. [ Links ]
7. Van Biesen W, Vanholder RC, Veys N, Dhondt A, Lameire NH. An evaluation of an integrative care approach for end -stage renal disease patients. J Am Soc Nephrol 2000;11(1):116–125. [ Links ]
8. Maiorca R, Cancarini GC, Brunori G, et al. Comparison of long-term survival between hemodialysis and peritoneal dialysis. Adv Perit Dial 1996;12:79–88. [ Links ]
9. Van Biesen W, Dequidt C, Vijt D, Vanholder R, Lameire N. Analysis of the reasons for transfers between hemodialysis and peritoneal dialysis and their effect on survivals. Adv Perit Dial 1998;14:90–94. [ Links ]
10. Heaf JG, Lokkegaard H, Madsen M. Initial survival advantage of peritoneal dialysis relative to haemodialysis. Nephrol Dial Transplant 2002;17(1):112–117. [ Links ]
11. Koc Y, Unsal A, Basturk T, et al. Is there impact of mortality prior hemodialysis therapy in peritoneal dialysis patients? Nefrologia 2012;32(3):335-342. [ Links ]
12. Liberek T, Renke M, Skonieczny B, et al. Therapy outcome in peritoneal dialysis patients transferred from haemodialysis. Nephrol Dial Transplant 2009;24(9):2889-2894. [ Links ]
13. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987;40(5):373–383. [ Links ]
14. Watson PE, Watson ID, Batt RD. Total body water volumes for adult males and females estimated from simple anthropometric measurements. Am J Clin Nutr 1980;33(1):27–39. [ Links ]
15. Du Bois D, Du Bois EF. Clinical calorimetry. Tenths paper to estimate the approximate surface area if height and weight be known. Arch Int Med 1916;17:863-871. [ Links ]
16. Sipahioglu MH, Aybal A, Unal A, Tokgoz B, Oymak O, Utas C. Patient and technique survival and factors affecting mortality on peritoneal dialysis in Turkey: 12 years experience in a single center. Perit Dial Int 2008;28(3):238-245. [ Links ]
17. Kim GC, Vonesh EF, Korbet SM. The effect of technique failure on outcome in black patients on continuous ambulatory peritoneal dialysis. Perit Dial Int 2002;22(1):53-59. [ Links ]
18. Nessim SJ, Bargman JM, Austin PC, Nisenbaum R, Jassal SV. Predictors of peritonitis in patients on peritoneal dialysis: results of a large, prospective Canadian database. Clin J Am Soc Nephrol 2009;4(7):1195-1200. [ Links ]
19. Han SH, Lee SC, Ahn SV, et al. Reduced residual renal function is a risk of peritonitis in continuous ambulatory peritoneal dialysis patients. Nephrol Dial Transplant 2007;22(9):2653–2658. [ Links ]
20. Zhang X, Han F, He Q, et al. Outcomes and risk factors for mortality after transfer from hemodialysis to peritoneal dialysis in uremic patients. Perit Dial Int 2008;28(3):313-314. [ Links ]
21. Lobbedez T, Crand A, Le Roy F, Landru I, Quere C, Ryckelynck JP. Transfer from chronic haemodialysis to peritoneal dialysis. Nephrol Ther 2005;1(1):38 -43. [ Links ]
22. Portoles J, Del Peso G, Fernandez -Reyes MJ, Bajo MA, Lopez - Sanchez P; GCDP. Previous comorbidity and lack of patient free choice of technique predict early mortality in peritoneal dialysis. Perit Dial Int 2009;29(2):150-157. [ Links ]
Dr. Cristina Miguel Correia Silva
Rua Luciano Freire 6 r/c 1600-143 Lisboa, Portugal
Email: cristinamcsilva@gmail.com
Conflict of interest statement: None declared.
Received for publication: 09/12/2013
Accepted in revised form: 21/04/2014


{kind=link}
{kind=link}