










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.29 no.1 Lisboa mar. 2015
CASE REPORT
Successful treatment of calcific uremic arteriolopathy with pamidronate
Tratamento bem sucedido da arteriolopatia urémica calcificante com pamidronato
Emanuel Ferreira, Maria Marques, Helena Pinto, Nsecumesso Bota, Ana Belmira, Armando Carreira, Mario Campos
Department of Nephrology, Centro Hospitalar e Universitário de Coimbra – Hospital Geral. Coimbra, Portugal
ABSTRACT
Calcific uremic arteriolopathy is a rare, life-threatening obliterative small vessel vasculopathy, most commonly seen in patients with chronic renal failure. The most prominent feature of this disease is painful lesions on various areas of the skin surface. It has a complex and poorly understood pathogenesis, which limits treatment strategies. Despite all the controversies, bisphosphonates have been successfully applied in some patients. Our paper describes a case of calcific uremic arteriolopathy in a 33-year-old woman undergoing peritoneal dialysis, successfully treated with pamidronate.
Key-Words: Bisphosphonates; calcific uremic arteriolopathy; chronic kidney disease; therapy; pamidronate.
RESUMO
A arteriolopatia urémica calcificante é uma vasculopatia obliterativa de pequenos vasos, rara e potencialmente mortal, que afecta principalmente doentes com insuficiência renal crónica. A principal característica desta doença é o aparecimento de lesões dolorosas envolvendo diferentes áreas da superfície cutânea. A sua patogenia é complexa e não está completamente esclarecida, o que limita a sua abordagem terapêutica. Apesar da controvérsia, os bifosfonatos têm sido utilizados com sucesso em alguns doentes. No presente artigo, descrevemos um caso de arteriolopatia urémica calcificante numa mulher de 33 anos de idade, em diálise peritoneal, com boa resposta à terapêutica com pamidronato.
Palavras-Chave: Arteriolopatia urémica calcificante; bifosfonatos; insuficiência renal crónica; pamidronato; terapêutica.
INTRODUCTION
Calcific uremic arteriolopathy (CUA), also called calciphylaxis1, is a rare, life-threatening disease characterized by mural calcification with intimal hyperplasia of small and medium-sized blood vessels, leading to occlusion of the vascular lumen2.
The pathogenesis is poorly understood3, but several risk factors have been associated with this condition, such as: end stage renal disease (ESRD), hyperparathyroidism, hypercalcaemia, hyperphosphatemia, warfarin therapy, use of vitamin D and calciumbased phosphate binders, female sex, Caucasian race, morbid obesity, recent weight loss, hypoalbuminemia and high levels of alkaline phosphatase4,5. Other risk factors frequently mentioned include the deficiency of vascular calcification inhibitors, such as fetuin-A and matrix Gla protein, and hypercoagulable states due to protein C and S deficiency6.
Clinically, CUA is characterized by areas of ischaemic necrosis of the dermis and subcutaneous fat2.
These ischaemic changes lead to livedo reticularis and/or violaceous, painful, plaque-like subcutaneous nodules that progress to ischaemic or necrotic ulcers within a few weeks2,7.
The diagnosis of CUA is mainly based on clinical judgment and should be suspected in patients with characteristic cutaneous features and related risk factors4. Skin biopsy of the lesions remains the gold standard to confirm the diagnosis since there are other disorders that may mimic CUA8.
Treatment strategies for CUA are limited by poor understanding of its pathophysiology3. Novel and experimental therapies have been evaluated, such as bisphosphonates and sodium thiosulfate9.
Bisphosphonates inhibit osteoclasts and are mainly used in the treatment of resorptive bone diseases, such as osteoporosis and Pagets disease of bone10.
A number of previous studies have shown that this class of drugs has beneficial effects on the evolution of experimental CUA11, which has led to its use in isolated cases of this disease9-13.
We present a case of CUA in a 33-year-old woman with end-stage renal disease requiring peritoneal dialysis, with good response to treatment with bisphosphonates.
CASE REPORT
The patient is a 33-year-old woman with congenital hydrocephaly secondary to type 2 Chiari malformation with ventricular-atrial shunt. She has been undergoing peritoneal dialysis, since June 2011, for ESRD secondary to a shunt nephritis. Her past medical history was also significant for paresis of the lower limbs and left upper limb secondary to bacterial meningitis in childhood, morbid obesity, dyslipidemia, secondary hyperparathyroidism (intact parathyroid hormone levels between 147-404 pg/mL; NR:16-87 pg/mL), stasis dermatitis of the lower limbs, pulmonary thromboembolism in 2009 and deep vein thrombosis of the lower right limb in 2006. Regarding her medication regimen, special mention is made of chronic medication with calcium carbonate (1g/day), aluminium hydroxide (1g/day), calcitriol (0.25μg/day) and warfarin. Calcitriol was administered at a dose of 0.25μg/day since 2010, after a hospitalization for severe seizures in the context of difficult to control hypocalcaemia secondary to chronic kidney disease.
In August 2011, she was admitted in the nephrology ward for volume overload and painful skin lesions, i.e., blood filled blisters, on the distal third of the right leg. She was seen by dermatology, which diagnosed pigmented purpuric dermatitis and recommended applying a moisturizer. In this admission, calcium carbonate was replaced by sevelamer carbonate.
In October 2011, the calcitriol was halted due to an intact parathyroid hormone (iPTH) of 26.2 pg/mL and stable calcium blood levels (2.35 mmol/L; NR: 2.1-2.55 mmol/L). The lesions on the right leg evolved into a highly infected ulcer and were treated on an outpatient basis with antibiotic therapy and local wound care. Since the lesion proved refractory to the treatment, the patient was admitted in the nephrology ward, in November and December, to boost the local therapy. An incisional biopsy was performed in the margins of the ulcer on the right leg, which disclosed focal loss of the epidermis covered by a superficial crust; underlying, there was infiltration by lymphocytes, macrophages and few neutrophils and mild dermal fibrosis; no specific diagnosis was proposed. The skin lesions evolved slowly but favourably with local therapy. Given the non-specificity of the biopsy and the suspicion of CUA, warfarin was replaced, in January 2012, with enoxaparin.
She was readmitted on the 9th April for worsening of the ulcer on the inner right leg. It was 6 cm in diameter with purulent exudate and necrotic edges.
She presented with another ulcer on the back of the left leg measuring 2 cm in diameter, with one necrotic edge (Fig. 1). Both lesions were very painful. Skin temperature was slightly warm around the ulcer in the right leg and normal in the left leg. Both peripheral pulses were palpable. Laboratory tests showed normal leukocyte count, hypoalbuminaemia (29g/L; NR: 35-50 g/L), elevated alkaline phosphatase (226 U/L; NR: 38-126 U/L), hyperphosphatemia (2 mmol/L; NR: 0.81-1.45 mmol/L), normocalcaemia (2.19 mmol/L) and elevated C-reactive protein (12.6 mg/dL; NR: < 1 mg/dL). Further coagulation tests were normal and auto-immune antibodies (antinuclear antibodies, extractable nuclear antigens, antineutrophil cytoplasmic antibodies, cryoglobulins, anticardiolipin antibodies and anti β>2-glycoprotein antibodies) were negative.
Ciprofloxacin, buprenorphine, pamidronate (30 mg, intravenous, a total of five administrations), and local care of skin lesions were initiated. The standard calcium dialysate (1.75 mmol/L) was also replaced by a dialysate with lower calcium content (1.25 mmol/L) at the start of hospitalization. On the 15th May, iPTH of 649 pg/mL with normal phosphatemia (0.93 mmol/L) and hypocalcaemia (1.45 mmol/L), led to the reinstatement of calcitriol (0.5 ug/day) and standard calcium dialysate. She was discharged on the 23rd May, free of pain and with complete re-epithelialization of the wound on the right leg and partial re-epithelialization of the wound on the left leg (Fig. 1). Two further administrations of pamidronate were given on an outpatient basis.
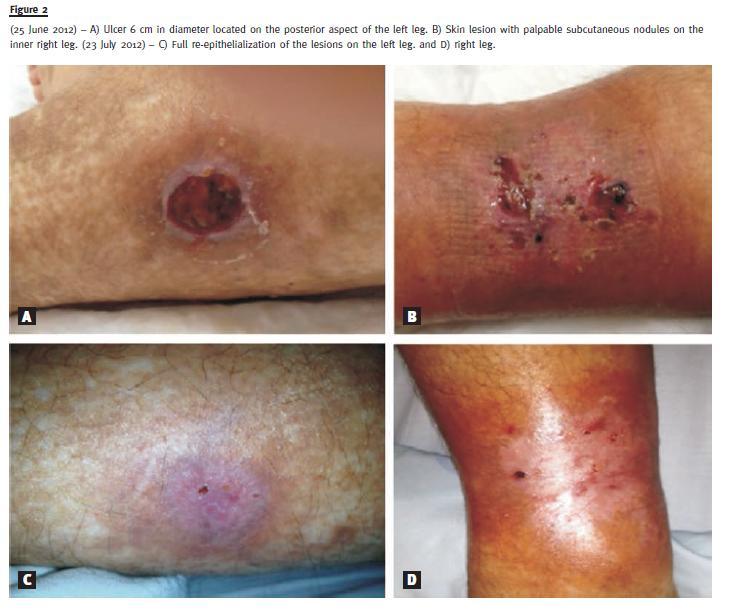
The patient was readmitted on the 25th June 2012, with a 6 cm diameter ulcer on the left leg and palpable subcutaneous nodules on the right leg (Fig. 2).
Laboratory tests showed normal leukocyte count, an iPTH level of 105 pg/mL, hypoalbuminemia (33 g/L), elevated alkaline phosphatase (186 U/L), hyperphosphatemia (2.52 mmol/L) and normocalcaemia (2.20 mmol/L). Bed rest and local care of skin lesions were intensified, calcitriol was stopped and pamidronate (3 administrations) and peritoneal dialysis with low-calcium dialysate were restarted. Low-calcium dialysate was discontinued one week after admission due to hypocalcaemia. She was discharged on the 23rd July 2012, with complete re-epithelialization of both lesions (Fig. 2).
After 22 months follow-up there was no further recurrence of CUA lesions, but the patient died of a non-CUA related cause.
DISCUSSION
Calcific uremic arteriolopathy has a higher incidence in patients with chronic kidney disease14, probably due to the uremic environment, higher prevalence of mineral metabolism disorders and iatrogenic causes associated with treatment with vitamin D and calcium-based phosphate binders5.
The histological picture of CUA is characterized by a triad: medial calcification of small and medium sized blood vessels, intima hyperplasia and necrosis of subcutaneous fat4. Histological evaluation may be helpful in equivocal cases of skin lesions, but a falsely negative result may occur in CUA, mainly when a single biopsy is performed7,15-17. In fact, the specificity and sensitivity of skin biopsies in the diagnosis of CUA have not been determined nor have definitive histologic criteria for making the diagnosis been established7. Besides the risk of sampling error, skin biopsy should not be routinely performed in CUA since it may inoculate or spread an infection and healing can be problematic8.
In our case, taking into account some doubts about the diagnosis, we decided to perform the biopsy but the pattern of changes was found to be non-specific.
The current literature argues that, in cases of inconclusive histological evaluation, a presumptive diagnosis of CUA should be made and treated accordingly if other causes have been excluded and a strong clinical suspicion of CUA remains7. The differential diagnosis of CUA includes entities such as vasculitis, peripheral vascular disease, cryoprecipitate disorders, antiphospholipid antibody syndrome, disseminated intravascular coagulation and cholesterol embolization3,4,7. These diseases were considered less likely in our case attending to clinical history, physical findings and diagnostic test results – normal skin temperature, intact peripheral pulses, bilateral necrosis without other generalized skin lesions and normal coagulation and autoimmune studies. Therefore, the diagnosis of CUA was advocated based on the typical history of CUA – painful, non-healing skin lesions in the setting of a patient with ESRD with multiple risk factors (hyperparathyroidism, hyperphosphatemia, Caucasian race, female gender, obesity, treated with warfarin, vitamin D analogues and calcium-based phosphate binders)4,6.
A multidisciplinary therapeutic approach was deemed appropriate to the presumably complex aetiology of CUA, with local wound care, adequate pain control with opiates and correction of related risk factors6,12. Local care of the skin wounds was based on cleansing with saline, the use of enzymatic debriding agents where there was necrotic tissue, and hydrogel dressings to stimulate granulation and epithelialization.
Infection is the primary cause of mortality in CUA7, so systemic antibiotics were given when there was suspicion of skin infection. The correction of risk factors included the suspension of warfarin and control of serum phosphorus and calcium with diet, administration of calcium-free phosphate binders, and performing peritoneal dialysis with low-calcium solutions3. Warfarin was discontinued because it reduces the vitamin k-dependent carboxylation of matrix Gla protein, a mineral-binding extra-cellular matrix protein that actively inhibits vascular calcification1.
Calcific uremic arteriolopathy also calls for the replacement of vitamin D analogues with calcimimetics for the control of hyperparathyroidism5. In agreement with current recommendations for mineral and bone disorder in chronic kidney disease18, we aimed to maintain iPTH levels in the range of two to nine times the upper limit for the assay. Our patient was medicated with calcitriol 0.25μg/day since a hospitalization, in 2010, for severely symptomatic hypocalcaemia secondary to chronic kidney disease.
Despite hyperphosphatemia, iPTH levels were maintained within the desired goal and calcium levels were normal. In October 2011, given the low iPTH levels (26.2 pg/mL), the stabilized calcium levels and the concern of CUA, calcitriol was discontinued.
However, in May 2012, it was necessary to temporarily reinstate it due to rising iPTH (649 pg/mL). At the concomitant hypocalcaemia (1.45 mmol/L), for which calcimimetics are not advisable19, proscribed their usage.
In recent years, novel agents like sodium thiosulfate and bisphosphonates have been infrequently but successfully used off-label, in addition to previously described general measures, in the treatment of CUA9-13,20-26. Sodium thiosulfate acts as a potent antioxidant and increases the solubility of calcium deposits, resulting in pain relief and successful wound healing within weeks to months of initiating therapy5. The most commonly reported dose in dialysis patients has been 25g three times weekly until complete resolution of lesions7. Adverse effects to monitor include metabolic acidosis, nauseas, vomiting and headache3. Likewise, the use of bisphosphonates is supported by their inhibitory effect on vascular calcification10 and their anti-inflammatory properties, resulting from inhibition of both macrophage activity and pro-inflammatory cytokines production6. Potential nephrotoxicity and, more especially, the risk of causing or worsening adynamic bone disease have raised questions about the safety use of bisphosphonates in chronic kidney disease1,9. However, some authors argue that since the bone-binding capacity of bisphosphonates is related to remodelling activity, its deposition will be reduced in the presence of adynamic bone disease9.
In addition, the high mortality in CUA probably outweighs the concern of worsening an adynamic bone disease1.
Since there are no randomized trials comparing bisphosphonates with sodium thiosulfate in CUA and drug approval process to use sodium thiosulfate would be time consuming and highly bureaucratic, we decided to use the former.
There is little information on the dosage of bisphosphonates in CUA, with reports of intravenous administration of pamidronate at a dose of 30 mg in 5-9 administrations, with a total treatment duration between 48 days and 3 months3,10,11. There are also references to success with alendronate, risendronate, etidronate and ibandronate9,12,13. We used intravenous pamidronate, 30 mg, in a total of 10 administrations over a period of 96 days. Response to treatment was good, with improved pain relief, full recovery of the lesions after 10 administrations and no recurrence after 24 months follow-up. Other than a transient reduction of calcium and phosphate, no side-effect was observed.
Although there are no prospective controlled studies comparing different therapeutic strategies, which have only been evaluated in a limited number of patients, this case demonstrates the efficacy and safety of bisphosphonates in the treatment of CUA.
References
1. New N, Mohandas J, John GT, et al. Calcific uremic arteriolopathy in peritoneal dialysis populations. Int J Nephrol 2011; 2011:982854. [ Links ]
2. Evenepoel P, Kuypers DR. Dermatologic Manifestations of Chronic Kidney Disease. In: Floege J, Johnson RJ, Feehally J, eds. Comprehensive Clinical Nephrology. Missouri: Saunders Elsevier, 2011:1004-1005. [ Links ]
3. Ross EA. Evolution of treatment strategies for calciphylaxis. Am J Nephrol 2011;34(5):460-467. [ Links ]
4. Pujar T, Spinello IM. A 44 year-old lady with chronic renal disease and intractable ulcers: a case report. Int Arch Med 2009;2(1):22. [ Links ]
5. Sowers KM, Hayden MR. Calcific uremic arteriolopathy: pathophysiology, reactive oxygen species and therapeutic approaches. Oxid Med Cell Longev 2010; 3(2):109-121. [ Links ]
6. Goel SK, Bellovich K, McCullough PA. Treatment of severe metastatic calcification and calciphylaxis in dialysis patients. Int J Nephrol 2011; 2011:701603. [ Links ]
7. Santos P, Hartle JE, Quarles LD. Calciphylaxis (calcific uremic arteriolopathy). Uptodate. 2013. Available at: www.uptodate.com/contents/calciphylaxis-calcific-uremicarteriolopathy?source=search_result&search=calcifilaxia&selectedTitle=1~16. Acess at 20/12/2013. [Updated 2013 Nov 21] [ Links ]
8. Mendes M, Ferreira AC, Ferreira A, Nolasco F. Calciphylaxis: a literature review based in two case reports. Port J Nephrol Hypert 2014; 28(1): 61-68. [ Links ]
9. Torregrosa JV, Durán CE, Barros X, et al. Successful treatment of calcific uraemic arteriolopathy with bisphosphonates. Nefrologia 2012;32(3):329-334. [ Links ]
10. Schliep S, Schuler G, Kiesewetter F. Successful treatment of calciphylaxis with pamidronate. Eur J Dermatol 2008;18(5):554-556. [ Links ]
11. Monney P, Nguyen QV, Perroud H, Descombes E. Rapid improvement of calciphylaxis after intravenous pamidronate therapy in a patient with chronic renal failure. Nephrol Dial Transplant 2004; 19(8):2130-2132. [ Links ]
12. Rodríguez-Villarreal I, Callejas R, Sánchez M, et al. Calcifilaxis o arteriolopatía urémica calcificante: combinación de tratamientos. NefroPlus 2010;3(3):39-44. [ Links ]
13. Shiraishi N, Kitamura K, Miyoshi T, et al. Successful treatment of a patient with severe calcific uremic arteriolopathy (calciphylaxis) by etidronate disodium. Am J Kidney Dis 2006; 48(1):151-154. [ Links ]
14. Brandenburg VM, Cozzolino M, Ketteler M. Calciphylaxis: a still unmet challenge. J Nephrol 2011; 24(2):142-148. [ Links ]
15. Fine A, Zacharias J. Calciphylaxis is usually non-ulcerating: risk factors, outcome and therapy. Kidney Int 2002;61(6):2210-2217. [ Links ]
16. Zhou Q, Neubauer J, Kern JS, Grotz W, Walz G, Huber TB. Calciphylaxis. Lancet 2014;383(9922):1067. [ Links ]
17. Stavros K, Motiwala R, Zhou L, Sejdiu F, Shin S. Calciphylaxis in a dialysis patient diagnosed by muscle biopsy. J Clin Neuromuscul Dis 2014;15(3):108-111. [ Links ]
18. Moe SM, Drüeke TB, Block GA, et al. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl 2009;76(Suppl 113):S1-130. [ Links ]
19. Rivera F, López FG. ¿Cuáles son los beneficios y peligros de los calcimiméticos en el tratamiento del hiperparatiroidismo secundario en la insuficiencia renal crónica? Nefrología 2007;27 Supl 5 [ Links ]
20. Nigwekar SU, Brunelli SM, Meade D, Wang W, Hymes J, Lacson E Jr. Sodium thios ulfate therapy for calcific uremic arteriolopathy. Clin J Am Soc Nephrol 2013;8(7):1162-1170. [ Links ]
21. Baldwin C, Farah M, Leung M, et al. Multi-intervention management of calciphylaxis: a report of 7 cases. Am J Kidney Dis 2011;58(6):988-991. [ Links ]
22. Hackett BC, McAleer MA, Sheehan G, Powell FC, ODonnell BF. Calciphylaxis in a patient with normal renal function: response to treatment with sodium thiosulfate. Clin Exp Dermatol 2009;34(1):39-42. [ Links ]
23. Araya CE, Fennell RS, Neiberger RE, Dharnidharka VR. Sodium thiosulfate treatment for calcific uremic arteriolopathy in children and young adults. Clin J Am Soc Nephrol 2006;1(6):1161-1166. [ Links ]
24. Cicone JS, Petronis JB, Embert CD, Spector DA. Successful treatment of calciphylaxis with intravenous sodium thiosulfate. Am J Kidney Dis 2004;43(6):1104-1108. [ Links ]
25. Brucculeri M, Cheigh J, Bauer G, Serur D. Long-term intravenous sodium thiosulfate in the treatment of a patient with calciphylaxis. Semin Dial 2005;18(5):431-434. [ Links ]
26. Guerra G, Shah RC, Ross EA. Rapid resolution of calciphylaxis with intravenous sodium thiosulfate and continuous venovenous haemofiltration using low calcium replacement fluid: case report. Nephrol Dial Transplant 2005;20(6):1260-1262. [ Links ]
Dr. Emanuel Ferreira
Department of Nephrology, Centro Hospitalar e Universitário de Coimbra – Hospital Geral
Quinta dos Vales, S. Martinho do Bispo, 3041-853 Coimbra, Portugal.
E-mail: emanuelfeferreira@gmail.com
Conflicts of interest statement: None declared.
Received for publication: 19/07/2014
Accepted in revised form: 30/11/2014


{kind=link}
{kind=link}