










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.29 no.4 Lisboa dez. 2015
REVIEW ARTICLE
Focus on: II – Imaging in vascular access for haemodialysis
Pedro Filipe Sousa1, Joana Ferreira2, Rui Ramos1, Monica Fructuoso3
1 Radiology Department, Centro Hospitalar de Trás -os -Montes e Alto Douro, Vila Real, Portugal
2 Angiology and Vascular Surgery Department, Centro Hospitalar de Trás-os-Montes e Alto Douro, Vila Real, Portugal
3 Nephrology Department, Centro Hospitalar de Trás -os -Montes e Alto Douro, Vila Real, Portugal.
ABSTRACT
A reliable vascular access is essential to effective haemodialysis. Imaging evaluation of vascular access for haemodialysis includes preoperative assessment of vascular anatomy and post-operative surveillance for access maturation, as well as diagnosis in vascular access dysfunction. This article reviews the current diagnostic imaging methods in haemodialysis fistulas. Ultrasound is the technique of first choice when imaging vascular accesses. Digital subtraction angiography is superior for the assessment of the central veins and makes diagnosis and treatment possible in the same session.
Key -Words: Computed tomography; digital subtraction angiography; magnetic resonance; ultrasound; vascular access for haemodialysis.
RESUMO
Um acesso vascular adequado é essencial para o tratamento dialítico eficaz. A avaliação imagiológica do acesso vascular para hemodiálise inclui avaliação pré-operatória da anatomia vascular e vigilância pós-operatória da maturação de acesso, bem como o diagnóstico de disfunção acesso vascular. Este artigo é uma revisão sobre os métodos de diagnóstico por imagem nas fístulas de hemodiálise. A ecografia é a técnica de primeira escolha no estudo imagiológico dos acessos vasculares. Angiografia é superior na avaliação das veias centrais e possibilita o diagnóstico e o tratamento na mesma sessão.
Palavras-Chave: Acesso vascular para hemodiálise; angiografia; ecografia; ressonância magnética; tomografia computorizada.
INTRODUCTION
Portugal has been characterized by the highest incidence and prevalence of end -stage renal disease (ESRD) treated by dialysis or kidney transplantation in the European Union1. A reliable vascular access is essential to effective haemodialysis (HD). The main goal of a vascular access team is to preserve arteriovenous fistulas long-term function and to avoid the use of dialysis catheters, which are associated with a higher mortality2.
The most common complications in dysfunctional arteriovenous fistulas (AVF) are stenosis of the vascular access vessels, thrombosis and steal syndrome3.
Vascular access thrombosis is generally related to stenosis and can occur as a segmental thrombosis or extensive thrombotic occlusion3. Dialysis patients can also develop central venous stenosis as a reaction to wall trauma associated with dialysis catheter and as a result of the arterialized flow conditions in the venous circulation4.
Imaging evaluation of vascular access for HD includes preoperative assessment of vascular anatomy and post-operative surveillance for access maturation as well as diagnosis in vascular access dysfunction.
In our centre, vascular accesses are managed in an interdisciplinary continuous cooperation between nephrologists, vascular surgeon and interventional radiologists.
This article reviews the current diagnostic imaging methods in haemodialysis fistulas.
ULTRASOUND
Ultrasound is widely available and non-invasive, and for these reasons is the most widely used vessel visualization method. As a cost -effective method, it allows assessment of vascular access maturity and diagnosis of complications5,6. It is portable, and radiation and iodinated contrast media free. Doppler ultrasound is a direct technique for assessment of flow in vascular accesses. However, this method is operator dependent and subject to errors caused by variations in cross -sectional area and the angle of insonation.
Duplex ultrasound is the preferred method for preoperative vascular mapping and it should be performed in all patients before placement of an access7. The ultrasound examination for dialysis access planning is designed to gather information about both the arterial system and the venous system8. A luminal diameter of 2.5mm or greater at the anastomosis point, absence of obstruction, a straight segment for cannulation, to be within 1 cm of the skin surface and to have continuity with the proximal central veins are venous requirements for AVF construction9. These criteria may differ for arteriovenous grafts (AVG) and among centres. In our institution we use a cut-off of 2mm for vein diameter.
In patients with persistent post-operative swelling, ultrasound may confirm extravasations and haematomas or purulent infiltrations, as well as stenosis of the venous outflow tract, in the latter case with known limitations for assessment of central veins.
Failure to mature should be evaluated by physical examination and, if needed, ultrasound5,7. If an adequate AVF is not clinically identified in the first 4 to 8 weeks after surgical access creation, an ultrasound examination can be performed to detect a correctable anatomical problem10. If no stenosis is identified, thresholds for venous diameter and blood flow may suggest whether the AVF is mature for haemodialysis. Fistulas are more likely to be useable when they meet the rule of 6s characteristics: flow greater than 600mL/min, diameter at least 0.6cm, no more than 0.6cm deep, and discernible margins7.
Ultrasound also allows the identification of large draining venous branches (competing veins), which may be surgically ligated to increase flow throughoutthe main draining vein to allow AVF maturation11.
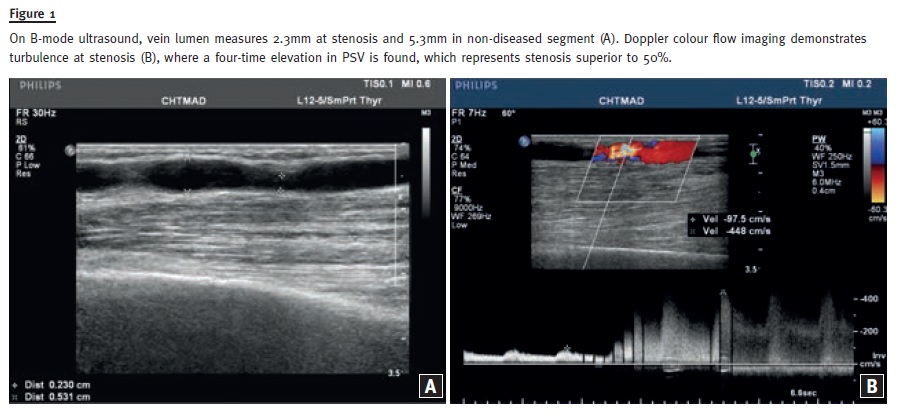
Ultrasound has become the primary imaging method in the case of vascular access dysfunction. Doppler ultrasound can provide anatomical assessment and direct evidence for the presence, location, and severity of access stenosis. Any visible narrowing of the draining vein on B-mode ultrasound or colour aliasing of flow within the vein should be further assessed with velocity measurements by spectral Doppler imaging10. Anastomosis luminal diameter inferior to 2mm or a Peak systolic velocity (PSV) ratio (anastomosis/artery 2cm upstream) greater than 3:1 has been suggested to represent a stenosis at anastomosis with diameter reduction greater than 50%12. A draining vein PSV ratio superior to 2:1 suggests stenosis superior to 50%13 (Fig. 1).
Ultrasound also allows the diagnosis of thrombotic occlusion. In any suspicion of steal syndrome clinical examination is mandatory, followed by ultrasound, as necessary. Central veins may be evaluated indirectly by using Doppler ultrasound14. However, angiography remains the standard for evaluating the central veins.
The benefit of duplex Doppler ultrasound on surveillance is controversial. The highest ultrasound surveillance benefit could be expected in AVGs and accesses with chronically lower flow15. Long-term follow-up via three-month duplex ultrasound can significantly extend the patency rate of dialysis vascular accesses16.
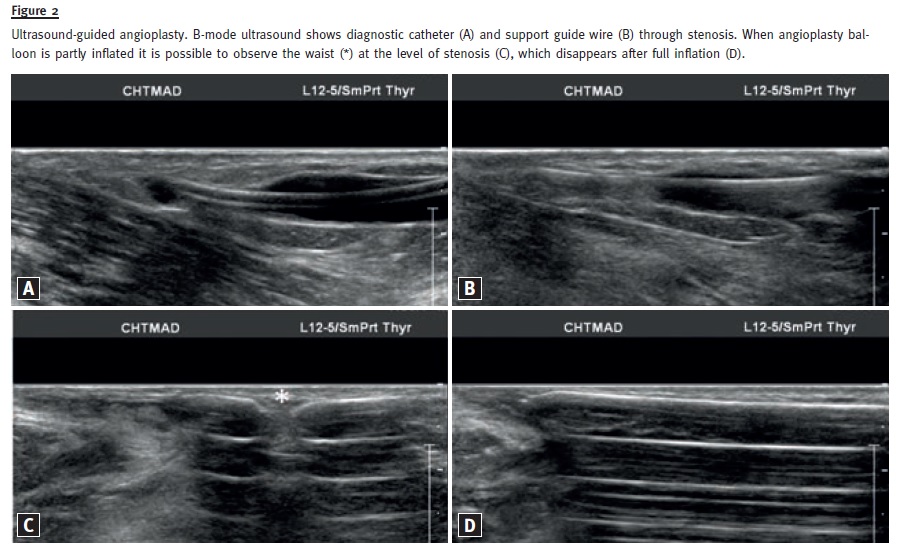
In our practice, we also use ultrasound during intervention, to select the adequate location to insert the introducer, to guide the puncture, particularly in immature AV fistulas or thrombosed vascular accesses, and to assist vessel angioplasty in patients not yet on haemodialysis (Fig. 2).
ANGIOGRAPHY
Digital subtraction angiography (DSA) is the gold standard for the evaluation of dialysis vascular access, and allows complete vessel visualization. A further advantage of this method is the possibility of treatment on the same session. However, DSA depends on ionizing radiation and contrast agents. Patients with renal disease or contrast allergy pose limitations on the use of iodinated contrast material (ICM). Alternative contrast media may be used in those patients.
Current alternatives are dilute ICM, carbon dioxide (CO2), and gadolinium17. Diluted ICM with a contrast volume of 10ml is safe and usually sufficient for diagnostic visualization18. In any suspicion of rupture during angioplasty in patients not yet on dialysis, under ultrasound guidance or CO2 angiography, we generally use a small amount (up to 10ml) of ICM to check AVF integrity. Carbon dioxide is a highly soluble, invisible gas. When injected into vessels, it briefly displaces the blood before it is rapidly dissolved and eliminated through exhalation19. CO2 is non -allergenic and non-nephrotoxic, making it safe for use in patients with either contrast allergy or kidney disease20. Although there is a known risk of neurotoxicity, central venography above the diaphragm is still permissible with CO221. If residual gas is seen between injections, the patient´s position should briefly be changed to move the CO2 bolus into a different vessel to allow dissolution22.
In our Institution, we use a system of three –way stopcock and a flow switch system. Special attention must be given to purging syringes of air and, once filled with CO2, not allowing valves to be left open.
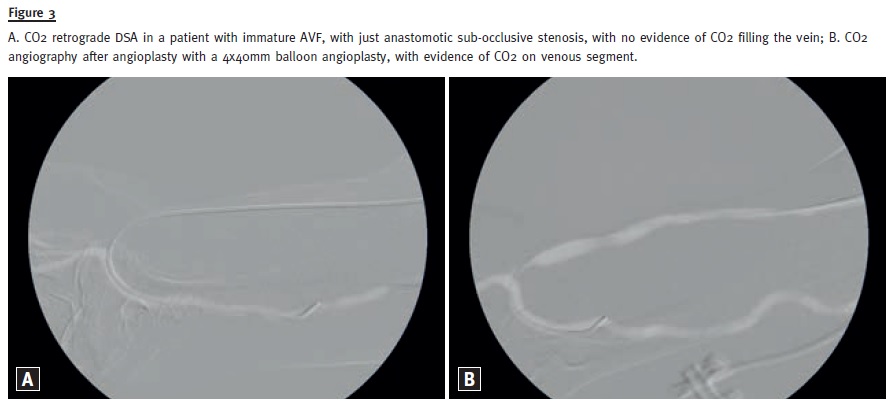
CO2 angiography represents an alternative to conventional DSA and is useful for the diagnosis and intervention of dysfunctional dialysis vascular access23 (Fig. 3).
The CO2 venography has a sensitivity of 97% and a specificity of 85% in the assessment of upper–limb and central vein patency and stenosis, compared to conventional venography24.
Gadolinium -enhanced DSA is also a further effective method for angiographic vessel visualization.
Since its association with nephrogenic systemic fibrosis (NSF) in 2006, its use as an angiographic agent in patients with CKD has appropriately declined rapidly (25 -27). The application of gadolinium as an ICM alternative for angiography is essentially limited to patients with normal renal function who have anaphylactic reaction to ICM.
Diagnostic DSA, without therapeutic intention, is not recommended, for reasons of radiation and invasiveness28.
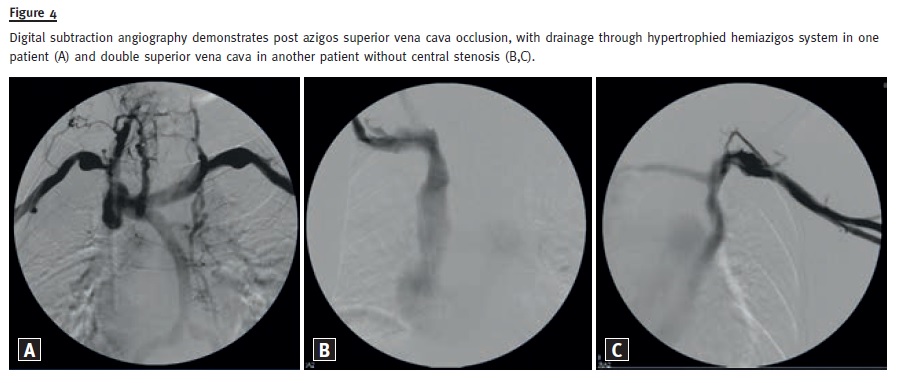
Digital subtraction angiography is the gold standard imaging method for the study of central veins (Fig. 4).
Preoperative imaging of the central veins should be performed in patients with a history of previous central venous catheters29.
Digital subtraction angiography is considered the gold standard for evaluating poor maturation of the fistula if the patient is already on dialysis therapy7, and allows evaluation of both arterial and venous segments of a dialysis vascular access.
Complete angiographic evaluation can be performed via retrograde arterial puncture of the brachial artery, near the elbow. It can also be done after antegrade puncture of the access vein, and in this case AV anastomosis can be visualized after proper compression of the draining vein with contrast medium reflux.
Finally, when looking for a more proximal arterial stenosis, it is possible to introduce the catheter through the anastomosis into the native portion of the arterial vessel after retrograde puncture of the access vein.
COMPUTED TOMOGRAPHY
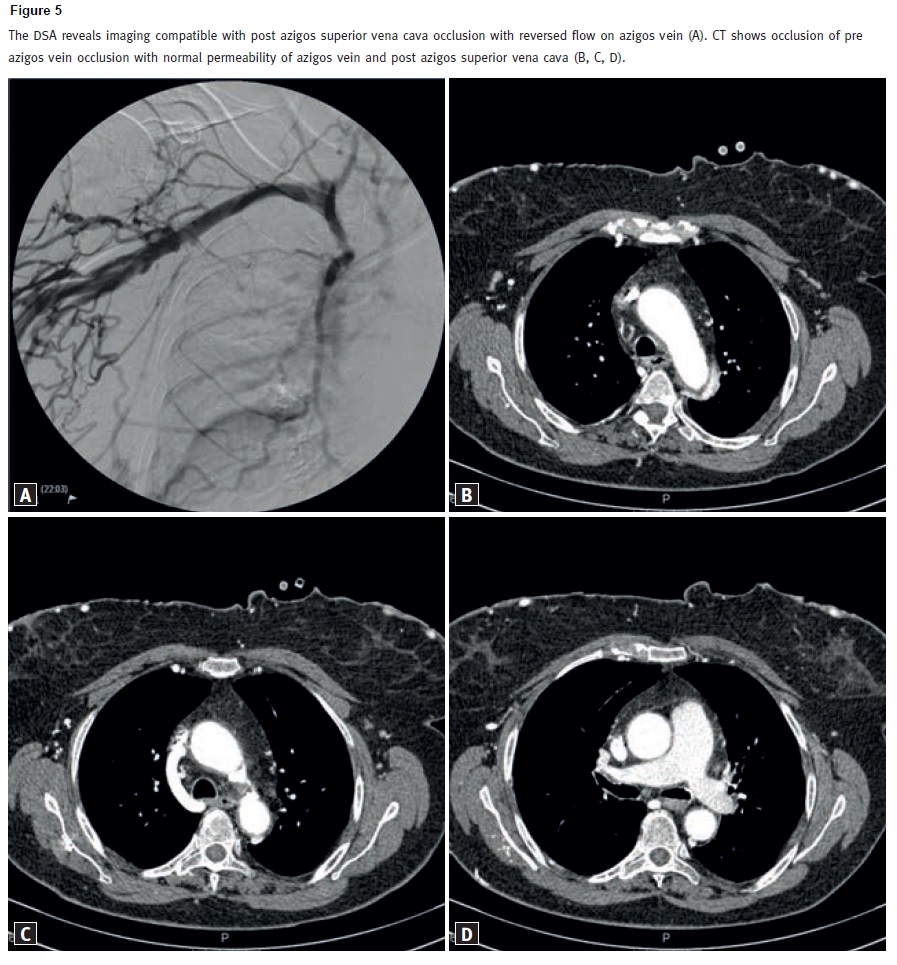
Computed tomography angiography (CTA) requires radiation exposure and iodine contrast administration. It is suitable for visualizing central veins and complete vascular tree in the case of an inconsistent sonographic finding. The CTA should only be used to clarify vascular access dysfunction if ultrasound and angiography yielded inconclusive findings (Fig. 5).
In particular, central venous thrombosis and paravascular soft tissues can be effectively detected with CT.
Computed tomography angiography is a non-invasive technique and may have economical benefits compared with purely diagnostic DSA30.
The CTA allows diagnosis of dysfunctional vascular access, as well as simultaneous visualization of the entire vascular tree31,32.
MAGNETIC RESONANCE
Magnetic resonance (MR) is radiation and ICM free. The presence of claustrophobia, pacemaker, and magnetized metal in patients are limitations in MR scanner. This is costly comparing to other imaging methods, particularly ultrasound.
Magnetic resonance angiography (MRA) provides anatomic assessment and direct evidence for the presence, location, and severity of access stenosis, and is particularly useful in central veins evaluation33.
Similarly to CTA, MRA is a valid alternative to purely DSA in the assessment of central veins.
However, for the reasons stated before about gadolinium, contrast enhanced MRA is no longer recommended in patients with CKD25-27.
There is promising data for the preoperative visualization of arterial and venous vascular structure by non-contrast MR angiography (MRA), but those techniques are not yet used in the clinical routine34.
CONCLUSION
Ultrasound is the technique of first choice when imaging vascular accesses. Digital subtraction angiography is superior for the assessment of the central veins and makes diagnosis and treatment possible in the same session. Computed tomography angiography should be reserved for patients with inconclusive ultrasound and DSA. Gadolinium–enhanced magnetic resonance imaging is no longer recommended in ESRD patients, because it may trigger nephrogenic systemic fibrosis, but there are promising results on non -contrast MR angiography.
References
1. OECD. Health at a Glance 2011: OECD indicators. [Online] 2011. [Cited: 30 Jan. 2012.] http://dx.doi.org/10.1787/health_glance-2011-en [ Links ]
2. Bray BD, Boyd J, Daly C, et al. with the Scottish Renal Registry. Vascular access type and risk of mortality in a national prospective cohort of haemodialysis patients. QJM 2012;105(11):1097 -1103. [ Links ]
3. Stolic R. Most important chronic complications of arteriovenous fistulas for hemodialysis. Med Princ Pract 2013;22(3):220-228. [ Links ]
4. Mansour M, Kamper L, Altenburg A, Haage P. Radiological central vein treatment in vascular access. J Vasc Access 2008;9(2):85-101. [ Links ]
5. Robbin ML, Chamberlain NE, Lockhart ME, et al. Hemodialysis arteriovenous fistula maturity: US evaluation. Radiology 2002;225(1):59-64. [ Links ]
6. Doelman C, Duijm LE, Liem YS, et al. Stenosis detection in failing hemodialysis access fistulas and grafts: comparison of color Doppler ultrasonography, contrast–enhanced magnetic resonance angiography, and digital subtraction angiography. J Vasc Surg 2005;42(4):739-746. [ Links ]
7. National Kidney Foundation. KDOQI Clinical Practice Guidelines and Clinical Practice Recommendations for 2006 Updates: Hemodialysis Adequacy, Peritoneal Dialysis Adequacy and Vascular Access. Am J Kidney Dis 2006;48(Suppl 1):S1-S322. [ Links ]
8. American Institute of Ultrasound in Medicine; American College of Radiology; Society of Radiologists in Ultrasound. AIUM practice guideline for the performance of ultrasound vascular mapping for preoperative planning of dialysis access. J Ultrasound Med 2012;31(1):173-181 [ Links ]
9. Shenoy S, Darcy M. Ultrasound as a tool for preoperative planning, monitoring, and interventions in dialysis arteriovenous access. AJR Am J Roentgenol 2013;201(4):W539-543. [ Links ]
10. American College of Radiology (ACR), Society of Radiologists in Ultrasound (SRU), American Institute of Ultrasound in Medicine (AIUM). AIUM practice guideline for the performance of a vascular ultrasound examination for postoperative assessment of dialysis access. J Ultrasound Med 2014;33(7):1321-1332. [ Links ]
11. Beathard GA, Settle SM, Sheilds MW. Salvage of the nonfunctioning arteriovenous fistula. Am J Kidney Dis 1999;33(5):910-916. [ Links ]
12. Lockhart ME, Robbin ML. Hemodialysis access ultrasound. Ultrasound Q 2001;17(3):157-167. [ Links ]
13. Robbin ML, Oser RF, Allon M, et al. Hemodialysis access graft stenosis: US detection. Radiology 1998;208(3):655-661. [ Links ]
14. Patel MC, Berman LH, Moss HA, McPherson SJ. Subclavian and internal jugular veins at Doppler US: Abnormal cardiac pulsatility and respiratory phasicity as a predictor of complete central occlusion. Radiology 1999;211(2):579-583. [ Links ]
15. Malik J, Kudlicka J, Novakova L, Adamec J, Malikova H, Kavan J. Surveillance of arteriovenous accesses with the use of duplex Doppler ultrasonography. J Vasc Access 2014;15(Suppl 7):S28-S32. [ Links ]
16. Malik J, Slavikova M, Svobodova J, Tuka V. Regular ultrasonographic screening significantly prolongs patency of PTFE grafts. Kidney Int 2005;67(4):1554 -1558. [ Links ]
17. Nadolski GJ, Stavropoulos SW. Contrast alternatives for iodinated contrast allergy and renal dysfunction: options and limitations. J Vasc Surg 2013;57(2):593 -598. [ Links ]
18. Asif A, Cherka G, Merrilll D, et al. Venous mapping using venography and the risk of radiocontrast -induced nephropathy. Semin Dial 2005;18(3):239 -242. [ Links ]
19. Huber PR, Leimbach ME, Lewis WL, Marshall JJ. CO2 angiography. Catheter Cardiovasc Interv 2002;55(3):398-403. [ Links ]
20. Hawkins IF, Cho KJ, Caridi JG. Carbon dioxide in angiography to reduce the risk of contrast-induced nephropathy. Radiol Clin North Am 2009;47(5):813-825. [ Links ]
21. Hawkins IF, Caridi JG. Carbon dioxide (CO2) digital subtraction angiography: 26-year experience at the University of Florida. Eur Radiol 1998;8(3):391-402. [ Links ]
22. Culp WC, McCowan TC, Goertzen TC, Habbe TG. Carbon dioxide angiography: complications and pseudocomplications. J Vasc Interv Radiol 1999;10(1):100-101. [ Links ]
23. Kariya S, Tanigawa N, Kojima H et al. Efficacy of carbon dioxide for diagnosis and intervention in patients with failing hemodialysis access. Acta Radiol Stockh Swed 2010;51:994-1001. [ Links ]
24. Heye S, Maleux G, Marchal GJ. Upper -extremity venography: CO2 versus iodinated contrast material. Radiology 2006;241(1):291-297. [ Links ]
25. Grobner T. Gadolinium – a specific trigger for the development of nephrogenic fibrosing dermopathy and nephrogenic systemic fibrosis? Nephrol Dial Transplant 2006;21(4):1104-1108. [ Links ]
26. Ergün I, Keven K, Uruç I, et al. The safety of gadolinium in patients with stage 3 and 4 renal failure. Nephrol Dial Transplant 2006;21(3):697 -700. [ Links ]
27. Prehal D, Holmes DT, Levin A. Nephrogenic systemic fibrosis: the story unfolds. Kidney Int 2008;73(12):1335-1337. [ Links ]
28. Tattersall J, Martin-Malo A, Pedrini L, et al. EBPG guideline on dialysis strategies. Nephrol Dial Transplant 2007;22(Suppl 2):ii5 -ii21. [ Links ]
29. Tordoir J, Canaud B, Haage P, et al. EBPG on vascular access. Nephrol Dial Transplant 2007;22(suppl 2):ii88-ii117. [ Links ]
30. Ye C, Mao Z, Rong S, et al. Multislice computed tomographic angiography in evaluating dysfunction of the vascular access in hemodialysis patients. Nephron Clin Pract 2006;104(2):c94-100. [ Links ]
31. Wasinrat J, Siriapisith T, Thamtorawat S et al. 64 -slice MDCT angiography of upper extremity in assessment of native hemodiaysis access. Vasc Endovascular Surg 2011;45(1):69-77. [ Links ]
32. Ko S -F, Huang C -C, Ng S -H, Tongdee T. MDCT angiography for evaluation of the complete vascular tree of hemodialysis fistulas. AJR Am J Roentgenol 2005;185(5):1268-1274. [ Links ]
33. Smits JH, Bos C, Elgersma OE, et al. Hemodialysis access imaging: comparison of flow -interrupted contrast -enhanced MR angiography and digital subtraction angiography. Radiology 2002;225(3):829-834. [ Links ]
34. Bode AS, Planken RN, Merkx MA, et al. Feasibility of noncontrast-enhanced magnetic resonance angiography for imaging upper extremity vasculature prior to vascular access creation. Eur J Vasc Endovasc Surg 2012;43(1):88-94. [ Links ]
Dr. Pedro Filipe Sousa
Radiology Department,
Centro Hospitalar de Trás -os -Montes e Alto Douro
Av. Noruega, Lordelo, 5000-508 Vila Real, Portugal.
E-mail: pedro.sousa@arsnorte.min-saude.pt
Conflict of interest statement: None declared.
Received for publication: 30/11/2015
Accepted:04/12/2015


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}