










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.30 no.3 Lisboa set. 2016
CASE REPORT
Hemodialysis Reliable Outflow (HeRO) Graft device: a lifesaving solution in multiple vascular access failure in haemodialysis patients
Miguel Bigotte Vieira*1, Tiago Ferreira*2, Alice Fortes1, Pedro Martins2, Augusto Ministro2, Hugo Ferreira3, Hugo Silva1, Tiago Amaral1, Cristina Resina1, Joana Gameiro1, Cristina Outerelo1, Estela Nogueira1, Sofia Jorge1, José Guerra1, José Fernandes e Fernandes2, António Gomes da Costa1
1Nephrology and Renal Transplantation Department, Hospital de Santa Maria, Centro Hospitalar Lisboa Norte, Portugal 2 Vascular Surgery Department, Hospital de Santa Maria, Centro Hospitalar Lisboa Norte, Portugal 3 Cardiothoracic Surgery Department, Hospital de Santa Maria, Centro Hospitalar Lisboa Norte, Portugal* Both authors contributed equally to this manuscript.
ABSTRACT
The increasing prevalence of end‑stage chronic kidney disease associated with advances in treatment is expected to lead to improved survival rates of chronic haemodialysis patients in Portugal. Establishing and maintaining vascular access patency is becoming a challenging issue in these patients. We present a case report of a multiple vascular access failure patient to whom a novel vascular access device was implanted which allowed successful haemodialysis, despite the presence of central venous stenosis and/or occlusion. To our knowledge the present case report describes the first utilization of Hemodialysis Reliable Outflow (HeRO) Graft device in Portugal. We present the case as well as a brief description of the device and available literature. This case report also underlines the importance of adopting a multidisciplinary approach in order to overcome complex and life‑threatening clinical challenges.
Key‑Words: multiple vascular access failure; central vein stenosis; Hemodialysis Reliable Outflow (HeRO) Graft; hemodialysis.
INTRODUCTION
The increasing prevalence of chronic kidney disease patients in Portugal has contributed to a higher incidence of haemodialysis in recent years1. Owing to medical research and treatment advances, haemodialysis patients, and in particular younger patients, are expected to present improved survival rates. Establishing and maintaining vascular access patency is a technically challenging issue in the management of these patients.
Multiple vascular access failure patients have exhausted peripheral venous access sites suitable for fistulas or grafts. These patients are treated with haemodialysis catheters as no other alternatives are available. Among vascular access options, catheters remain associated with higher rates of complications, notably bloodstream infections and catheter malfunction, subjecting end‑stage renal disease patients to more frequent hospitalizations, as well as higher morbidity and mortality2.
The utilization of percutaneous translumbar, transhepatic and direct right intra‑atrial catheters in multiple vascular access failure patients has been described3,4,5.
However, these techniques are last‑resort options to be used in this complex population.
We present a case report of a multiple vascular access failure patient who was treated with a novel vascular access device which allowed successful haemodialysis despite the presence of central venous stenosis.
The device became first available in the United States in 2008 after the FDA approved it for catheter‑dependent patients with central venous stenosis and/or occlusion6. There have been various descriptions of this device in the literature, but to our knowledge the present case report describes the first utilization of Hemodialysis Reliable Outflow (HeRO) Graft device in Portugal.
CASE REPORT
We present the case of a 46‑year‑old Angolan female patient with chronic kidney disease stage 5‑d of unknown aetiology. The patient was diagnosed with hypertension at age sixteen and had not received regular medical care. Comorbidities included inferior vena cava agenesis, hypertensive heart disease and retinopathy, obesity, dyslipidaemia, previous hysterectomy due to endometriosis, chronic venous insufficiency and right gonarthrosis.
An upper right arm arteriovenous fistula was created in 2006 and the patient started haemodialysis in 2007. Between 2007 and 2013 the patient presented several vascular access complications, concerning either tunneled haemodialysis catheter infections or arteriovenous grafts/fistula thrombosis and/or infections.
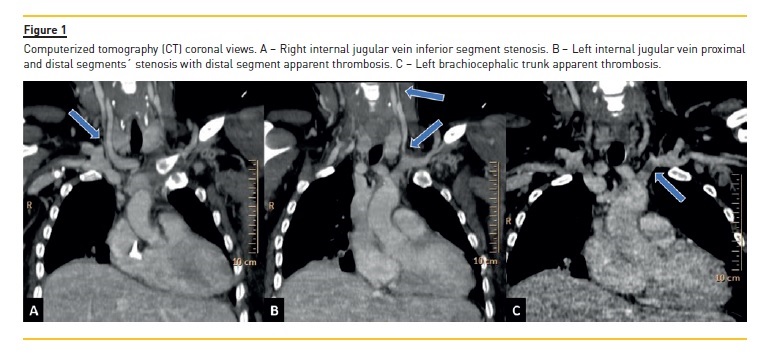
Considering this, the patient presented patency loss of the right and left Internal and external jugular veins, left brachiocephalic trunks, left subclavian vein (including a subclavian artery‑to‑contralateral subclavian vein necklace graft that thrombosed just a few weeks after surgery), left axillary vein and right femoral vein (Fig. 1).
Continuous ambulatory peritoneal dialysis had been carried out for 4 months during 2010 and was discontinued due to peritoneal dialysis catheter malfunction and two unsuccessful surgical revision attempts. The patient was considered for urgent kidney transplant in April 2014.
In July 2014 the patient underwent direct right intra‑atrial catheter placement using a right anterior minithoracotomy, which was revised two weeks later due to catheter exteriorization. In the seven following months, the patient presented successive catheter infections, leading to three hospital admissions. In February 2015 the patient presented another catheter exteriorization, which was replaced by median ministernotomy.
The patient was admitted in May 2015 due to a third episode of catheter exteriorization. This catheter was surgically replaced, requiring at this time a median sternotomy, but presented a deep wound infection and malfunction as procedure complications.
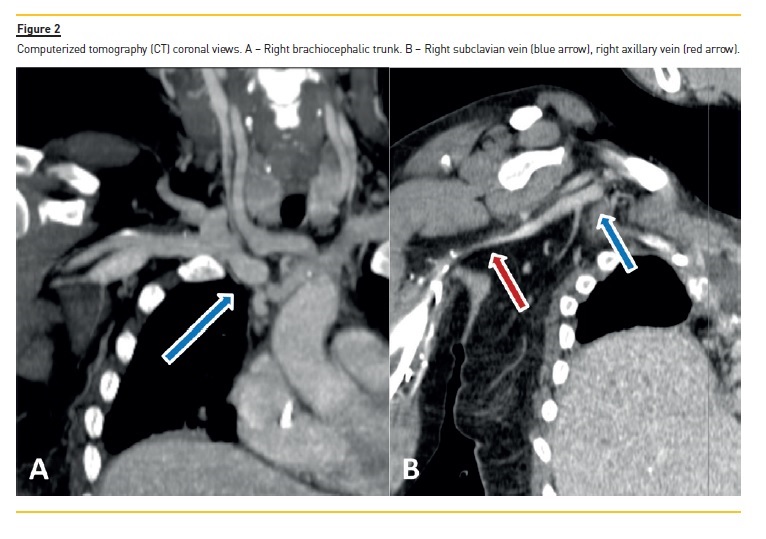
Although a whole‑body computerized tomography (CT) angiography revealed patent right subclavian and axillary veins (Fig. 2), it was not possible to place a catheter in this location after several attempts and therefore left femoral vein was considered as last vascular access site option. Although the implantation of a new catheter at this vein could theoretically jeopardize future kidney transplantation, taking into account the patient´s desperate clinical situation, a left femoral catheter was implanted. Peritoneal dialysis catheter implantation was also attempted without success due to multiple abdominopelvic adhesions. Considering the importance of maintaining femoral vascular patency to allow future renal transplantation, a multidisciplinary meeting involving the Nephrology and Vascular Surgery departments decided to use a Hemodialysis Reliable Outflow (HeRO) Graft. Blood cultures obtained before the procedure were negative.
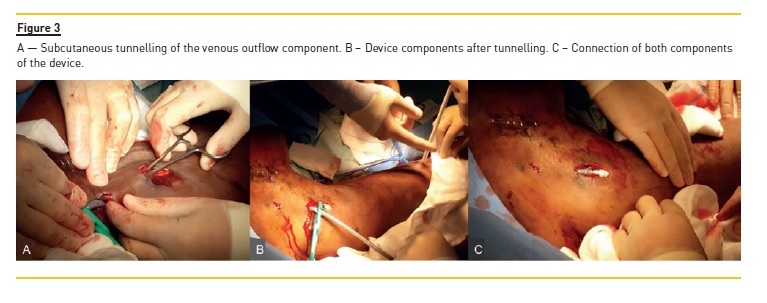
The device was implanted by a surgical team from the Vascular Surgery Department (Fig. 3). Under general anaesthesia, central venous access was obtained in the right subclavian vein by standard Seldinger technique.
A 0.035 hydrophilic guidewire was advanced into the inferior vena cava under fluoroscopic guidance. A pigtail catheter was used for exchange into a stiff Amplatz guidewire. A 20F introducer was inserted over the wire and the venous outflow component with its 10F delivery stylet was advanced up the introducer sheath under fluoroscopic guidance to confirm correct tip placement in the right atrium. The sheath was peeled off and the guidewire and delivery stylet removed. The venous outflow component was flushed with heparinized saline and clamped. A small incision was created in the deltopectoral groove for tunnelization of the venous outflow component. The right brachial artery was exposed and a tunneller was used to create a soft C‑shaped subcutaneous path between the incisions. The arterial graft component was tunnelled and the arterial anastomosis was constructed in standard fashion. After flushing, both components were then connected and unclamped.
Presence of a readily palpable thrill was verified and the incisions closed. The procedure took approximately 2 hours and no intraoperative or post‑procedural complications were noted. Antibiotic prophylaxis was not used as the patient was already under antibiotherapy with vancomycin and gentamicin for the thoracic wound infection.
The patient received a cadaveric kidney transplant one week after device implantation. Considering the presence of hyperkalaemia, the patient underwent a haemodialysis session before the transplantation surgical procedure. Due to femoral vein catheter malfunction, HeRO device was punctured once, one week after implantation, providing a medium blood flow rate of 300‑350 mL/min (within prespecified ranges) with regular vascular access site haemostasis and no immediate complications. After several months the HeRO device presents palpable pulse and soft continuous, diffuse thrill. The patient post‑transplant nadir creatinine was 1.8 mg/dL. Considering the risk of progression to end‑stage renal disease aggravated by the patients past history of treatment non‑adherence, it was decided to maintain the device in place for the first year after renal transplant.
DISCUSSION
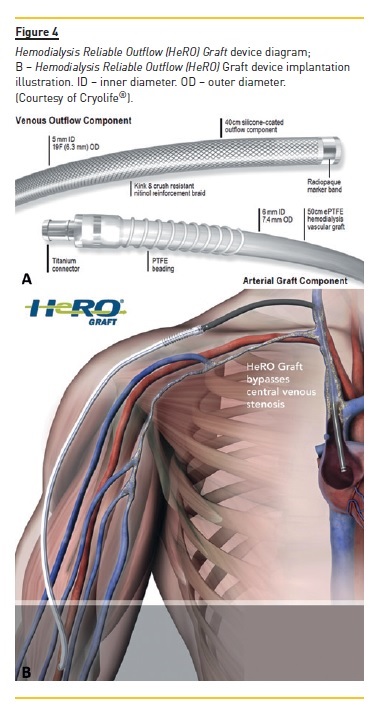
The Hemodialysis Reliable Outflow (HeRO) Graft device, available in Portugal since July 2015, is an access solution for chronic haemodialysis patients who have exhausted peripheral venous access sites suitable for fistulas or grafts (Fig. 4). The device is a fully subcutaneous surgical implant that bypasses central venous stenosis, providing hybrid arteriovenous (AV) access with continuous outflow into the central venous system.
It consists of two primary components; a standard polytetrafluoroethylene tube graft component and a nitinol‑reinforced silicone catheter outflow component.
The former can be used as a usual vascular graft while the latter allows dialyzed blood direct access into the right atrium.
The implantation procedure is undertaken under fluoroscopy guidance. Patients should be assessed for the existence of contraindications to device implantation, such as brachial or target artery inner diameter (ID) inferior to 3 mm; impracticability of internal jugular vein (IJV) or target vasculature dilatation to accommodate the 19F venous outflow component; significant arterial occlusive disease that would preclude safe placement of an upper extremity haemodialysis access; known or suspected allergy to device materials (i.e., polytetrafluoroethylene [ePTFE], silicone, titanium, nitinol); topical or subcutaneous infection associated with the implantation site and presence of known or suspected systemic infection, bacteraemia or septicaemia. To maintain adequate flow through the graft, the ejection fraction should be over 20% and the systolic blood pressure should be at least 100 mmHg. Blood cultures should be obtained before implantation to screen for asymptomatic bacteraemia.
It should be noted that during clinical trials, the device was implanted through the internal jugular vein and brachial artery. Considering this, central venous access through any other veins or implantation of the device into other arteries has not been studied and may increase the risk of adverse events.
Clinical Practice Guidelines for graft assessment, preparation and cannulation should be pursued, although a light tourniquet may be used for cannulation as the thrill and bruit may be softer than a conventional ePTFE graft due to absence of venous anastomosis.
The device requires equivalent maintenance to conventional ePTFE grafts such as percutaneous thrombectomy and has been determined to be magnetic resonance‑conditional.
Accordingly, the device has been demonstrated to pose no known hazards in a specified magnetic resonance imaging environment with specified conditions of use. As potential limitations, the HeRO device is costlier than AV grafts and the surgical procedure is more complex, requiring fluoroscopic guidance. Device removal requires a surgical procedure.
The HeRO device has been shown to have similar incidence of dysfunction and thrombosis compared with standard prosthetic AV grafts8. Noteworthy, the venous anastomosis and outflow veins of a prosthetic AV graft are the most frequent sites of stenosis, resulting in dysfunction and thrombosis, whereas the HeRO device is continuous to the right atrium, without a venous anastomosis.
A study describing 73 percutaneous interventions on 26 HeRO devices presented no or minor complications during or after procedures and one major complication after a procedure9. In this study, several HeRO devices demonstrated an apparent intra‑graft stenosis within 3 cm of the graft‑to‑catheter coupler. As needle access punctures are not performed at that site, which is typically at the level of the shoulder, the authors consider that the actual nature and aetiology of such stenosis are uncertain. It was also found that 22% of the procedures were due to thrombosis without any stenosis or other causative aetiology which is unusual in conventional haemodialysis fistulas and grafts. Considering this, authors hypothesize that there might exist a predisposition to a higher rate of spontaneous thrombosis due to HeRO device design, notably the extended length of synthetic material (compared with conventional AV grafts) and a relatively increased outflow resistance (compared with the normal central venous system) given the length and diameter of the device outflow catheter. Theoretically the bimodular design and route across the shoulder could also potentially cause graft or catheter kinking. Owing to the HeRO device design, medical doctors that perform vascular interventions should be aware of the potentially substantial clot burden contained within a thrombosed HeRO device, which may have a higher pulmonary embolism risk if not addressed appropriately. Thrombus volume within the device has been estimated to be higher than conventional haemodialysis vascular access thrombus. Therefore, the risk of pulmonary embolism with endovascular thrombectomy should be weighed against the possibility of performing surgical thrombectomy9.
A review of this device including 164 HeRO implants has concluded that the device has proven superior to tunnelled haemodialysis catheters in terms of patency (48.8% versus 36% primary patency, 90.8% versus 37% secondary patency rates at 12 months), intervention (1.5 versus 5.8 intervention rate per year) and infection rates (0.14 versus 2.3 bacteraemia rate per 1000 days) when compared to the peer‑reviewed literature. In this study, the HeRO device primary and secondary patency rates were superior (48.8% versus 42% primary patency; 90.8% versus 65% secondary patency rates at 12 months) while intervention rates were lower (1.5 versus 1.6‑2.4 intervention rate per year) than AVG historical controls.
The authors sustain that this device could also reduce the morbidity, mortality and costs associated with catheter‑related infections and interventions as it constitutes an alternative to catheter dependency6.
A randomized clinical trial enrolled and assigned 72 patients either to HeRO or conventional AV control grafts. Patients that received the device presented patency, adequacy of dialysis and bacteraemia rates comparable to those that received conventional AV grafts. However, due to slow enrolment and early termination, the study results were not sufficiently powered to answer the primary objective of demonstrating equivalent safety and efficacy between cohorts. In this study there was a tendency to higher intervention rates within the HeRO cohort compared to the AV graft control group, but this did not reach statistical significance.
However, the HeRO Graft cohort maintained secondary patency for nearly twice as long as the control group.
This difference was statistically significant. The authors postulate that this difference might be attributed to the absence of a venous anastomosis when the device is implanted. In conventional AV grafts venous anastomosis is associated with venous hyperplasia. Notwithstanding this possible advantage, it should be noted that HeRO device may fail like conventional AV grafts, notably due to inadequate arterial inflow, hypotensive episodes, patient hypercoagulability and steal syndrome10. These findings were consistent with results from other studies8.
A recent review of previous studies including 409 patients concluded that although this device presents a low primary patency, it presents acceptable secondary patency rates following intervention (one‑year primary and secondary patency rates of 21.9% (9.6‑37.2%) and 59.4% (39.4‑78%), respectively). It is also stated that the number of bacteraemia episodes is significantly lower with the HeRO device than either tunnelled or non‑tunnelled catheters (device‑related bacteraemia rate and catheter‑related bacteraemia rate per 1000 days between 0.13 and 0.7 and between 0.6 and 6.5 respectively).
Due to device availability, most results are from patients in the United States. Therefore, the authors highlight that data from other populations is required11.
Inferior vena cava agenesis has been described as a rare congenital abnormality associated with deep vein thrombosis in young people7. We consider that this comorbidity may partially explain this patients successive vascular thrombosis and probably contributed to multiple vascular access failure.
CONCLUSION
The HeRO graft device constitutes an alternative access option for complex haemodialysis patients with multiple vascular access failure, notably central vein stenosis and/or occlusion. These patients are expected to increase in number with the improved survival of haemodialysis patients. The device has already been used before in a considerable number of patients, mainly in the USA, with encouraging results. According to the literature, the device presents similar mechanical complications and bacteraemia rates to vascular grafts.
In light of this, we consider that it is an alternative in the subgroup of patients that have exhausted other vascular access options, benefiting patients and their families. This case report also highlights the vital importance of adopting a multidisciplinary approach in order to overcome challenging clinical scenarios.
References
1. Departamento de Gestão e Financiamento de Prestações de Saúde. Relatório de acompanhamento de actividade – Hemodiálise 2011‑2013. Administração Central do Sistema de Saúde, 2013 [ Links ]
2. NKF KDOQI GUIDELINES. Clinical Practice Guidelines and Clinical Practice Recommendations 2006 Updates. Vascular Access. Accessible on http://www2.kidney.org/professionals/KDOQI/guideline_upHD_PD_VA/va_wg.htm [ Links ] Motta‑leal‑filho JM, Carnevale FC, Nasser F, Oliveira W De, Junior S. Percutaneous transhepatic venous access for hemodialysis: an alternative route for patients with end‑stage renal failure. J Vasc Brasil 2010; 9(3):131‑136 [ Links ]
4. Oguz E, Ozturk P, Erkul S, Calkavur T. Right intra‑atrial catheter placement for hemodialysis in patients with multiple venous failure. Hemodial Int. 2012;16(2):306–309. [ Links ]
5. Biswal R, Nosher JL, Siegel RL, Bodner LJ. Translumbar placement of paired hemodialysis catheters (Tesio catheters) and follow‑up in 10 patients. Cardiovasc Intervent Radiol 2000;23(1):75–78. [ Links ]
6. Gage SM, Katzman HE, Ross JR, Hohmann SE, Sharpe CA, Butterly DW, et al. Multi‑center experience of 164 consecutive hemodialysis reliable outflow [HeRO] graft implants for hemodialysis treatment. Eur J Vasc Endovasc Surg. 2012;44(1):93–99. [ Links ]
7. Lambert M, Marboeuf P, Midulla M, Trillot N, Beregi J‑P, Mounier‑Vehier C, et al. Inferior vena cava agenesis and deep vein thrombosis: 10 patients and review of the literature. Vasc Med. 2010;15(6):451–459. [ Links ]
8. Katzman HE, McLafferty RB, Ross JR, Glickman MH, Peden EK, Lawson JH. Initial experience and outcome of a new hemodialysis access device for catheter‑dependent patients. J Vasc Surg. 2009;50(3):600–7.e1. [ Links ]
9. Gebhard., Bryant J A, Adam Grezaffi J, Pabon‑Ramos WM, Gage SM, Miller MJ, et al. Percutaneous interventions on the hemodialysis reliable outflow vascular access device. J Vasc Interv Radiol. 2013;24(4):543–549.
10. Nassar GM, Glickman MH, Mclafferty RB, Kevin Croston J, Zarge JI, Katzman HE, et al. A comparison between the HeRO graft and conventional arteriovenous grafts in hemodialysis patients. Semin Dial. 2014;27(3):310–318. [ Links ] [ Links ]
Dr. Miguel Bigotte Vieira
Nephrology and Renal Transplantation Department
Hospital de Santa Maria, Centro Hospitalar Lisboa Norte
Av. Prof. Egas Moniz, 1649‑035 Lisboa, Portugal
E‑mail: mbigottevieira@gmail.com
Conflict of interest statement: None declared
Acknowledgements
The authors thank Rui Araújo for 3D and MIP image processing.
Received for publication: Nov 30, 2015
Accepted in revised form: July 15, 2016


{kind=link}
{kind=link}
{kind=link}
{kind=link}