










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.31 no.3 Lisboa set. 2017
ORIGINAL ARTICLE
Diagnosis and treatment of haemodialysis vascular access problems without iodinated contrast: a single-centre experience
Joana Francisca Rocha1, Mónica Fructuoso1, Pedro Filipe Sousa2, Joana Ferreira3, Rui Miguel Abreu1, Catarina Eusébio1, Teresa Morgado1
1Nephrology Department, Centro Hospitalar de Trás-os-Montes e Alto Douro
2 Radiology Unit, Centro Hospitalar de Trás-os-Montes e Alto Douro
3 Angiology and Vascular Surgery Department; Centro Hospitalar de Trás-os-Montes e Alto Douro
ABSTRACT
Introduction: The use of iodinated contrast angiography in the diagnostic and therapeutic approach to arteriovenous access (AVA) problems is limited by nephrotoxicity and allergic reactions. The use of alternatives such as CO2 or ultrasound guidance has increased over the last few decades.
Purpose: To evaluate the results and complications of the diagnostic and therapeutic procedures of AVA performed at our centre without the use of iodinated contrast.
Methods: We evaluated retrospectively all patients submitted to endovascular diagnostic and/or therapeutic procedures using CO2 or ultrasound at our hospital between January 2013 and December 2016.
Results: 30 procedures were performed in 22 patients: 15 ultrasound-guided angioplasties and 15 CO2 procedures (14 angioplasties and 1 diagnostic angiography). The mean age of patients was 74±10 years (41–-94). Most procedures (90%) were performed on proximal arteriovenous fistulas (AVFs) and 3 were performed on distal AVFs. Iodinated contrast was not used because of its potential nephrotoxicity. Ultrasound-guided angioplasty was performed to treat outflow stenoses in the majority (73%) of the cases. The result was favourable in all procedures. One was complicated by venous rupture. Regarding angioplasties with CO2, outflow stenoses were the most treated (38%). The result was favourable in all procedures. Diagnostic angiography with CO2 was performed in a patient with signs of limb venous hypertension and was inconclusive. There were two complications in CO2 procedures: formation of pseudoaneurysm at the place of insertion of the introducer (n=1) and transient headache and nausea (n=1). Three of the patients who underwent angioplasty with CO2 and one patient who underwent ultrasound-guided procedure were submitted to balloon-assisted maturation.
Conclusion: In our experience, the use of alternative methods with no iodinated contrast (CO2/ultrasound) in the evaluation and treatment of vascular access problems in patients with renal dysfunction is effective and safe.
Key words: Angiography, carbon dioxide, haemodialysis vascular access, ultrasound guided
INTRODUCTION
Of all the types of vascular access, arteriovenous fistula (AVF) has higher patency rates, lower infection rates and lower overall costs1,2. The rate of complications related to vascular access rises significantly once it fails and, therefore, it is important to implement surveillance programmes in order to diagnose and correct vascular access problems within an adequate period of time.However, the reality is that a large proportion of incident patients start haemodialysis with other types of access.
Many factors contribute to this, including concerns over the use of iodinated contrast to evaluate and treat arteriovenous fistula problems in pre-dialytic stages.
When planning an AVF, venography is frequently necessary to complement the study of upper-limb vessels.
The main indication is the evaluation of the central vein in high-risk patients for stenosis (patients with previous central venous catheters or with cardiac devices)3. Additionally, venography plays an important role in the evaluation of obese patients and in those with previous failed AVFs. Despite the protocols for iodinated contrast nephrotoxicity prophylaxis and the development of low and iso-osmolar iodinated contrast products, patients with chronic kidney disease remain at a high risk of contrast-induced nephropathy4,5. Moreover, the allergic potential of this material is not negligible, even when anti-allergic medication is given6.
For many decades, carbon dioxide (CO2) and ultrasound have been used as alternatives to iodinated contrast for evaluating haemodialysis vascular accesses in patients in whom iodinated contrast agents are not advisable7-10.
PURPOSE
To evaluate the efficacy and complications of CO2 and ultrasound-guided procedures performed in our centre to diagnose and treat arteriovenous vascular accesses.
METHODS
Patient Population
We performed a retrospective analysis of all patients who underwent angiography and/or angioplasty with CO2 or ultrasound guided at our centre between January 2013 and December 2016.
Procedures description
The vascular access problem was previously identified in our Vascular Access Clinic, where all patients are routinely observed via complete physical examination and ultrasound. All procedures were performed by the same interventional radiologist and vascular surgeon, under local anaesthesia and light sedation, in an outpatient setting.
Ultrasound-guided procedures
Ultrasound apparatus
A Philips CX50 portable ultrasound (Philips Medical Systems, Bothell, WA) is used.
Ultrasound-guided procedure
All sheaths are inserted under ultrasound guidance through direct vascular access puncture at least 5 cm away from the most proximal stenosis. When possible, the access site is selected proximal to the stenosis to use high arteriovenous access blood flow to facilitate wire manipulation.
When this could not be done, stenoses were treated in a retrograde fashion (accessed via distal puncture).
Two access sheaths were rarely required to address venous and arterial stenoses. Guidewire and catheter navigation were performed under fluoroscopy guidance without intravenous iodinate contrast. Balloon size, position and inflation were guided by ultrasound only.
The success of the technique was measured based on three parameters: (1) clinical evaluation with physical examination, (2) final imaging result and (3) post-procedure access flow. Unfortunately, this last piece of information could not be obtained due to absence of registration in the intervention room.
CO2 procedures
CO2 infusion apparatus
A disposable aluminium cylinder containing 99.9% pure CO2 from Gasin® is connected to a laparoscopic gear (Strykers® 45 L PneumoSure®). In the connecting tube between the laparoscopic tower and a 50 mL syringe there is a 0.22 ųm (Bausch + Lomb®) filter. The syringe is connected to the tube and to the diagnostic catheter with a 3-way stopcock fixed together in line. All injections are performed manually. The cylinder should not be directly connected to the diagnostic catheter because a huge volume of CO2 under high pressure should not be delivered. As CO2 is a compressible gas and its volume is inversely proportional to the pressure, we use a laparoscopic tower to determine a constant pressure of CO2 and consequently a constant volume. According to the literature, the pressure should be 15 mmHg because at this pressure, the volume of CO2 in the syringe will be equal to its capacity. The syringe capacity chosen was 50 mL because the volume of CO2 administered should be between 40–60 mL to prevent explosive delivery, which would result in rapid vessel distension, with consequent pain and poor image quality. The filter is used to remove any particle or bacteria. The syringe is connected to the diagnostic catheter and to the connecting tube with a three-way stopcock fixed together in line. This arrangement in a closed system allows us to remove the residual contaminant air present in the system (the gas is purged three or four times) without disconnecting the syringe, avoiding in this way room air contamination.
As recommended by several authors, the fluid present in the diagnostic catheter is cleared with injection of 3 to 5 mL of CO2, to decrease the risk of explosive delivery. Moreover, to minimize this complication, the diagnostic CO2 hand injection should be performed slowly, uniformly and with lower pressure. CO2 injections should be separated between 2–3 minutes.
Venography Procedure
The arm is positioned in supination and in slight abduction to prevent anatomically pseudostenosis images in the axillary region. After puncture of the vein and placement of an introducer sheath, 10 ml of CO2 is injected to accustom the patient to the sensation.
The injected volume of CO2 varies between 10 and 30 mL for the upper-extremity veins and between 30–50mL for the central veins. When is intended to evaluate the anastomotic region, a diagnostic catheter is inserted into the artery. Ultrasonography was not used during the interventional procedure and, therefore, the success of the technique was measured based on physical examination and final imaging result.
Images were performed using digital subtraction technique. Acquisition rate was five frames per second.
RESULTS
Thirty procedures were performed in 22 patients: 15 ultrasound-guided angioplasties and 15 CO2 procedures (14 angioplasties and 1 diagnostic angiography). Mean age at the time of the procedure was 74±10 years (41–94).
Iodinated contrast was not selected because of its potential nephrotoxicity since all patients were in the pre-dialytic stage and one was a renal transplant recipient [glomerular filtration rate of 15±5ml/min (7–22)].
Ultrasound-guided procedures
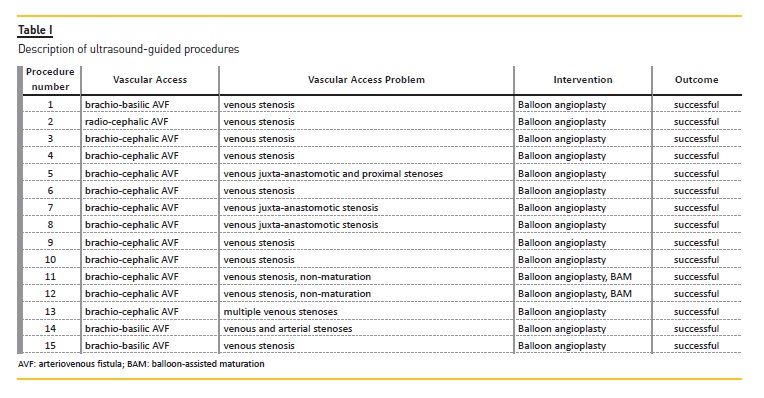
Table I gives detailed information about the ultrasound-guided procedures.
These were performed in 14 proximal arteriovenous fistulas (11 brachio-cephalic and 3 brachio-basilic) and in 1 radio-cephalic. The median time between vascular access creation and angioplasty was 4.5 months.
Ultrasound-guided angioplasty was performed to treat isolated venous stenosis [(n=12), of which 2 were juxta-anastomotic], venous and arterial stenosis (n=1), juxta-anastomotic and proximal venous stenoses (n=1) and multiple venous stenoses (n=1). The immediate result was favourable in all procedures. One procedure was complicated by venous rupture, which was treated with minimal surgery (venorraphy) and access function was restored.
One patient was submitted to balloon-assisted maturation with progressive dilatation of the arterialized vein.
CO2 procedures
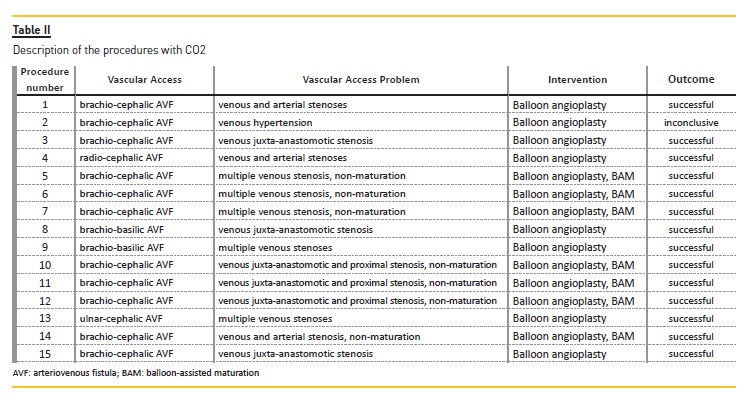
Table II contains detailed information about CO2- guided procedures.
Most procedures (n=12) were performed on proximal arteriovenous fistulas (10 brachio-cephalic and 2 brachio-basilic) and 2 were performed on distal AVFs (1 radio-cephalic and 1 ulnar-cephalic). The median time between vascular access construction and angioplasty was 3,3 months. Of the 13 angioplasties, 5 were performed for the treatment of multiple venous stenoses, 3 for venous and arterial stenosis, 3 for the treatment of juxta-anastomotic and proximal stenoses and 2 for the treatment of isolated juxta-anastomotic stenosis. The immediate result was favourable in all angioplasties.
Three of the patients underwent balloon-assisted maturation with progressive dilatation of the arterialized vein.
Diagnostic angiography was performed in a patient with signs of venous hypertension, but was inconclusive.
Among the 15 procedures, two complications occurred. One patient developed a pseudoaneurysm at the site of the introducer insertion that was surgically corrected. Other patient presented transitory headache and nausea. She presented a severe stenosis at the cephalic arch, which may have conditioned the reflux of CO2 to the arterial system. The brain CT performed to evaluate circulation was normal. The patient was kept under surveillance and the symptoms reverted spontaneously.
DISCUSSION
Many studies have proven the nephrotoxicity of iodinated contrast, even in patients with moderate renal function impairment, with dialysis precipitation5,11.
Moreover, the enormous importance of preserving residual renal function in patients on dialysis has led many health organizations to establish guidelines to avoid these agents even in that population.
Nowadays, the main alternatives for iodinated contrast to guide vascular access procedures are ultrasound and CO2. Our centre has been developing both techniques over the last 4 years and this retrospective review was conducted to evaluate our results regarding efficacy and safety and improve our practice.
Ultrasound-guided procedures
Over the last two decades, the safety and efficacy of endovascular procedures with ultrasound guidance have been established. The largest study of ultrasoundguided angioplasties (with 4869 cases) reported an early success rate of 97.1%12. In 2012, a review of 55 interventions reported an immediate success and 90-day patency of 93% with complications in 11% (n=6) of the cases13. In early 2017, a study comparing ultrasound-guided (n=53) with conventional angioplasties (n=90) registered equal success rates with same proportion of complications14. Other studies have corroborated these findings15,16.
In our experience, all vascular access angioplasties were effective when ultrasound was used to guide the procedure (100% success rate), allowing detection and treatment of different types of stenoses.
The benefits of ultrasound guidance for haemodialysis vascular access interventions are numerous.
Real-time visualization of stenoses makes possible real-time identification of the most advantageous access site and cannulation.
Since 1991 it has been suggested that ultrasound guidance identifies disease that may not be detected by conventional angiography and when adding ultrasound to classic angiography, the likelihood of detecting thrombus and dissection increases17,18. A single-centre randomized study with 100 patients showed that adding ultrasound to classic angiography in graft endovascular interventions was superior in the detection of stenosis than isolated conventional angiography19. The group showed that the procedure was shorter and the contrast material volume was reduced when using ultrasound guidance. Additionally, the addition of ultrasound altered the treatment considerably in 76% of the cases.
B-Mode duplex images of vein or graft wall are used to select proper diameter and length of balloon and stents, in order to prevent rupture while providing sufficient dilatation of stenoses.
Additionally, real-time monitoring of haemodynamic changes after balloon deflation allows immediate evaluation of treatment results.
Furthermore, as Marks and colleagues demonstrated, ultrasound guidance offers very important advantages of haemodynamic evaluation for recoiling lesions and need for stenting20.
Ultrasound is also useful in thromboaspiration since the catheter tip is visible and real time visualization makes it simpler to confirm aspiration of the thrombus16.
García-Medina prospectively studied 54 thrombosed native fistulae that underwent ultrasound-guided thrombolysis, with high success rates (83% in fistulas with total thrombosis and 100% in partial thrombosis)16.
Another undeniable benefit of ultrasound-guided procedures is the elimination of radiation exposure, making them more harmless for the patient and the health staff, doing away with the need for high doses of radiation that are required in conventional fluoroscopy procedures (due to magnification, multiple projections and quick dye washout inherent to this last technique).
It should be highlighted that the more patients are treated, the more important this advantage becomes.
Despite all the above-mentioned advantages, ultrasound guidance has some limitations, such as deep veins, cephalic arch stenosis and central stenosis evaluation21.
In fact, from our experience and as far as the literature describes, in these cases angiography with CO2 may be a more adequate alternative (see below).
Also very important is the need for more than 1 operator since more than two hands are required to perform the procedure. This is not a drawback in our hospital because, as in other centres, all procedures (including conventional angiography) are performed by two operators.
Another limitation is that this technique does not allow a panoramic view of the access, as fluoroscopy does. Moreover, finding collateral circulation is more complex. Additionally, ultrasound guidance requires high-resolution equipment due to the unique flow patterns such as very high velocities and major turbulence.
CO2 procedures
CO2 was first used in radiology to demonstrate retroperitoneal structures in 1914. After that, it was been used in evaluating many different structures, including the heart and infradiaphragmatic vessels7-9,22. Because of its low density, adequate imaging became much more reliable with the development of digital subtraction angiography in 1980 and since then the pioneer Hawkins group have used CO2 in more than 1400 patients23.
In 1994, Ehrman et al. documented that image quality of CO2 fistulography was sufficient for making therapeutic decisions even in patients undergoing routine venography (without clinical evidence of vascular access problems), after evaluating 32 procedures.
Kariya and co-workers performed interventional treatment in 141 vascular accesses (predominantly distal), including percutaneous transluminal angioplasty, thrombolysis, thrombectomy and stent placement24.
In this study, the authors reported that the immediate success rate was comparable to published data. Our experience is also favourable, since we were able to treat different types of stenosis with 100% success, despite the small number of cases.
However, the data about sensibility and specificity of CO2 have been controversial, with some studies showing that CO2 underestimates the stenosis grade and other publications demonstrating that this gas overestimates it25,26. Seventeen years ago it was demonstrated that CO2 yielded significantly larger vessel diameter compared with conventional angiography in an aortoiliac flow model27. This can be explained by the fact that CO2 is infused in an explosive way in vessels with elastic capacity, leading to an underestimation of the degree of stenosis. On the other hand, when using a tourniquet one should be aware that vasospasm may occur and that it may be resistant to vasodilative drugs, interfering with determination of the degree of stenosis . Moreover, CO2 is a gas and thus does not mix with blood, so the entire vessel must be filled with CO2 to avoid underestimation of the vessel diameter.
Sam Heye and colleagues compared venography with CO2 and iodinated contrast, using two independent observers with different amount of experience (3 and 9 years)28. They found a satisfactory interobserver agreement for patency/stenosis and stenosis grade.
Although the sample was small (22 patients) the sensitivity, specificity and accuracy of CO2 venography for all vein segments were 97%, 85% and 95%, respectively. In fact, for superior vena cava segments, CO2 was superior for evaluation than iodinated contrast, which could not depict these segments because of slow flow and significant motion artefacts. These problems can be prevented in most cases by performing an additional cannulation of a more proximal vein to shorten the distance between the contrast injection site and the central veins. However, even with this adaptation, these vein segments may not be assessable mainly because the venous flow remains too slow or the patients clinical condition is bad. In these patients CO2 is an attractive alternative, as demonstrated in numerous studies29.
Because CO2 does not mix with blood (unlike iodinated agents) venography with CO2 is more sensitive to detect small bleedings and collateral venous circulation.
Although other techniques that do not use iodinated agents have been developed (for example, ultrasound), CO2 venography is better in evaluating obese patients and when assisted balloon maturation is needed.
Moreover CO2 low viscosity permits injection between a guidewire and a catheter, obviating the necessity to remove the guidewire for contrast injections.
Although safety concerns limited its use in the beginning, improvements have been made and nowadays its safety has been demonstrated in several studies. In fact, CO2 can be injected for long, complex procedures.
Its high solubility (20x more than oxygen) means intravascular injection is safe, with air trapping only occurring if closed one-way valve systems are not used. This may occur if a 20cc syringe filled with CO2 remains open for 1h, when 68% of the volume is replaced by room air, since CO2 diffuses extremely and because of the concentration difference of CO2 in the syringe (99.5%) compared with the air (0.03%)23. CO2 can be safely used in patients with pulmonary chronic disorders as long as the time to body depuration of the gas is respected23.
Regarding renal safety, it was demonstrated that even after selective renal artery CO2 injection there are no renal changes, from a clinical and histopathological point of view (normal renal biopsies, including no endothelial injury on electronic microscopy)10,30.
Neurological symptoms are occasionally noted, when reflux of CO2 into the cerebral vessels (through arterial system) occurs, usually consisting of transient nausea or headache, as was the case with one of our patients24.
However, serious adverse effects rarely occur, with seizures or transient loss of conscience described in some reports24,25. These complications tend to occur early after procedure and are usually treated conservatively.
To the best of our knowledge, no permanent sequelae are reported in literature. The diagnosis of neurological complications relies on clinical suspicion. Brain CT scan can be performed to exclude other causes of neurological dysfunction and can rarely make the diagnosis when trapped gas is seen. Some manoeuvres have been proposed to avoid CO2 reflux. Kariya and colleagues used retrograde-fashion CO2 infusion under balloon occlusion, in order to prevent CO2 reflux to the vein24. Other authors have proposed arterial manual compress when infusing CO2 in the vein, essentially when the problem is near the anastomotic region and in severe stenosis that induce low blood flow. In fact, after that isolated case of a patient who developed potential neurological complication, we decided to use this technique when treating juxta-anastomotic region stenosis, to prevent CO2 reflux to the arterial system. Lastly, it should be noted that manual injection is inaccurate and the compressibility of CO2 results in an explosive injection, raising the risk of CO2 reflux. The use of a dedicated CO2 injector would overcome this undesirable effect (as well as improving the quality of venographies). In the absence of such a device, we developed a hand-delivery system, which incorporated principles learned from the dedicated injector.
Although endovascular treatment of isolated and non-complex stenoses is possible with the use of diluted contrast, in the treatment of multiple and/or complex stenoses, or when balloon-assisted maturation is indicated, patients would be exposed to a higher quantity of contrast and repeatedly. It is in these patients, as well as in patients with allergy, that these techniques represent a valuable alternative.
As discussed, CO2 and ultrasound guidance have many specific advantages and limitations and the choice between these two techniques depends on patient and clinical features. Ultrasound guidance is probably adequate in the majority of the patients; however, CO2 may be preferred in obese patients, in central veins or cephalic arch problems and when balloon-assisted maturation is required.
Although our immediate success rate was 100%, we are gathering more experience with these techniques to compare access patency after this type of intervention with the results of accesses undergoing conventional angiography. However, we believe that the results will be similar, as demonstrated in other series. This primary analysis was to establish the practical feasibility, immediate success, and safety of these techniques.
In our experience, even with the limitations of a small sample and a retrospective design, the use of CO2 and ultrasound to evaluate and treat arteriovenous vascular access problems in patients with renal dysfunction was effective and safe.
References
1. Ravani P, Palmer SC, Oliver MJ, et al. Associations between hemodialysis access type and clinical outcomes: a systematic review. J Am Soc Nephrol 2013;24:465-73. [ Links ]
2. Lacson E, Jr., Wang W, Lazarus JM, Hakim RM. Change in vascular access and mortality in maintenance hemodialysis patients. Am J Kidney Dis 2009;54:912-21. [ Links ]
3. Tordoir J, Canaud B, Haage P, et al. EBPG on Vascular Access. Nephrol Dial Transplant 2007;22(2):ii88-117. [ Links ]
4. Rundback JH, Nahl D, Yoo V. Contrast-induced nephropathy. J Vasc Surg 2011;54:575-9. [ Links ]
5. Kooiman J, Pasha SM, Zondag W, et al. Meta-analysis: serum creatinine changes following contrast enhanced CT imaging. Eur J Radiol 2012;81:2554-61. [ Links ]
6. Davenport MS, Cohan RH, Caoili EM, Ellis JH. Repeat contrast medium reactions in premedicated patients: frequency and severity. Radiology 2009;253:372-9. [ Links ]
7. Oliva VL, Denbow N, Therasse E, et al. Digital subtraction angiography of the abdominal aorta and lower extremities: carbon dioxide versus iodinated contrast material. J Vasc Interv Radiol 1999;10:723-31. [ Links ]
8. Diaz LP, Pabon IP, Garcia JA, de la Cal Lopez MA. Assessment of CO2 arteriography in arterial occlusive disease of the lower extremities. J Vasc Interv Radiol 2000;11:163-9. [ Links ]
9. Scalise F, Novelli E, Auguadro C, Casali V, Manfredi M, Zannoli R. Automated carbon dioxide digital angiography for lower-limb arterial disease evaluation: safety assessment and comparison with standard iodinated contrast media angiography. J Invasive Cardiol 2015;27:20-6. [ Links ]
10. Seeger JM, Self S, Harward TR, Flynn TC, Hawkins IF, Jr. Carbon dioxide gas as an arterial contrast agent. Ann Surg 1993;217:688-97; discussion 97-8. [ Links ]
11. Fahling M, Seeliger E, Patzak A, Persson PB. Understanding and preventing contrastinduced acute kidney injury. Nat Rev Nephrol 2017;13:169-80. [ Links ]
12. Wakabayashi M, Hanada S, Nakano H, Wakabayashi T. Ultrasound-guided endovascular treatment for vascular access malfunction: results in 4896 cases. J Vasc Access 2013;14:225-30. [ Links ]
13. Gorin DR, Perrino L, Potter DM, Ali TZ. Ultrasound-guided angioplasty of autogenous arteriovenous fistulas in the office setting. J Vasc Surg 2012;55:1701-5. [ Links ]
14. Cho S, Lee YJ, Kim SR. Clinical experience with ultrasound guided angioplasty for vascular access. Kidney Res Clin Pract 2017;36:79-85. [ Links ]
15. Ascher E, Hingorani A, Marks N. Duplex-guided balloon angioplasty of failing or nonmaturing arterio-venous fistulae for hemodialysis: a new office-based procedure. J Vasc Surg 2009;50:594-9. [ Links ]
16. Garcia-Medina J. Value of duplex ultrasound assistance for thromboaspiration and dilation of thrombosed native arterio-venous fistulae. Cardiovasc Intervent Radiol 2013;36:1658-63. [ Links ]
17. Davidson CJ, Newman GE, Sheikh KH, Kisslo K, Stack RS, Schwab SJ. Mechanisms of angioplasty in hemodialysis fistula stenoses evaluated by intravascular ultrasound. Kidney Int 1991;40:91-5. [ Links ]
18. Arbab-Zadeh A, Mehta RL, Ziegler TW, et al. Hemodialysis access assessment with intravascular ultrasound. Am J Kidney Dis 2002;39:813-23. [ Links ]
19. Ross JR, Franga DL, Gallichio M, Patel AJ, Ouriel K. Role of intravascular ultrasound imaging during endovascular interventions of failing hemodialysis access grafts. J Vasc Surg 2017;65:1383-9. [ Links ]
20. Marks N, Ascher E, Hingorani AP. Duplex-guided repair of failing or nonmaturing arteriovenous access for hemodialysis. Perspect Vasc Surg Endovasc Ther 2007;19:50-5. [ Links ]
21. Garcia-Medina J, Garcia-Alfonso JJ. Ultrasound-Guided Angioplasty of Dysfunctional Vascular Access for Haemodialysis. The Pros and Cons. Cardiovasc Intervent Radiol 2017;40:750-4. [ Links ]
22. Hallin RW. Carbodissection as an adjunct to endarterectomy. Am Surg 1967;33:542-5. [ Links ]
23. Hawkins IF, Caridi JG. Carbon dioxide (CO2) digital subtraction angiography: 26-year experience at the University of Florida. Eur Radiol 1998;8:391-402. [ Links ]
24. Kariya S, Tanigawa N, Kojima H, et al. Efficacy of carbon dioxide for diagnosis and intervention in patients with failing hemodialysis access. Acta Radiol 2010;51:994-1001. [ Links ]
25. Ehrman KO, Taber TE, Gaylord GM, Brown PB, Hage JP. Comparison of diagnostic accuracy with carbon dioxide versus iodinated contrast material in the imaging of hemodialysis access fistulas. J Vasc Interv Radiol 1994;5:771-5. [ Links ]
26. Black CM, Lang EV, Kusnick CA, et al. 1996 AUR Memorial Award. Densitometric analysis of eccentric vascular stenoses: comparison of CO2 and iodinated contrast media. Acad Radiol 1996;3:985-93. [ Links ]
27. Moresco KP, Patel N, Johnson MS, Trobridge D, Bergan KA, Lalka SG. Accuracy of CO2 angiography in vessel diameter assessment: a comparative study of CO2 versus iodinated contrast material in an aortoiliac flow model. J Vasc Interv Radiol 2000;11:437-44. [ Links ]
28. Heye S, Maleux G, Marchal GJ. Upper-extremity venography: CO2 versus iodinated contrast material. Radiology 2006;241:291-7. [ Links ]
29. Sullivan KL, Bonn J, Shapiro MJ, Gardiner GA. Venography with carbon dioxide as a contrast agent. Cardiovasc Intervent Radiol 1995;18:141-5. [ Links ]
30. Hawkins IF, Jr., Mladinich CR, Storm B, et al. Short-term effects of selective renal arterial carbon dioxide administration on the dog kidney. J Vasc Interv Radiol 1994;5:149-54. [ Links ]
Joana Rocha, MD
Serviço de Nefrologia do Centro Hospitalar de Trás-os-Montes e Alto Douro, Av. Noruega, 5000-508 Vila Real, Portugal.
E-mail: joanafvrocha@gmail.com
Disclosure of potential conflicts of interest: none declared
Authors Contributions: All authors made substantial contributions to the conception and design of the manuscript, were involved in revising it critically for important intellectual content, and gave final approval of the version to be submitted.
Received for publication: Sep 1, 2017
Accepted in revised form: Sep 22, 2017


{kind=link}
{kind=link}