










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.32 no.2 Lisboa jun. 2018
CASE REPORT
Tubulointerstitial nephritis and uveitis syndrome (TINU) – à propos of 2 cases
Ricardo A. Macau1, Sara Barreto1, Joana Martins1, Joana Silva1, Filipe Fraga2, Rita T Manso3, Pedro Bravo1, Aura Ramos1
1 Nephrology Department, Hospital Garcia de Orta, Almada
2 Ophtalmology Department, Hospital Garcia de Orta, Almada
3 Anatomic Pathology Department, Hospital Fernando da Fonseca, Amadora
ABSTRACT
The authors present two cases of tubulointerstitial nephritis and uveitis syndrome (TINU). TINU is a well-known yet rarely reported oculorenal inflammatory clinical entity. A high level of suspicion is needed to identify this entity. The first case is that of a 24-year-old female presenting with bilateral red eye and ocular pain. Laboratory investigation revealed renal insufficiency (serum creatinine 4.9mg/dL) and kidney biopsy presented tubulointerstitial nephritis. The second case is that of a 69-year-old female initially diagnosed with uveitis who later presented with general symptoms and renal insufficiency (serum creatinine 3.96 mg/dL) and whose kidney biopsy showed a tubulointerstitial nephritis pattern. Both patients were treated with steroids and renal function improved. It may be worth screening for uveitis in all patients with tubulointerstitial nephritis and evaluating renal function in those presenting with apparent idiopathic uveitis.
Key-Words: Immunosuppression, Interstitial nephritis, Steroids, Tubulointerstitial nephritis and uveitis, Uveitis.
BACKGROUND
Acute tubulointerstitial nephritis (ATIN) is an entity with growing incidence in clinical practice1,2, responsible for a significant percentage (15-27%) of cases of acute kidney injury (AKI) that undergo renal biopsy3,4.
It is an inflammatory process of the renal interstitium and tubules, sparing the glomeruli and vasculature. In addition to AKI, patients may present tubular dysfunction. In line with its etiology, ATIN can be broadly classified into 1) drug-induced (D-ATIN), 2) autoimmune/secondary to a systemic disease, or 3) due to other rare causes (such as infection, malignancy or metabolic disorder)4. Most studies suggest that drugs are implicated in the majority of biopsy-proven ATIN cases (70–90%), followed by autoimmune diseases, including Sjögren´s syndrome, IgG4-related disease, tubulointerstitial nephritis and uveitis syndrome (TINU) and sarcoidosis1,5. However, there is a possibility that some autoimmune-related ATIN are misclassified as D-ATIN when the renal diagnosis is made, due to the absence of systemic manifestations that can present later in the course of the disease4. Since the initial presentation may be misleading, a high level of suspicion and close follow-up are mandatory to correctly identify the underlying cause.
TINU is a well-known yet rarely reported6 oculorenal inflammatory condition in which patients may either be asymptomatic or they may refer nonspecific symptoms (fever, rash, arthralgia, malaise). Synchronous or non-synchronous uveitis (generally bilateral suddenonset anterior ocular inflammation) and renal disease coexist7. Since TINU represents a diagnosis of exclusion, ruling out other systemic disease that may explain both manifestations is essential. The underlying pathological process remains elusive but treatment with corticosteroids and other immunosuppressive agents seems effective. The authors describe two cases of TINU in different age groups, with different presentations but with similar outcome, while reviewing its epidemiology, pathophysiology, diagnostic criteria, treatment and prognosis.
CASE REPORTS
Case 1
A 24-year-old female patient, originally from Brazil and living in Portugal for the past 2 years, presented with mild fever (37.5-38 °C), chills, myalgia, fatigue and nausea. Symptoms started 2 months before admission, during a trip to Brazil. At that time, she was admitted to the emergency department and discharged with the diagnosis of a common cold.
She complained of general discomfort from that moment on. When she returned to Portugal, she presented to the emergency department with visual acuity reduction, red eye and ocular pain and was diagnosed with anterior uveitis. Topical therapy with dexamethasone, cyclopentolate and chloramphenicol was started, and a laboratory investigation of uveitis was performed in the ophthalmology outpatient clinic. She was referred to the emergency department due to serum creatinine elevation of 4.9 mg/dL and was then admitted to the nephrology ward. She had no relevant past medical history apart from tonsillitis during childhood and a self-reported allergy to penicillin. The patient was not under any habitual medication and she denied having taken other medicines besides intra-ocular ones and metamizol.
On admission she referred general indisposition and ocular pain. Diuresis was preserved and the patient denied any change in its pattern or aspect.
Signs of neurological impairment were absent and her vital signs were normal. Blood pressure was 110/73 mmHg, pulse 80 bpm regular; she was apyretic and peripheric oxygenation was normal as was respiratory rate. Clinical examination was unremarkable apart from bilateral red eye and pallor. She did not present any sign of hydrosaline overload.
Blood tests revealed normochromic normocytic anemia, with otherwise normal blood count. Her renal function was impaired (urea 49 mg/dL and creatinine 4.3 mg/dL). Ionogram values were normal, as was glucose, and hepatic or cytolysis markers. C-reactive protein was mildly elevated (1.77 mg/dL). Urinalysis showed proteinuria 100mg/dL, erythrocyturia 20/uL and glycosuria 300mg/dL. Urinary creatinine to protein ratio was 0.4. Beta-HCG was negative. Kidney ultra-sound showed normal aspect of both kidneys. Additional investigation was inconclusive including negative ANA, C3 and C4 levels, HIV, Hepatitis A, B and C markers, ASO reaction, ANCA, ECA, anti-GMB and serum electrophoresis. Brucelosis, Coxiella burnetii, Ricketsia conorii and Borrelia infections were excluded. There was past contact with toxoplasma and CMV (IgG positive with IgM negative).
Assuming uveitis (not responding to topical treatment) and possible interstitial nephritis she was started on prednisolone 1mg/kg – 60 mg and a kidney biopsy was performed.
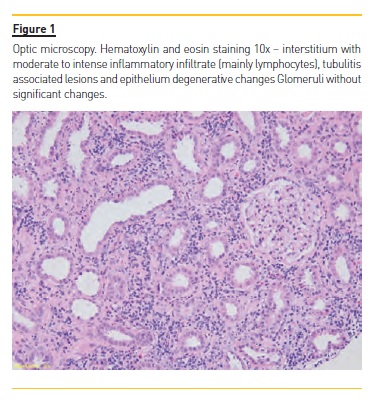
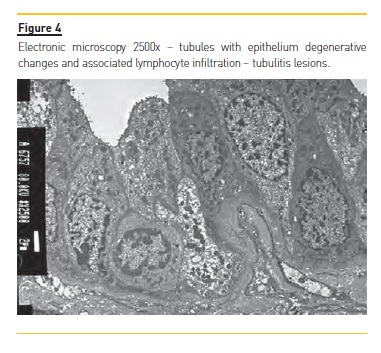
Kidney biopsy showed active chronic tubulointerstitial nephritis ( Figures 1 and 2) with no deposits on immunofluorescence and the diagnosis of TINU was assumed.
Patient evolution was favorable with regression of renal dysfunction under prednisolone treatment (slow tapering). She presented a creatinine of 1.3mg/dL and mild glycosuria and leukocyturia after 3 months of treatment.
Case 2
A 69-year-old woman, with a past history of sporadic consumption of NSAIDs and a 2-month diagnosed hypertension, medicated with an ACEi. Symptoms started 3 months previously, with 3 episodes of painful ocular inflammation (red eye). She consulted an ophthalmologist who confirmed the diagnosis of uveitis, and was medicated with topical steroids. One month later she went to her general practioner, complaining of malaise and anorexia. Blood analysis showed normocytic/normochromic anemia, erythrocyte sedimentation rate 82 seconds, urea 106 mg/dL, Cr 3.96 mg/dL and urinalysis with proteinuria (50 mg/dL) and glycosuria (100 mg/dL). She denied diabetes, hearing loss, arthralgia, photosensitivity or recent infections.
Even though the etiology of the renal disease was not known, she was started on systemic steroids referred to the nephrology outpatient clinic.
On our evaluation, blood analysis confirmed the normocytic and normochromic anemia (Hb 8.6 g/dL) and impaired kidney function (although improving) (Cr 2.8 mg/dL). Diabetes was excluded (HbA1c 5%). The remaining study was unremarkable with neither C3 nor C4 decreased levels and negative ANA, ANCA, ECA, anti-GMB. HIV, Hepatitis A, B and C markers were also negative, as well as ASO reaction. Electrophoresis of serum proteins was normal. Renal ultrasound showed no abnormalities.
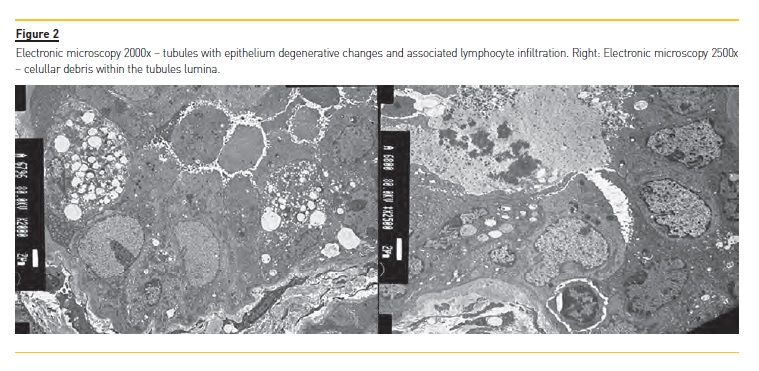
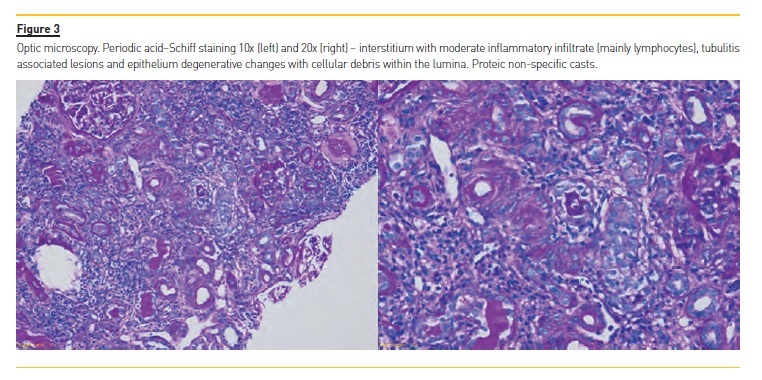
Kidney biopsy was then performed and showed chronic tubulointerstitial nephritis with active inflammatory infiltrate rich in lymphocytes and active tubulitis lesions, without deposits on immunofluorescence (Figures 3 and 4).
The diagnosis of TINU was assumed and she was started on prednisolone 1mg/kg.
On follow-up, the episodes of uveitis stopped and the authors verified an improvement of kidney function (Cr 2.8-> 1.9 mg/dL).
DISCUSSION
Epidemiology
TINU was first reported in 1975 by Dobrin et al8 and since then many cases have been described worldwide.
It is predominantly seen in younger age groups, with a slight preponderance in the female gender9. Most studies available included pediatric population; hence the reported median age of onset was 15–17 years old9,10. However, a French study encompassing older patients encountered a median age of presentation at around 47 years old11. Published data suggest an estimated incidence of 1–2 per 10 million population per year12, a prevalence of 3.5 cases per million13 and only 0.1–2% of patients attending specialized uveitis centers9,14; nonetheless its prevalence may be higher than currently recognized15. One prospective study in pediatric patients with biopsy-proven interstitial nephritis identified asymptomatic uveitis in 50% of cases16 so this entity might be underdiagnosed. TINU may account for 9 to 22% of all cases of ATIN in adults4. On the other hand, some uveitis labeled as idiopathic did not undergo further laboratory evaluation to rule out or confirm this entity15.
Our hospital serves a population of about 350,000 inhabitants and 2 cases of TINU were identified in the same year, which suggests that indeed its incidence may be higher than described. Both cases occurred in women, with an older age of onset than initially reported but in agreement with more recent series and case reports.
Diagnostic criteria
In 2001, Mandeville and colleagues9 proposed diagnostic criteria for this entity that include (1) occurrence of tubulointerstitial nephritis (TIN) and (2) uveitis (3) in the absence of other systemic diseases that cause either conditions. Therefore, TINU is considered a diagnosis of exclusion. The urine sediment may present red cells or red cell casts; tubular proteinuria may be detected and a proportion of patients exhibit sterile pyuria. Peripheral blood and urinary eosinophilia are inconsistent findings7. Elevated urinary β2-microglobulin was reported in about 87% of cases of TINU, and thus has been suggested as a sensitive and specific noninvasive diagnostic test. However, it is a marker of tubular injury of any etiology and not specific for TINU6,17,18. While the type of inflammatory cells infiltrating the renal interstitium are not included in the diagnostic criteria, Legendre et al observed a preponderance of lymphocytes (100% of cases) and plasmocytes (57%)11. Although initially defined as anterior, several reports showed a broad range of ocular manifestations (from posterior, intermediate and panuveitis)11,17,18. The relationship between clinically apparent tubulitis and uveitis is variable, with several series reporting different predominant sequence: uveitis may precede renal disease in 21–31% of the cases, may be concurrent with nephritis in 15 to 49% and can follow it in 20 to 65%9,11. Sarcoidosis, Sjögren´s syndrome, systemic lupus erythematosus, inflammatory bowel disease and tuberculosis are amongst the pathologies that should be ruled out6,9,10.
In both cases, the ocular manifestations were typical anterior bilateral uveitis. Tubulointerstitial nephritis was clinically suspected by the concomitant occurrence of renal dysfunction, altered urinalysis (with proteinuria, glycosuria and presence of red cells) and systemic symptoms, later confirmed histologically on kidney biopsy.
The interstitial infiltrate was mostly composed of lymphocytes.
In case 1, although laboratory evaluation was not initially performed, the authors suspect that nephritis was the presenting feature, based on the presence of systemic symptoms and morphological signs of chronicity in the biopsy specimen. In the second case, the patient had already experienced several episodes of idiopathic uveitis before renal dysfunction became apparent. Extensive serological evaluation was performed, excluding other possible causative systemic disorders.
Pathophysiology
Thus far, the precise pathophysiology of this syndrome remains to be determined2,6,18. Several etiologic factors have been identified, including susceptibility features and environment triggers19. Genetic susceptibility associated to various human leucocyte antigens (HLA) has been proposed – HLA-A220, HLA-A2420, HLA-DQA1*0121, HLA-DQB1*0521,22, HLA-DRB1*121,22 and HLA-DRB1*010223 – but small sample size and heterogeneity between reports preclude robust conclusions6.
Drugs such as non-steroidal anti-inflammatory agents (NSAID)24,25,26 and antibiotics25,26 were the main pharmacological groups associated with the occurrence of TINU. However, a causal relationship has not been proved; these are medicines commonly used in the general population that may simply coexist7 or patients may take them to treat the prodromal symptoms19.
Giving the prodromal flu-like symptoms, although with no localizing sign or positive microbial cultures, infectious agents were also considered to have a possible role as external triggers of TINU7,19.
It is thought to be an immune-mediated process (involving both humoral and cellular responses)19. Several findings point to a contribution of humoral immune mechanisms: reports describing the presence of circulating immune complexes27, transiently reduced C4 concentrations28, serum from patients with TINU reacting against both the eye and the kidney29,30, with a possible role for antimonomeric C-reactive protein antibodies31,32,33, antinuclear antibodies19,34, antineutrophil cytoplasmic antibody35 and anti-glomerular basement membrane antibody36. Cellular immune mechanisms are elicited by the presence of a predominantly lymphocytic and monocytic interstitial infiltrate and the association with HLA genotypes19. A possible model includes a microbial or chemical agent triggering an innate immune response, with production of cytokines and proinflammatory proteins, resulting in indiscriminate tissue damage and exposure of antigenic sites that elicit an autoimmune response. The triggering antigens associate with HLA peptides and interact with T-cell receptors, initiating the adaptive immune response in which antigen-specific T cells are stimulated to proliferate, differentiate, produce cytokines and exert direct cytotoxic effects to the uvea and renal interstitium19,37,38. Being a delayed-type hypersensitivity response, a period of 7–10 days is expected between exposure to the triggering agent and organ damage; a shorter period can be seen if preexposure has occurred39.
Indeed, a flu-like syndrome occurred in case 1 with evidence of organ damage recorded about 2 weeks later – in agreement with the model described above.
Treatment
Although comparative studies with control groups are lacking, current accepted treatment in active TIN with progressive renal insufficiency comprises the use of corticosteroids. For uveitis, topical steroids in association with cycloplegic agents are recommended; oral corticoids or other immunosuppressive medication are reserved for refractory cases11,18,20. The renal course is thought to be independent from ocular disease as neither the severity nor the prognosis of nephritis is influenced by the presence of uveitis40,41. Renal disease relapses in 9% and becomes chronic in 11–32% of cases, with only 5% requiring renal replacement therapy11,42.
Ocular inflammation may persist for more than 3 months in 14% of cases43 and recur in 40–50% of patients after corticoid withdrawal43,44. So, it seems that maintaining quiescence in the eye can be more difficult than in the kidney but overall, long-term prognosis is favorable for both organ systems6.
The mainstay of therapy in both cases was oral prednisolone at 1 mg/Kg/day. In case 1, the patient started ocular treatment with topical agents, but considering the lack of response and the presence of active tubulointerstitial nephritis, systemic corticosteroids were initiated as recommended. The patient presented in case two was initially medicated with topical steroids.
Oral corticosteroid (deflazacort) was initiated prior to our evaluation, given the presence of renal impairment. After making the AIN diagnosis (histologically), the switch to prednisolone was made. Even though the follow-up period was short, both patients experienced improved renal function, with no evidence of relapsing uveitis.
CONCLUSION
TINU is a rarely diagnosed syndrome with probable higher frequency than reported. Its clinical recognition may be hindered by the presence of non-specific symptoms, absence of concomitant renal and ocular manifestations and general limited knowledge of the disease.
As demonstrated in several studies, it may be worth screening for uveitis in all patients with tubulointerstitial nephritis and evaluating renal function in those presenting with apparent idiopathic uveitis. No randomized controlled trials exist regarding treatment; however observational studies suggest that corticosteroids and other immunosuppressive agents seem effective and this entity has an overall good prognosis.
It is thus essential to enhance awareness of general practioners and internists for a correct and timely referral and a optimal articulation between ophthalmologists and nephrologists for both correct diagnosis and treatment.
References
1. Goicoechea M, Rivera F, López-Gómez JM. Increased prevalence of acute tubulointerstitial nephritis. Nephrol Dial Transplant. 2013 Jan; 28(1): p. 112–5. [ Links ]
2. Bomback AS, Markowitz GS. Increased prevalence of acute interstitial nephritis: more disease or simply more detection? Nephrol Dial Transplant. 2013 Jan; 28(1): p. 16–8. [ Links ]
3. Praga M, González E. Acute interstitial nephritis. Kidney Int. 2010 Jun; 77(11): p. 956–61. [ Links ]
4. Su T, Gu Y, Sun P, Tang J, Wang S, Liu G, et al. Etiology and renal outcomes of acute tubulointerstitial nephritis: a single-center prospective cohort study in China. Nephrol Dial Transplant. 2017 Aug; 32(8): p. 1–9. [ Links ]
5. Muriithi AK, Leung N, Valeri AM, Cornell LD, Sethi S, Fidler ME, et al. Biopsy-proven acute interstitial nephritis, 1993-2011: a case series. Am J Kidney Dis. 2014 Oct; 64(4): p. 558–66. [ Links ]
6. Pakzad-Vaezi K, Pepple KL. Tubulointerstitial nephritis and uveitis. Curr Opin Ophthalmol. 2017 Nov; 28(6): p. 629–35. [ Links ]
7. Okafor LO, Hewins P, Murray PI, Denniston AK. Tubulointerstitial nephritis and uveitis (TINU) syndrome: a systematic review of its epidemiology, demographics and risk factors. Orphanet J Rare Dis. 2017 Jul; 12(1): p. 128. [ Links ]
8. Dobrin RS, Vernier RL, Fish AL. Acute eosinophilic interstitial nephritis and renal failure with bone marrow-lymph node granulomas and anterior uveitis. A new syndrome. Am J Med. 1975 Sep; 59(3): p. 325–33. [ Links ]
9. Mandeville JTH, Levinson RD, Holland GN. The tubulointerstitial nephritis and uveitis syndrome. Surv Ophthalmol. 2001 Nov-Dec; 46(3): p. 195–208. [ Links ]
10. Joyce E, Glasner P, Ranganathan S, Swiatecka-Urban A. Tubulointerstitial nephritis: diagnosis, treatment, and monitoring. Pediatr Nephrol. 2017 Apr; 32(4): p. 577–87. [ Links ]
11. Legendre M, Devilliers H, Perard L, Groh M, Nefti H, Dussol B, et al. Clinicopathologic characteristics, treatment, and outcomes of tubulointerstitial nephritis and uveitis syndrome in adults: A national retrospective strobe-compliant study. Medicine (Baltimore). 2016 Jun; 95(26): p. e3964. [ Links ]
12. Sinnamon KT, Courtney AE, Harron C, ORourke DM, Mullan RM. Tubulointerstitial nephritis and uveitis (TINU) syndrome: epidemiology, diagnosis and management. NDT Plus. 2008 Apr; 1(2): p. 112–6. [ Links ]
13. Kump LI, Cervantes-Castañeda RA, Androudi SN, Foster CS. Analysis of Pediatric Uveitis cases at a tertiary referral centre. Ophthalmology. 2005 Jul; 112(7): p. 1287–92. [ Links ]
14. Mackensen F, Smith JR, Rosenbaum JT. Enhanced recognition, treatment, and prognosis of tubulointerstitial nephritis and uveitis syndrome. Ophthalmology. 2007 May; 114(5): p. 995–9. [ Links ]
15. Saarela V, Nuutinen M, Ala-Houhala M, Arikoski P, Rönnholm K, Jahnukainen T. Tubulointerstitial nephritis and Uveitis syndrome in children: a prospective multicenter study. Ophthalmology. 2013 Jul; 120(7): p. 1476–81. [ Links ]
16. Mackensen F, Billing H. Tubulointerstitial nephritis and uveitis syndrome. Curr Opin Ophthalmol. 2009 Nov; 20(6): p. 525–31. [ Links ]
17. Hettinga YM, Scheerlinck LME, Lilien MR, Rothova A, de Boer JH. The value of measuring urinary b2-microglobulin and serum creatinine for detecting tubulointerstitial nephritis and uveitis syndrome in young patients with uveitis. JAMA Ophthalmol. 2015 Feb; 133(2): p. 140–5. [ Links ]
18. Sobolewska B, Bayyoud T, Deuter C, Doycheva D, Zierhut M. Long-term follow-up of patients with tubulointerstitial nephritis and uveitis (TINU) syndrome. Ocul ImmunolInflamm. 2016 Dec;: p. 1–7. [ Links ]
19. Clive DM, Vanguri VK. The syndrome of tubulointerstitial nephritis with uveitis (TINU). Am J Kidney Dis. 2018 Feb; pii: S0272-6386(17)31133-2. [ Links ]
20. Matsumoto K, Fukunari K, Ikeda Y, Miyazono M, Kishi T, Matsumoto R, et al. A report of an adult case of tubulointerstitial nephritis and uveitis (TINU) syndrome, with a review of 102 japanese cases. Am J Case Rep. 2015 Feb; 16: p. 119–23. [ Links ]
21. Levinson RD, Park MS, Rikkers SM, Reed EF, Smith JR, Martin TM, et al. Strong associations between specific HLA-DQ and HLA-DR alleles and the tubulointerstitial nephritis and uveitis syndrome. Invest Ophthalmol Vis Sci. 2003 Feb; 44(2): p. 653–7. [ Links ]
22. Reddy AK, Hwang YS, Mandelcorn ED, Davis JL. HLA-DR, DQ class II DNA typing in pediatric panuveitis and tubulointerstitial nephritis and uveitis. Am J Ophthalmol. 2014 Mar; 157(3): p. 678–86. [ Links ]
23. Mackensen F, David F, Schwenger V, Smith LK, Rajalingam R, Levinson RD, et al. HLADRB1* 0102 is associated with TINU syndrome and bilateral, sudden-onset anterior uveitis but not with interstitial nephritis alone. Br J Ophthalmol. 2011 Jul; 95(7): p. 971–5. [ Links ]
24. Santoro D, Vita G, Rovito S, Venuto L, Cavallari V, Vita R, et al. Drug-induced TINU syndrome and genetic characterization. Clin Nephrol. 2012 Sep; 78(3): p. 230–6. [ Links ]
25. Kawamata M, Akimoto T, Sugase T, Otani-Takei N, Miki T, Masuda T, et al. Tubulointerstitial Nephritis and Uveitis Syndrome: Are Drugs Offenders or Bystanders? Clin Med Insights Case Rep. 2016 Mar; 9: p. 21–4. [ Links ]
26. Perazella MA, Markowitz GS. Drug-induced acute interstitial nephritis. Nat Rev Nephrol. 2010 Aug; 6(8): p. 461–70. [ Links ]
27. Vanhaesebrouck P, Carton D, de Bel C, Praet M, Proesmans W. Acute tubulo-interstitial nephritis and uveitis syndrome (TINU syndrome). Nephron. 1985; 40(4): p. 418–22. [ Links ]
28. Conz PA, Milanb M, Bragantinib L, La Grecab G, Bevilac PA. TINU syndrome associated with reduced complement levels. Nephron. 2001 Nov; 89(3): p. 340-1. [ Links ]
29. Abed L, Merouani A, Haddad E, Benoit G, Oligny LL, Sartelet H. Presence of autoantibodies against tubular and uveal cells in a patient with tubulointerstitial nephritis and uveitis (TINU) syndrome. Nephrol Dial Transplant. 2008 Apr; 23(4): p. 1452–5. [ Links ]
30. Shimazaki K, Jirawuthiworavong GV, Nguyen EV, Awazu M, Levinson RD, Gordon LK. Tubulointerstitial nephritis and uveitis syndrome: a case with an autoimmune reactivity against retinal and renal antigens. Ocul Immunol Inflamm. 2008 Jan-Feb; 16(1): p. 51–3. [ Links ]
31. Li C, Su T, Chu R, Li X, Yang L. Tubulointerstitial nephritis with uveitis in chinese adults. Clin J Am Soc Nephrol. 2014 Jan; 9(1): p. 21–8. [ Links ]
32. Tan Y, Yu F, Qu Z, Su T, Xing GQ, Wu LH, et al. Modified C-reactive protein might be a target autoantigen of TINU syndrome. Clin J Am Soc Nephrol. 2011 Jan; 6(1): p. 93–100. [ Links ]
33. Onyekpe I, Shenoy M, Denley H, Riad H, Webb NJA. Recurrent tubulointerstitial nephritis and uveitis syndrome in a renal transplant recipient. Nephrol Dial Transplant. 2011 Sep; 26(9): p. 3060–2. [ Links ]
34. Zhou L, Li Y, Liu F, Peng Y, Liu Y, Li J. Excellent outcome of tubulointerstitial nephritis and uveitis: case report and five-year follow-up. Ren Fail. 2012; 34(7): p. 934–6. [ Links ]
35. Simon AHR, Alves-Filho G, Ribeiro-Alves MAVF. Acute tubulointerstitial nephritis and uveitis with antineutrophil cytoplasmic antibody. Am J Kidney Dis. 1996 Jul; 28(1): p.124–7. [ Links ]
36. Lee JW, Kim HJ, Sung SH, Lee SJ. A case of tubulointerstitial nephritis and uveitis syndrome with severe immunologic dysregulation. Pediatr Nephrol. 2005 Dec; 20(12): p. 1805–8. [ Links ]
37. Du L, Kijlstra A, Yang P. Immune response genes in uveitis. Ocul Immunol Inflamm. 2009 Jul-Aug; 17(4): p. 249–56. [ Links ]
38. Lee RW, Nicholson LB, Sen HN, Chan CC, Wei L, Nussenblatt RB, et al. Autoimmune and autoinflammatory mechanisms in uveitis. Semin Immunopathol. 2014 Sep; 36(5): p. 581–94. [ Links ]
39. Berney-Meyer L, Hung N, Slatter T, Schollum JBW, Kitching AR, Wlaker RJ. Omeprazoleinduced acute interstitial nephritis: a possible Th1-Th17-mediated injury? Nephrology (Carlton). 2014 Jun; 19(6): p. 359–65. [ Links ]
40. Jahnukainen T, Saarela V, Arikoski P, Ylinen E, Rönnholm K, Ala-Houhala M, et al. Prednisone in the treatment of tubulointerstitial nephritis in children. Pediatr Nephrol. 2013 Aug; 28(8): p. 1253–60. [ Links ]
41. Thomassen VH, Ring T, Thaarup J, Baggesen K. Tubulointerstitial nephritis and uveitis (TINU) syndrome: a case report and review of the literature. Acta Ophthalmol. 2009 Sep; 87(6): p. 676–9. [ Links ]
42. Pinheiro MA, Rocha MBC, Neri BO, Parahyba IO, Moura LAR, Oliveira CMC, et al. TINU syndrome: review of the literature and case report. J Bras Nefrol. 2016 Mar; 38(1): p. 132–6. [ Links ]
43. Liakopoulos V, Ioannidis I, Zengos N, Karabatsas CH, Karasavvidou F, Salmas M, et al. Tubulointerstitial nephritis and uveitis (TINU) syndrome in a 52-year-old female: a case report and review of the literature. Ren Fail. 2006; 28(4): p. 355–9. [ Links ]
44. Goda C, Kotake S, Ichiishi A, Namba K, Kitaichi N, Ohno S. Clinical features in tubulointerstitial nephritis and uveitis (TINU) syndrome. Am J Ophthalmol. 2005 Oct; 140(4): p. 637–41. [ Links ]
Ricardo A. Macau, MD
Hospital Garcia de Orta – Nephrology Department, Almada, Portugal
E-mail: ricardoandremacau@gmail.com
Acknowledgments
Authors would like to acknowledge Nephrology, Ophthalmology and Anatomic Pathology staff members.
Disclosure of potential conflicts of interest: none declared
Received for publication: Jan 9, 2018
Accepted in revised form: May 15, 2018


{kind=link}
{kind=link}