










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.32 no.2 Lisboa jun. 2018
CASE REPORT
Acute tubulointersticial nephritis with uveitis: A report of two cases
Filipa Silva, Sofia O Correia, Ana Castro, Carla Moreira, Sofia Santos, Jorge Malheiro, Josefina Santos, La Salete Martins, António Cabrita
Nephrology Department, Centro Hospitalar e Universitário do Porto, Porto, Portugal
ABSTRACT
Tubulointersticial nephritis and uveitis syndrome is an idiopathic and rare cause of acute kidney injury that should not overlooked, because it usually requires specific therapeutic interventions.
We report two distinct cases: a young and an elder female. Both cases presented with unspecific constitutional symptoms but had different onset of renal and ocular involvement. Both were treated with topical and systemic corticoids and although there was a good initial response in both cases, an early relapse after steroids taper was observed in the younger patient and a persistent renal dysfunction in the older one.
A high clinical suspicion and understanding of this disease is necessary for an adequate management and treatment of these patients. Recent data associates a worse renal prognosis when the disease appears inadvanced age. In both of our cases the outcome was good but we had a short follow-up. The histological presentation of this disease in our older patient was similar to that reported in the literature, with a high percentage of fibrosis and chronicity of renal tissue that can contribute to the higher grade of renal dysfunction in this type of patients.
Key-words: tubulointerstitial nephritis, anterior uveitis, glucocorticoids, renal dysfunction
INTRODUCTION
Tubulointersticial nephritis and uveitis (TINU) syndrome is defined by the combination of both idiopathic acute tubulointersticial nephritis (AIN) and uveitis.
It was described for the first time in 1975 by Dobrin et al.1 and more than 250 cases have now been reported, mostly in children and young females2,3, although it has also been reported in adults. There is also a female predominance in all series3,4. Estimated prevalence is around 3.5 cases/million of persons and the incidence is 0.2 cases/million/year5,6.
No identifiable risk factors have been found in at least 50 percent of cases3,4. In some of them, prior infections and/or use of specific drugs have been reported3,4,7. There is no particular affinity with race, familiar inheritance, genetics or geographic clusters3.
The correct diagnosis can be difficult to establish especially when the renal involvement is mild. The exclusion of other systemic diseases is mandatory and the ophthalmological evaluation plays an important role in the presence of interstitial nephritis with no defined etiology.
We report two different cases of TINU syndrome, one in a young and another in an older female. Although they had similar constitutional symptoms at presentation, the renal and ocular manifestations as well as the response to the treatment was distinct.
CASES REPORT
Case 1
An 18-year-old female with recent diagnosis of hyperthyroidism presented in the emergency department with a 9 months history of photophobia. She was treated with antibiotics, given the suspicion of bilateral purulent conjunctivitis. Two months before admission started, there were complaints of weight loss, vomiting, abdominal pain, diarrhea, fatigue and anorexia. Blood samples showed anemia and altered renal function with serum creatinine (sCr) of 1.8mg/dL, hypouricemia and hypophosphatemia. Presence of glycosuria, granular casts and proteinuria (< 1g/per day) was visible in the urinalysis. Renal ultrasonography was normal as were immunological markers (antinuclear antibody (ANA), antineutrophil cytoplasmic antibody (ANCA), anti-double-stranded DNA (anti-dsDNA), HLAB27, anti-RNP/Smith, SSA, SSB, SCL70, and antoJo1).
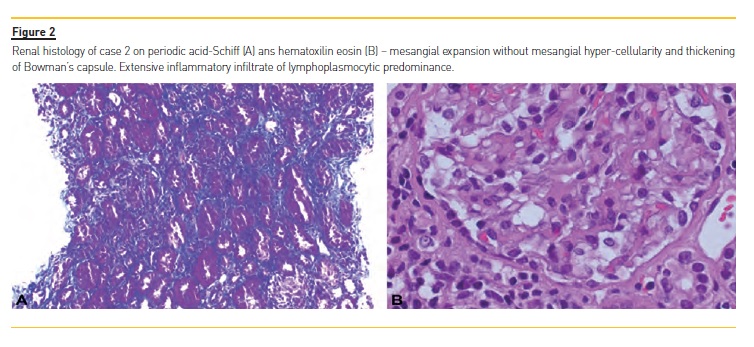
Angiotensin converting enzyme (ECA) and serology for syphilis (VDRL) were also negative. Kidney biopsy revealed mesangial expansion without mesangial hyper-cellularity and thickening of Bowman´s capsule.
Extensive interstitial inflammation with lymphoplasmocytic predominance occupying more than 25% of the extension of the cortex was observed. Fibrosis in approximately 5 to 10% of the cortical extension was noticeable. Tubular atrophy was present in 10% of the cortex. Arterial branches and arterioles had concentric wall thickening. The direct immunofluorescence study with antibodies to albumin, C3, C4, C1q, IgA, IgG and IgM showed vestigial mesangial and focal C3 in the tubular membrane with absence of deposits for the remaining antibodies tested. Electron microscopy showed no ultrastructural changes.
Ophthalmologic evaluation documented bilateral anterior uveitis. She started corticoid therapy, ocular and systemic (prednisolone 1mg/Kg/day), with early recovery of renal function. She had recurrent uveitis when steroids taper was performed (after 3 months), with 2 episodes of recurrent uveitis, the last one needing systemic corticotherapy (completing 1 year of prednisolone).
After 2 years, she maintains normal renal function (sCr of 1mg/dL) and no signs of tubular dysfunction (ratio proteinurine/creatinineurine 0.1g/g), no glycosuria (0mg/dL) or granular casts (0-2/field).
Case 2
A 71-year-old female with an unremarkable past medical history: no chronic medication or recent use of nonsteroidal anti-inflammatory drugs (AINEs); no history of tobacco or alcohol. She presented with weight loss, fatigue, asthenia and malaise in the previous 4 months. No other symptoms were reported. At hospital admission she presented with an elevated C-reactive protein (CRP), 100mg/L and erythrocyte sedimentation rate (ESR), 74mm. Blood samples showed new onset of normocytic, normochromic anemia (haemoglobin 9.3g/dL) and acute renal failure KDIGO 3 (sCr increased from 0.9mg/dL to 3.1mg/dL).
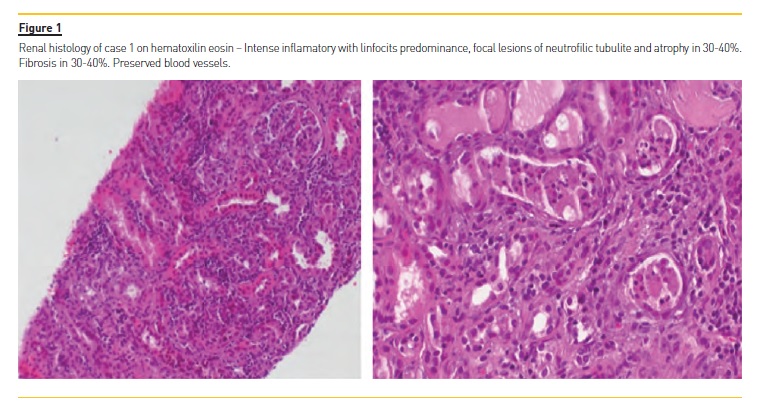
Urinalysis showed proteinuria (ratio proteinurine/creatinineurine 1.2g/g), glycosuria (>1000mg/dL) and granular casts (10-25/field) and no eosinophiluria or eosinophilia. No abnormalities in the renal ultrasound were observed. ANA, ANCA, anti-dsDNA, HLA-B27, anti-RNP/Smith, SSA, SSB, SCL70, and antoJo1 antibodies were negative. ECA and VDRL were also negative. In renal biopsy, two of the twenty-six glomeruli identified had global sclerosis, showing interstitial inflammation with intense infiltrate of lymphocyte predominance, occupying 25% of cortical extension. Fibrosis in 30 to 40% of the sample was noticeable. Renal tubules appeared with thickened basement membrane and focal lesions of neutrophilic tubulitis. Tubular atrophy in 30 to 40% was detectable. Arterial branches and arterioles had discrete intima myofibroblastic thickening.
Immunofluorescence study with antibodies to albumin, C3, C4, C1q, IgA, IgG, IgM, kappa and lambda chains revealed absence of immune deposits. Immunohistochemical study was compatible with lymphocyte population composed mainly by T lymphocytes. She had no ocular symptoms but evidence of bilateral anterior uveitis was present on ocular examination. Prednisolone, 1mg/Kg/day, was initiated with early recover of renal function. She started steroids taper after 3 months and they were stopped after 5 months (sCr 1.4mg/dL). After 10 months of follow-up she had no anemia (Hb 12.9g/dL), low VS (10mm), sCr 1.4mg/dL and no signs of tubular dysfunction (ratio proteinurine/creatinineurine 0.3g/g), no glycosuria (0mg/dL) or granular casts (0-2/field).
DISCUSSION
With this case report the authors want to emphasize the importance of suspecting this syndrome when in the presence of an acute interstitial nephritis of unclear etiology. In addition, idiopathic AIN patients must have an ocular examination since they could have uveitis with no ocular symptom, as was the case in one of the patients.
It is also important to notice that despite the lack of long-term follow-up, the older patient appears to have a worse prognosis and the difference could in part be explained by the tendency for accelerated fibrosis in the older patient. The underlying mechanism of TINU remains unclear.
Some studies suggest that IgG antibodies directed to modified CRP, an autoantigen common to both renal tubular cells and uvea may be implicated in the pathogenesis, since they are significantly higher in TINU patients than when compared with patients with other diseases (Sjogren syndrome, drug-induced interstitial nephritis, glomerulonephritis, IgA nephropathy, minimal change disease, ANCA associated vasculitis and amyloidosis) or healthy controls8.
Gafter at al.9 associated TINU syndrome to the suppression of cell-mediated immunity and reported normal T-cell population but decreased secretion of lymphokines and anergy to skin tests in these patients. This paradox is not unique to TINU, as increased tissue inflammation with concomitant suppression of peripheral immunity is also seen in patients with sarcoidosis9,10.
Other studies reported a genetic association with HLA-DQA1*01, HLADQB1*05 and HLA-DQB1*013,7.
There has also been reported TINU syndrome in patients with autoimmune diseases like hypoparathyroidism, thyroid disease, immunoglobulin G4 related autoimmune disease and rheumatoid arthritis3,8,11-13.
TINU may present with unspecific general symptoms4,14 like those that occurred in both of our patients.
The typical ocular presentation of TINU syndrome is bilateral and nongranulomatous anterior uveitis with sudden onset in 80% of patients, but may also manifest as posterior or panuveitis4,16. Ocular symptoms include eye redness and pain, photophobia and decreased visual acuity.
Renal manifestations include flank pain, sterile pyuria, proteinuria, hematuria and acute kidney injury.
Proximal and distal tubular defects can be commonly seen, resulting in aminoaciduria, glycosuria, phosphaturia and acidifications defects17,18. Nephritis precedes uveitis in 65%, in 21% of cases uveitis is present before nephritis and in 15% the two occur in simultaneously4.
In our report, one patient presented first ocular disease and the other renal involvement.
There are no specific serum markers or laboratory findings that suggest TINU. We may find leucocyturia, eosinophilia, anemia, slightly abnormal liver functions test and an elevated ESR and CRP3. Beta 2 microglobulin and Krebs von den Lunge-6 (KL-6) could be two potential diagnostic markers according to some reports and the levels of beta 2 microglobulin were correlated with histologic grade of tubulointerstitial nephritis in 10 children19. Compared with patients with uveitis from other causes, serum KL-6 levels were significantly elevated in patients with TINU syndrome. Renal biopsies stained strongly with anti KL-6 antibody suggest that the elevated KL-6 levels reflect the underlying renal lesion20.
However, KL-6 levels were no different between patients with TINU syndrome or drug-induced interstitial nephritis3.
TINU syndrome might be underdiagnosed due to lack of recognition8. The definitive diagnosis is nonspecific and is suggested by the combination of renal involvement and uveitis with renal biopsy consistent with AIN. On light microscopy, typical biopsy findings include tubulointerstitial edema and infiltration of inflammatory cells composed mainly of mononuclear cells. Glomerular and vascular structures are generally preserved. There are no specific findings with immunofluorescence and electron microscopy21.
In our cases, all kidneys biopsies had inflammatory infiltrate with lymphocyte predominance. No alterations on immunofluorescence or electronic microscopywere found. The older patient presented with more fibrosis and tubular atrophy translating into a worse outcome when compared with the younger patient, who had less signs of chronicity on biopsy.
Treatment is not yet standardized and varies between centers and clinicians22.
Topical corticosteroids are recommended as the firstchoice treatment in anterior uveitis24. However, 80% of patients requires systemic corticosteroids and 9% progress to other immunosuppressive treatment4.
Sobolewska et al.23 suggested that treatment duration of at least 12 months with oral systemic corticosteroids or immunomodulatory agents may reduce or prevent the recurrence rate in patients who relapse.
Our approach consists in initiate both topic and systemic corticoterapy. We usually initiate, as is recommended20, with oral prednisolone at 1mg/kg/day in cases with progressive renal impairment. Therapy is given by three to six months depending on the response and then is slowly tapered. In our cases we started tapering corticoterapy after 3 months and stopped after5. The younger patient had a relapse of uveitis after systemic corticoterapy tapering, with accordance with literature that report more tendency for eye symptoms than renal to occur (40% vs 9%, respectively, at 1 year follow up)3,4,22,24. On the other hand, the older patient progressed to chronic disease, which is more frequent for renal symptoms. None of them has of yet started any additional immunosuppressive drugs.
The long term prognosis isnt well established since there is few data to follow-up along with. While the most reports described TINU syndrome as having a favorable renal outcome4,19,24,25, other data suggests that full renal recovery is not the norm, with the patients evolving to impaired renal function in the medium term3,22.
Legendre et al22. recently report new data suggesting that with the older the patient is, the poorer is the renal prognosis after 1 year of follow-up. In addition, they also associated the initial severity of renal symptoms with the renal function after 1 year of follow-up.
This data was in accordance with our cases, in which the older patient presented with a higher grade of renal dysfunction, more fibrosis was present in the renal biopsy and there was a progression to chronic renal dysfunction.
Until now, no pathological markers proved to be prognostic factors in TINU syndrome3,4.
CONCLUSION
TINU syndrome is a rare disease and it may be difficult to identify.
Patients that have acute interstitial nephritis on renal biopsy and have no obvious underlying cause may require a slit lamp examination to exclude uveitis.
This disease should be considered in the differential diagnosis of tubulointersticial nephritis of unclear etiology, especially in the presence of ocular manifestations, in older patients where the disease is probably underdiagnosed, and in young patients with asymptomatic mild renal disease.
The long-term care is fundamental given the possible evolution with impaired renal function, especially in elder people.
References
1. Dobrin RS, Vernier RL, Fish AL. Acute eosinophilic interstitial nephritis and renal failure with bone marrow-lymph node granulomas and anterior uveitis. A new syndrome. Am J Med 1975; 59:325. [ Links ]
2. Abed L, Merouani A, Haddad E, et al. Presence of autoantibodies against tubular and uveal cells in a patient with tubulointerstitial nephritis and uveitis (TINU) syndrome. Nephrol Dial Transplant 2008; 23:1452. [ Links ]
3. Li C, Su T, Chu R, et al. Tubulointerstitial nephritis with uveitis in Chinese adults. Clin J Am Soc Nephrol 2014; 9:21. [ Links ]
4. Mandeville JT, Levinson RD, Holland GN. The tubulointerstitial nephritis and uveitis syndrome. Surv Ophthalmol 2001; 46:195. [ Links ]
5. Helms E, Sevilla KS, Hartshorne MF, Harris A, Nichols MJ, Tzamaloukas AH. Tubulointersticial nephritis and uveitis syndrome: use of gallium scintigraphy in its diagnosis and treatment. Int Urol Nephrol 2005; 37:119-22. [ Links ]
6. Weinstein O, Tovbin D, Rogachev B, Vorobiov M, Kratz A, et al. Clinical manifestations of adult tubulointerstcial nephritis and uveitis (TINU) syndrome. Int Ophthalmol 2010; 30:621-8. [ Links ]
7. Levinson RD, Park MS, Rikkers SM, et al. Strong associations between specific HLA-DQ and HLA-DR alleles and the tubulointerstitial nephritis and uveitis syndrome. Invest Ophthalmol Vis Sci 2003; 44:653. [ Links ]
8. Tan Y, Yu F, Qu Z, et al. Modified C-reactive protein might be a target autoantigen of TINU syndrome. Clin J Am Soc Nephrol 2011; 6:93. [ Links ]
9. Gafter U, Kalechman Y, Zevin D, et al. Tubulointerstitial nephritis and uveitis: association with suppressed cellular immunity. Nephrol Dial Transplant 1993; 8:821. [ Links ]
10. Yoshioka K, Takemura T, Kanasaki M, et al. Acute interstitial nephritis and uveitis syndrome: activated immune cell infiltration in the kidney. Pediatr Nephrol 1991; 5:232. [ Links ]
11. Catalano C, Harris PE, Enia G, et al. Acute interstitial nephritis associated with uveitis and primary hypoparathyroidism. Am J Kidney Dis 1989; 14:317. [ Links ]
12. Paul E, Van Why S, Carpenter TO. Hyperthyroidism: a novel feature of the tubulointerstitial nephritis and uveitis syndrome. Pediatrics 1999; 104:314. [ Links ]
13. Yoneda K, Murata K, Katayama K, et al. Tubulointerstitial nephritis associated with IgG4-related autoimmune disease. Am J Kidney Dis 2007; 50:455. [ Links ]
14. Jahnukainen T, Ala-Houhala M, Karikoski R,et al. Clinical outcome and occurrence of uveitis in children with idiopathic tubulointersticial nephritis. Pediatr Nephrol Berl Ger 2011; 26:291-9. [ Links ]
15. Han JM, Lee YJ, Woo SJ. A case of tubulointersticial nephritis and uveitis syndrome in an elderly patient. Korean J Ophthalmol 2012;26:398-401. [ Links ]
16. Mackensen F, Smith JR, Rosenbaum JT: Enhanced recognition, treatment, and prognosis of tubulointersticial nephritis and uveitis syndrome. Ophthalmology, 2007; 114(5): 995-99. [ Links ]
17. Igarashi T, Kawato H, Kamoshita S, et al. Acute tubulointerstitial nephritis with uveitis syndrome presenting as multiple tubular dysfunction including Fanconis syndrome. Pediatr Nephrol 1992; 6:547. [ Links ]
18. Koike K, Lida S, Usui M, et al. Adult-onset acute tubulointerstitial nephritis and uveitis with Fanconi syndrome. Case report and review of the literature. Clin Nephrol 2007; 67:255. [ Links ]
19. Takemura T, Okada M, Hino S, et al. Course and outcome of tubulointerstitial nephritis and uveitis syndrome. Am J Kidney Dis 1999; 34:1016. [ Links ]
20. Parameswaran S, Mittal N, Joshi K, et al. Tubulointersticial nephritis with uveitis syndrome: A case report and review of literature. Indian J Nephrol 2010; 20:103-5. [ Links ]
21. Joss N, Morris S, Young B, Geddes C. Granulomatous interstitial nephritis. Clin J Am Soc Nephrol 2007; 2:222. [ Links ]
22. Legendre M, Devilliers H, Perard L, et al. Clinicopathologic characteristics, treatment, and outcomes of tubulointerstitial nephritis and uveitis syndrome in adults: a national retrospective strobe-compliant study. Medicine 2016; 95:26. [ Links ]
23. Sobolewska B, Bayyoud T, Deuter C, et al. Long-term follow up of patients with tubulointersticial nephritis and uveitis (TINU) syndrome. Ocular Immunology e Inflamation, 2016; 26:4, 601-607. [ Links ]
24. Goda C, Kotake S, Ichiishi A, et al. Clinical features in tubulointersticial nephritis and uveitis (TINU) syndrome. Am J Ophthalmol 2005; 40:637-41. [ Links ]
25. Kobayashi Y, Honda M, Yoshikawa N, et al. Acute tubulointersticial nephritis in 21 Japanese children. Clin Nephrol 2000; 54:191-7. [ Links ]
Filipa Silva, MD
Nephrology Department, Centro Hospitalar e Universitário do Porto,
Porto, Portugal.
Email: filipasofiasantossilva@gmail.com
Disclosure of potential conflicts of interest: the authors declare no conflicts of interest.
Received for publication: Jan 31, 2018 Accepted in revised form: May 29, 2018


{kind=link}
{kind=link}