










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.33 no.1 Lisboa mar. 2019
https://doi.org/10.32932/pjnh.2019.04.014
TUBULAR QUIZ
A child with acute kidney injury
Rui Domingues1, Tânia Moreira1, Telma Francisco2, Sara Nóbrega3, António Pedro Campos3, Raul Silva3, Margarida Abranches2
1Unidade Funcional de Pediatria Médica, Área da Mulher, Criança e Adolescente, Hospital Dona Estefânia, Centro Hospitalar Universitário de Lisboa Central
2 Unidade de Nefrologia Pediátrica, Área da Mulher, Criança e Adolescente, Hospital Dona Estefânia, Centro Hospitalar Universitário de Lisboa Central
3 Unidade de Cuidados Especiais Respiratórios e Nutricionais, Área da Mulher, Criança e Adolescente, Hospital Dona Estefânia, Centro Hospitalar Universitário de Lisboa Central
CASE PRESENTATION
We present the case of an 18-month-old boy born with intestinal atresia type IIIa, resulting in short bowel syndrome, treated with home parenteral nutrition by an indwelling central line and weighing 8.300 kg (<3rd centile).
He was admitted to the hospital with a catheter-related bloodstream infection (CRBSI) caused by methicillin-resistant Staphylococcus aureus. The patient was treated with intravenous vancomycin and gentamicin for 14 days.
Three days after finishing this course of antibiotics, the patient presented a second CRBSI caused by Pseudomonas aeruginosa and Candida albicans, and therefore intravenous amphotericin B, gentamicin and ceftazidime were initiated.
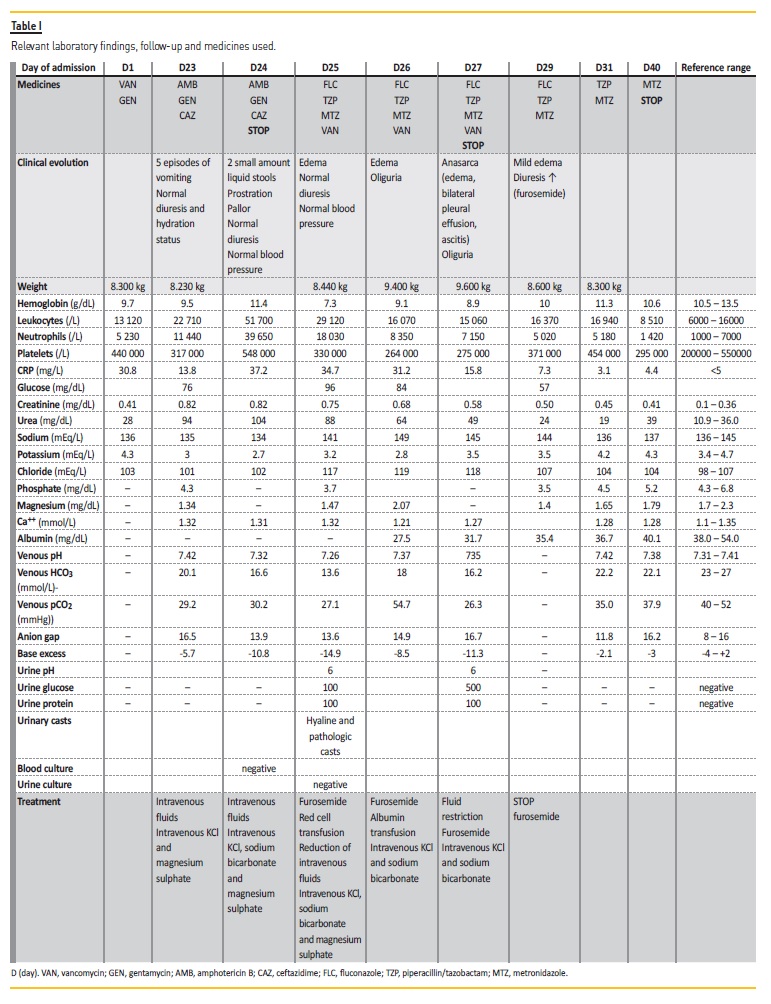
On day 24 of hospitalization (8 days after starting the second antibiotic cycle), the patient started vomiting (five episodes, small amount) and having diarrhea (two liquid stools, small amount), followed by prostration, pallor and poor peripheral perfusion. Laboratory workup at this time and a few days after showed anemia, leukocytosis with neutrophilia, increasing C-reactive protein (CRP), metabolic acidosis, hypokalemia, hypophosphatemia, hypomagnesemia, hypoalbuminemia,
elevated serum urea and creatinine, glycosuria and proteinuria.
Estimated glomerular filtration rate (eGFR) was 52 mL/min/1,72 m2. (Table 1). Astrovirus was isolated from stools. Hydroelectrolytic disorders were treated with intravenous fluids and sodium bicarbonate, potassium chloride and magnesium sulphate; red cells and albumin transfusions were prescribed.
In the context of central line infection and worsening inflammatory markers, nephrotoxicity caused by amphotericin B and gentamicin was suspected, so both medicines were stopped and replaced by intravenous fluconazole, piperacillin/tazobactam, metronidazole and vancomycin.
On day 27 of hospitalization (and day 3 of the third antimicrobial cycle) the patient developed oliguria (minimum of 0.5 milliliters/kg/hour), anasarca (edema, weight gain of 1.2 kg, bilateral pleural effusion and ascites) and worsening metabolic acidosis with respiratorycompensation, despite improvement in kidney function. He was treated with intravenous sodium bicarbonate and vancomycin was stopped. Hydric restriction and furosemide, with strict evaluation of enteric fluid losses and diuresis, were started, with significant improvement after 48 hours.
WHY DID THIS PATIENT DEVELOP HYPOPHOSPHATEMIA AND HYPOKALEMIA, DESPITE AN ACUTE KIDNEY INJURY?
Acute kidney disease (AKI) is defined by Kidney Diseases Improving Global Outcomes (KDIGO) as an increase in creatinine of ≥50% or an absolute increase of creatinine of 0.3 mg/dL or an eGFR ≤35 ml/min per 1.73 m2 or a urine output <0,5mL/kg/hour in 6-12 hours (stages 1-3 are defined according to severity of theses alterations).1 AKI is characterized by an increase in the blood concentration of creatinine and nitrogenous waste products and by the inability of the kidney to regulate the fluid and electrolyte homeostasis appropriately2, causing metabolic acidosis, hyperkalemia and hyperphosphatemia. However, our patient presented hypokalemia, hypomagnesemia and hypophosphatemia, along with metabolic acidosis, glycosuria, and proteinuria. Altogether, these results indicate a tubular disorder.
WHAT’S THE MOST PROBABLE CAUSE OF RENAL LESION IN THIS CASE?
This patient has a severe chronic condition (short bowel syndrome) leading to intestinal failure, poor oral feeding, had a multi-agent CRBSI and simultaneously a viral gastroenteritis, which could lead to dehydration.
However, the Astrovirus gastroenteritis was not serious enough (only a few episodes of vomiting through the day, in small amount, and two small liquid stools) to cause, by itself, AKI, acidosis and electrolytic disorders. Furthermore, the patient was treated with several nephrotoxic drugs: amphotericin B, gentamicin, piperacillin/tazobactam and vancomycin.
Several studies indicate that among hospitalized children, nephrotoxic drug exposure is one of the most common contributors to AKI.3
Drug-induced tubular disorders have been described with several medications that are handled through tubular transport mechanisms.4
Several patterns have been described, ranging from isolated abnormalities (e.g. phosphate leak) to more generalized lesions contributing to a proximal renal tubular acidosis or an acquired Fanconi syndrome. By recognizing the wide spectrum of tubular dysfunction, we must include abnormalities in urinary losses of phosphate, glucose, magnesium, potassium, and tubular proteins or water handling.
In aminoglycosides, nephrotoxicity is associated with a varying degree of renal tubular dysfunction that may, in the most severely affected patients, lead to AKI.1
Aminoglycosides cause damage primarily to tubular epithelial cells3 (particularly proximal tubular cells5), but can also have an adverse effect on renal function via activation of the renin-angiotensin-aldosterone system and changes of glomerular endothelial cells.3 Other mechanisms involved are the direct and indirect effects on the mitochondria that lead to the disruption of electron transport and ATP production and the production of reactive oxygen species.1 Patients may present with oliguric AKI, along with proximal tubule dysfunction, resulting in loss of enzymes, proteins, glucose, calcium, potassium and magnesium. Most patients recover but some can progress to chronic interstitial nephritis.5 There are several risk factors that can increase the nephrotoxic potential of aminoglycosides, such as preexisting renal disease, treatment for more than 10 days, higher trough levels and hypoalbuminemia.4
The role of vancomycin as a nephrotoxin remains controversial, particularly in the context of monotherapy with appropriate drug monitoring levels.5 However, there is evidence that vancomycin has detrimental oxidative effects on proximal tubule cells.3 The exact mechanism of nephrotoxicity remains unclear, but may be related to oxidative effects on the proximal tubule.6 Moreover, simultaneous use of vancomycin and piperacillin/tazobactam has been linked to the development of AKI in non-critically ill children. There is even more evidence suggesting substantial nephrotoxicity associated with piperacillin/tazobactam, independent of vancomycin use.6 Furthermore, the combined use of vancomycin and aminoglycoside may increase nephrotoxicity.6
Nephrotoxicity represents the most significant side effect of amphotericin B (80% of patients5) and results from a combination of vasoconstriction and direct distal tubular toxicity.5 The direct toxicity and increased tubular membrane permeability accounts for the characteristic electrolyte abnormalities that can be seen after amphotericin B administration (hypokalemia, hyponatremia, acidosis and hypomagnesemia).5 In our patient, the hypomagnesemia found on day 23 (table 1) was most probably related with treatment with amphotericin B, as this drug was prescribed seven days before.
WHICH RISK FACTORS FOR DRUG NEPHROTOXICITY CAN BE FOUND IN THIS CASE?
In hospitalized children, predisposing factors such as age3,6, low weight-for-age3, severity of illness, pharmacogenetics, dosage, duration, and concomitant nephrotoxic medication determine and influence the severity of nephrotoxic insult.6 In this case, several risk factors can be identified for AKI, such as low weight, young age (<5 years), sepsis, dehydration, low serum albumin, association of several nephrotoxic drugs (aminoglycosides, vancomycin, piperacillin/tazobactam and amphotericin B) and a prolonged treatment with gentamicin.
As a critically ill patient, he is at the highest risk for drug-induced comorbidities of AKI, sepsis, hypotension, polypharmacy, and poor estimation of renal function.3 Regular assessment of serum creatinine levels, urine output and drug monitoring (peak and trough drug levels for aminoglycosides and vancomycin) allow early recognition of the development of AKI with the need to further adjustment of drug dosing to the eGFR.
CASE FOLLOW-UP
The patient showed progressive improvement of his clinical condition, and after three days, acidosis and the other tubular disorders were solved. Urea and creatinine blood levels showed progressive improvement and, on hospital discharge, he had nearly normal renal function (Table 1).
With this case, authors intend to warn of the potential nephrotoxic effects of some drugs currently used in everyday practice. A high index of suspicion is required to identify potential at-risk children for drugassociated AKI. As there is no specific treatment for AKI, preventive measures include assuring an adequate hydration status, avoiding nephrotoxic medications and adjusting drug dosing to eGFR, particularly when a combination of nephrotoxic agents is required and the patient presents many risk factors for AKI.
References
1. McWilliam SJ, Antoine DJ, Smyth RL, Pirmohamed M. Aminoglycoside-induced nephrotoxicity in children. Pediatr Nephrol 2017; 32:2015–2025 [ Links ]
2. Andreoli SP. Acute kidney injury in children. Pediatr Nephrol 2009; 24:253–263 [ Links ]
3. Joyce EL, Kane-Gill SL, Fuhrman DY, Kellum JA. Drug-associated acute kidney injury: who’s at risk? Pediatr Nephrol 2017; 32:59–69
4. Mehta RL, Awdishu L, Davenport A, Murray PT, Macedo E, Cerdad J, Chakaravarthi R, Holden AL, Goldstein SL. Phenotype standardization for drug-induced kidney disease. Kidney Int 2015; 88:226–234 [ Links ]
5. Faught LN, Greff M, Rieder MJ, Koren G. Drug-induced acute kidney injury in children. Br J Clin Pharmacol 2015;80(4):901–909 [ Links ]
6. Hanna MH, Askenazi DJ, Selewski DT. Drug-induced acute kidney injury in neonates. Curr Opin Pediatr 2016; 28:180–187 [ Links ]
Rui Pereira Domingues; MD
Área da Mulher, Criança e Adolescente, Hospital Dona Estefânia, CHULC.
Rua Jacinta Marto, 1169-045 Lisboa.
E-mail: rp.domingues87@gmail.com
Disclosure of potential conflicts of interest: none declared.
Received for publication: Feb 2, 2019
Accepted in revised form: Mar 26, 2019


{kind=link}