










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.33 no.2 Lisboa jun. 2019
https://doi.org/10.32932/pjnh.2019.07.023
CASE REPORT
Severe passenger lymphocyte syndrome associated to Rh antibodies after donor living renal transplantation
Marika Bini Antunes1, Jorge Malheiro2, Leonidio Dias2, La Salete Martins2, Sofia Pedroso2, Manuela Almeida2, Antonio Castro Henriques2, Margarida Amil1
1 Serviço de Hematologia Clinica, Centro Hospitalar Universitário do Porto (Porto, Portugal)
2 Serviço de Nefrologia, Centro Hospitalar Universitário do Porto (Porto, Portugal)
ABSTRACT
The passenger lymphocyte syndrome may cause hemolytic anemia after bone marrow and solid organ transplantation when there is minor erythrocyte antigen incompatibility in the donor/recipient pair. Anemia is usually self-limiting, frequently related to ABO antibodies and rarely to Rh mismatches.
We report a rare case of passenger B lymphocyte syndrome mediated by Rh antibodies occurring after a donor living renal transplantation and discuss its clinical severity at presentation, the therapeutic decisions and their outcome.
Keywords: Passenger lymphocyte; transplantation; Rh antibody
INTRODUCTION
Passenger B lymphocyte syndrome (PBLS) has been described after hematopoietic progenitors and solid organ transplantation1,2 and may occur when there is a minor erythrocyte antigen mismatch between donor and recipient. It is mediated by graft B lymphocytes that recognize erythrocyte antigens as non-self with subsequent alloimmune response causing hemolytic anemia, through the production of antibodies against recipient red cell antigens. PBLS incidence in kidney transplantation (KT) varies between 9 and 20% according to publications1-3. It is predominantly mediated by ABO isoagglutinins and rarely by Rh antibodies. A Coombs positive anemia 7-14 days after a transplant with minor blood antigens incompatibility should raise diagnostic suspicion for this entity2. A correct and prompt management is essential to ensure a good outcome.
CASE REPORT
A fifty-three-year-old woman with end stage renal disease secondary to IgA nephropathy was admitted for donor living KT in July 2018. She was on peritoneal dialysis (PD) since August 2014 and was submitted to living donor KT from her sister in October 2014.
The patient was O Rh positive (ccDEe) and had negative indirect antiglobulin test (IAT) and negative direct antiglobulin test (DAT); Her HLA low resolution typing was: A (2, 32); B (65, 63); DR1,13. Her sister was O Rh positive; HLA low resolution typing: A (1, 32); B (8, 14); DR (1, 8). Complement dependent cytotoxicity (CDC) and flow cytometry cross match were negative, panel reactive antibody (PRA) was 0%. This first transplantation surgery was complicated by immediate graft arterial thrombosis and graft nephrectomy was needed at day (D)1, with patient returning to PD. A thrombophilia study did not detect any mutation in prothrombin gene and FV Leiden. Circulating phospholipid antibodies as well as ATIII, protein C and protein S deficiencies were excluded.
Her present donor was a fifty-three -year-old female friend. Her blood group was O Rh negative (ccdee). In her obstetric anamnesis, she referred an Rh immunizing event during a 1st pregnancy in 2005 and occurrence of foetal haemolytic disease mediated by anti-Rh (D) during her 2nd pregnancy in 2011, with need for cesarean delivery at 32 week of gestation. Her low-resolution HLA typing was: A (2); B (44, 51); DR (7, 18).
Complement dependent cytotoxicity (CDC) and flow cytometry cross match were negative; panel reactive antibody (PRA) was 0%. A nondonor specific low title anti-HLA A1 was detected.
Her immunosuppression protocol included Basiliximab, tacrolimus, mycophenolate mofetil and corticoids. The surgical procedure was complicated with thrombosis of proximal iliac artery and an urgent thrombectomy was performed at D1, followed by a haemorrhagic shock. At D2 Balloon angioplasty was done but after rupture of the heterologous graft renal artery a surgical bypass with interposition of large saphenous vein was required.
She had delayed graft function, remaining on haemodialysis for 4 days. Given this complicated immediate post-KT period, adequate tacrolimus trough levels were not achieved and clinicians opted for changing induction strategy, starting anti-thymocyte globulin (ATG) at D3 that was administered for 7 consecutive days.
She was transfused with 9 O Rh positive (Phenotype ccDEE or ccDEe) red blood cells (RBCs) between D1 and D14.
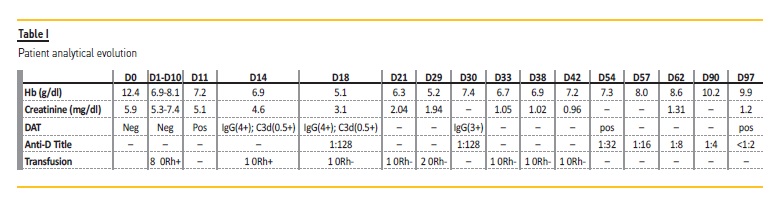
At D11 she presented a positive direct antiglobulin test (DAT), confirmed at D14 (DAT positive IgG 4+, C3d 0.5+), when she was again transfused with an O Rh positive RBC. At D18 she maintained a positive DAT with a strongly reactive eluate and identification of anti D. The IAT was also strongly positive and anti-D was titled 1:128. Hemoglobin dropped to 5.1 g/dl and positive criteria for extra and intravascular haemolysis were documented with absolute reticulocytes 356 x109/l, DHL 431 U/L, indirect hyperbilirubinemia (1.6 mg/dl) and undetectable haptoglobins.
Platelets counts and coagulations times and fibrinogen were in normal range (platelets 348 x 109 /L, prothrombin time 12.4 seconds (sec)/normal 11.4 sec, partial activated thromboplastin time 33.9 sec/normal 26.9 sec, fibrinogen 336 mg/dl). Peripheral blood smear did not show schistocytes or other morphologic alterations suggestive of thrombotic microangiopathy.
A PBLS was diagnosed. She was transfused with 7 O Rh negative (phenotype rr) RBCs between D18 and D42.
She was also treated with polyvalent human immunoglobulin (0.5 g/kg/day x 3 days) and methylprednisolone (625 mg x 3 days). Immunohematology clinical evolution is shown in Table I.
On D44 she reached clinical and analytical stability (creatinine 0.9 mg/dl, Hb 9.0 g/dl, reticulocyte count 152 x 109/L, DHL 279 U/L and indirect bilirubin 0.78 mg/dl) and was discharged.
DAT+ Hemolytic anemia persisted for over 3 months with hemoglobin values between 7.3 g/dl and 10.2 g/dl (Table I), reticulocytosis and slightly elevated DHL and indirect bilirubin. Six months after KT the patient had hemoglobin 12.2 g/dl but maintained a positive IAT with an anti-D title 1:2.
DISCUSSION
The role of donor tissue-resident lymphocytes subsets has increasingly been studied in solid organ transplantation. Donor lymphocytes, in particular donor derived tissue resident T regulatory (Treg) cells, seem to be required for tolerance induction, as evidenced by the fact that irradiation of donor graft in rodent models led to rejection of otherwise tolerated transplants4.
Additionally, donor derived tissue resident T cells might also protect against infection4.
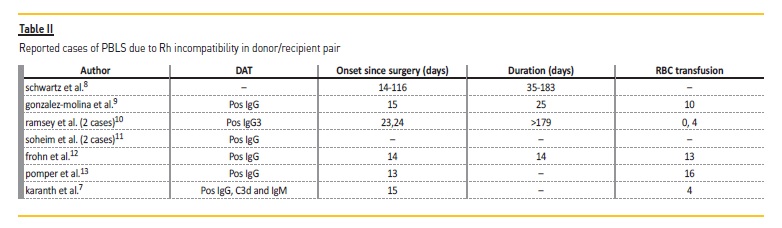
However, donor memory CD4+ T cells and donor passenger B lymphocytes may be implicated in moderate to severe immune complications after solid organ transplantation. Several cases of PBLS in the context of renal transplantation have been described, mainly related to minor ABO incompatibility3,5,6. PBLS due to Rh incompatibility is rarer, with only 10 reported cases to our knowledge (Table II)3,7.
The severity of the hemolytic condition is variable and may be related to the conditioning regimen, to the amount of lymphocytes transferred with the engraft as well as to the type of implicated immunoglobulin3.
Immune hemolytic anemia starts within 7-14 days and usually selflimits within 6 to 8 weeks after transplantation. However, cases in which the hemolytic condition lasted up to 6 months8 have been described.
In the presented case the appearance of a hemolytic anemia raised some diagnostic hypotheses namely the possibility of a posttransplant thrombotic microangiopathy or an immune-mediated hemolytic anemia associated to immunosuppressive drugs as tacrolimus or ATG.
As rhesus (Rh) antigens are not expressed on kidney tissue cell surfaces, matching for Rh antigens is not relevant in most settings but the possible occurrence of an Rh associated PBLS should have been kept in mind.
Transfusion with donor-type RBC is recommended in these cases until the TAD gets negative.
The patient had several postoperative complications demanding 2 surgical re-interventions and the need of multiple transfusions.
Hence, Rh positive RBCs increased immune stimulation and an exuberant anamnestic response by the donor memory B lymphocytes, leading to a severe hemolytic anemia. At that time, the presence of high title anti-D was documented and confirmed the diagnosis of PBLS. Afterwards an appropriate transfusion protocol with Rh negative RBCs was established but the hemolytic condition persisted for over 3 months.
The factors that contributed to the clinical severity in this case were the presence of previous sensitization and alloimmunization in the donor and the need for multiple transfusions in the recipient in the first 2 weeks after transplantation. We question whether it wouldn’t be opportune to transfuse these patients with Rh negative RBC since the day of surgery, regardless of the DAT result, as recommended in hematopoietic stem cell transplantation.
Besides transfusion with donor-type RBC, other therapeutics are available in PBLS namely steroids, plasmapheresis and rituximab2,3.
Rituximab is an anti-CD20 monoclonal antibody and its role in preventing PBLS has been well documented in allogenic stem cell transplantation.
A recent paper from Tsujimura and colleagues14 evaluated the efficacy of rituximab in preventing PBLS in 85 patients treated with ABO mismatched KT during a period of 8 years. None of the patients treated with rituximab had PBLS so the monoclonal antibody seems to be efficacious in inhibiting B lymphocytes proliferation.
The present case points out that PBLS should be considered in the presence of Rh incompatibility in the donor/recipient pair when DAT+ hemolytic anemia occurs. It is a potentially serious clinical condition and requires a prompt diagnosis and treatment, being particularly important the transfusion management with Rh negative RBCs.
References
1. Ainsworth CD, Crowther MA, Treleaven D, Evanovitch D, Webert KE, Blajchman MA. Severe haemolytic anemia post-renal transplantation produced by donor anti-D passenger lymphocytes: case report and literature review. Transfus Med Rev 2009; 23(2):115-159 [ Links ]
2. ElAnsary M, Hanna MO, Saadi G, et al.; Passenger lymphocyte syndrome in ABO and Rhesus D minor mismatched liver and kidney transplantation: a prospective analysis. Human immunology 2015; 76:447–452 [ Links ]
3. Nadarajah L, Ashman N,Thuraisingham R, Barber C, Allard S, Green L. Literature review of passenger lymphocyte syndrome following renal transplantation and two case reports. American journal of Transplantation 2013; 13:1594–1600 [ Links ]
4. Prosser AC, Kallies A, Lucas M. Tissue-Resident Lymphocytes in Solid Organ Transplantation: Innocent Passengers or the Key to Organ Transplant Survival? Transplantation 2018; 102(3):378–386 [ Links ]
5. Arul R, Dhanaprija J, Dinesh KT, Sakthirajan R, Balasubramaniyan T, Gopalakrishnan N. Passenger lymphocyte syndrome in a Renal Transplant Recipient- a case report Journal of renal medicine 2017; 1:1–6 [ Links ]
6. Pascual-Perez V, Gomez-Larrambe N, Collantes-Mateos R, Manzanos T, Urbizu-Gallardo JM. Passenger lymphocyte syndrome: an uncommon form of anaemia in renal transplantation. Nefrologia 2013; 33(4):615–616 [ Links ]
7. Karanth P, Birchall J, Day S, Unsworth DJ, Ravanan R. Immune hemolysis resulting from passenger lymphocyte syndrome derived anti-rh(D) reactivity after kidney transplantation: a case report and literature review. Transplantation 2014; 97(9):e54–55 [ Links ]
8. Schwartz D, Gotzinger P. Immune-haemolytic anaemia (IHA) after solid organ transplantation due to rhesus antibodies of donor origin: Report of 5 cases. Beitr Infusionsther 1992; 30:367–369 [ Links ]
9. Gonzalez-Molina M, Cabello M, Uyonarte S, Frutos MA, Martin Reyes G, Lopez de Novales E. Haemolytic anemia in renal transplant patients treated with cyclosporin A. Nefrologia 1988; 8:380–383 [ Links ]
10. Ramsey G, Israel L, Lindsay GD, Mayer TK, Nusbacher J. Anti-Rho (D) in two Rh-positive patients receiving kidney grafts from an Rh-immunized donor. Transplantation 1986; 41:67–69 [ Links ]
11. Solheim BG, Albrechtsen D, Egeland T, et al. Auto-antibodies against erythrocytes in transplant patients produced by donor lymphocytes. Transplant Proc 1987; 19:4520–4521 [ Links ]
12. Frohn C, Jabs WJ, Fricke L, Goerg S. Hemolytic anemia after kidney transplantation: Case report and differential diagnosis. Ann Hematol 2002; 81:158–160 [ Links ]
13. Pomper GJ, Joseph RA, Hartmann EL, Rohr MS, Adams PL, Stratta RJ. Massive immune hemolysis caused by anti-D after dual kidney transplantation. Am J Transplant 2005; 5:2586–2589 [ Links ]
14. Tsujimura K, Ishida H, Tanabe K. Is Efficacy of the Anti-Cd20 Antibody Rituximab Preventing Hemolysis Due to Passenger Lymphocyte Syndrome? Ther Apher Dial. 2017 Feb;21(1):22–25 [ Links ]
Marika Bini Antunes, MD
Serviço de Hematologia Clínica, Centro Hospitalar Universitário do Porto
Rua Dom Manuel II, 4099-001, Porto, Portugal
Email: marikabiniantunes@gmail.com
Disclosure of potential conflicts of interest: none declared.
Received for publication: Jan 28
Accepted in revised form: Jan 28


{kind=link}
{kind=link}