










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkNascer e Crescer
versão impressa ISSN 0872-0754versão On-line ISSN 2183-9417
Nascer e Crescer vol.26 no.1 Porto mar. 2017
EDITORIAL
Cardiac preparticipation screening for the young athlete: still a matter of controversy
Sílvia ÁlvaresI
I Cardiology Department of Centro Materno Infantil do Porto, Centro Hospitalar do Porto. 4099-001 Porto, Portugal. silvia.c.alvares@gmail.com
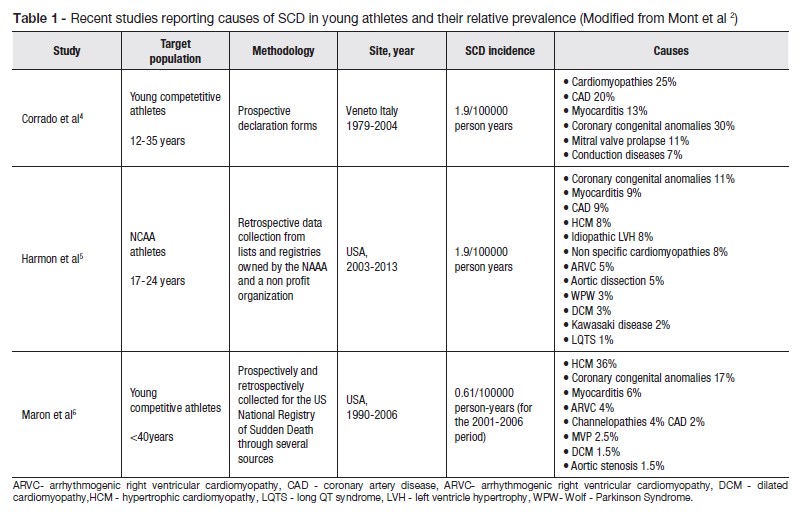
Regular physical activity is recommended as part of cardiovascular prevention and reduction of cardiovascular morbidity and mortality. However, vigorous exertion may increase the risk of sudden cardiac death in predisposed individuals: the risk of sudden cardiac death (SCD) is 2to 3-fold higher in athletes compared to nonathletes.1 Most of these events in the young athletes less than 35 years are due to malignant tachyarrhythmias, usually ventricular fibrillation (VF) or ventricular tachycardia (VT) degenerating into VF, occurring in individuals with arrhythmogenic disorders (e.g. hypertrophic cardiomyopathy, arrhythmogenic cardiomyopathy, channelopathies).2 Although the incidence of SCD is not accurately known, it is estimated in 0.5 and 1 per 100 000 below the age of 35 years. A comprehensive literature search review by Harmon et al found that this incidence is probably underestimated, which may imply the need of more effective prevention strategies.3 The causes of cardiac sudden death in the different series also depend on the characteristics of the population studied (age and geographical localization) (table 1).2
It is generally accepted that screening to detect potential diseases and prevent sudden death is justified and potentially beneficial. The strategies of screening are different across the countries. A medical detailed history (personal and family history to exclude genetic diseases) and a thorough physical examination are the basis of the evaluation for sports participation. Various protocols of preparticipation evaluation have been developed. In Portugal the questionnaire form can be assessed at the site of Instituto Português de Juventude e Desporto (Portuguese Institute of Sport and Youth); the Portuguese screening includes the history and physical examination, an ECG and a thorax X-ray.
The inclusion of the ECG to identify athletes at risk is still a matter of debate and controversy. The European Society of Cardiology recommends the addition of the ECG on the basis that medical history and physical examination alone have a limited ability to detect potentially lethal cardiac conditions, often silent. The ECG can manifest abnormalities in cardiomyopathies or channelopathies and contribute to the early recognition of these diseases.2,4,7
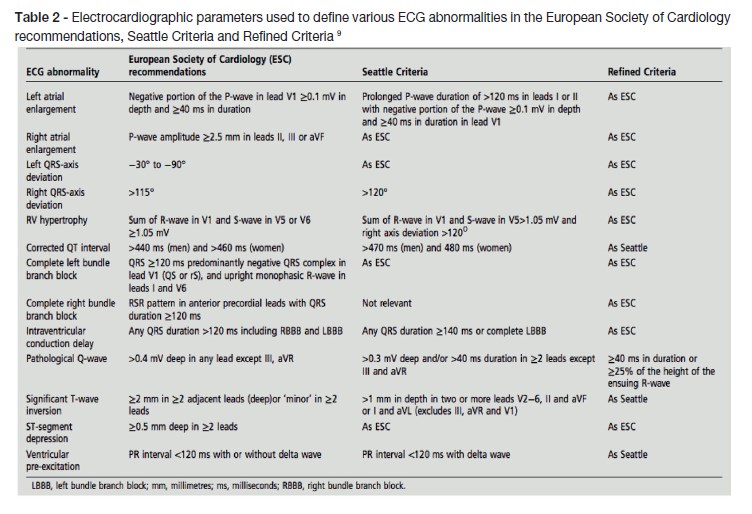
This argument is supported by a recent meta analysis of available studies comparing screening strategies (history, physical examination and ECG) that demonstrated the efficacy of the twelve lead ECG in the detection of cardiac disease.8 The use of modern criteria for interpretation of the ECG has reduced the number of false positives and the associated cost of further investigation (table 2).9-11
The ESC statement does not recommend the use of transthoracic echocardiography as a first line of screening or other imaging techniques. Exercise ECG test should be reserved for symptomatic athletes or those presenting high risk of CAD. The ambulatory ECG recording remains a second-line test. The most common indications for ambulatory ECG monitoring are unexplained syncope and palpitations, the investigation of bradyarrhythmias, to quantify premature ventricular contractions (PVC) density after initial prepraticipation tests or to assess QT in patients with suspected LQTS.2
The recommendations of the American Heart Association (AHA) for preparticipation screening for cardiovascular disease includes a comprehensive personal/family history and physical examination, using the AHAs 14-point screening guidelines or those of other societies, such as the American Academy of Pediatrics Preparticipation Physical Evaluation (the latter available at http://www.aap.org/PPE).12 Mandatory and universal mass screening with 12-lead ECGs in large general populations of young healthy people 12 to 25 years of age is not recommended for athletes and nonathletes. The reasons for this position are based mainly on the low incidence of SCD, the difficulties in the interpretation of the ECG and the false negative and false positive results, depending on the criteria used and in cost-efficacy considerations.
No screening program is able to prevent sudden cardiac arrest/death (SCA/SCD) completely. To improve outcomes other preventive measures should be taken, namely an emergency action plan (EAP) and access to an automated external defibrillator (AED). Personal in schools, clubs and sports organizations should have training in cardiopulmonary resuscitation.13,14
In summary, cardiac preparticipation screening for the young athlete is still a matter of controversy. The goal of cardiovascular screening of athletes is to detect cardiac conditions predisposing to SCD. The addition of 12-lead ECG to the clinical history and physical examination demonstrates to have superior diagnostic capability than just clinical history and physical examination. The ECG should be interpreted with modern standards that distinguish normal findings related to physiological cardiac remodelling in trained athletes from abnormalities associated to cardiac disease.
However, no screening program provides absolute protection against sudden cardiac arrest/death (SCA/SCD); an emergency action plan and access to an automated external defibrillator are essential to improve outcomes from SCA in athletes.
REFERENCES
1. Schmied C, Borjesson M. Sudden cardiac death in athletes. J Intern Med 2014; 275: 93–103 doi: 10.1111/joim.12184 [ Links ]
2. Mont L, Pelliccia A, SharmaS et al. Pre-participation cardiovascular evaluation for athletic participants to prevent sudden death: position paper from the EHRA and the EACPR, Q2 Q3 branches of the ESC. Endorsed by APHRS, HRS, and SOLAECE. Europace 2017; 19: 139-63. doi:https://doi.org/10.1093/europace/euw243 [ Links ]
3. Harmon KG, Drezner JA, Wilson MG, Sharma S. Incidence of sudden cardiac death in athletes: a state-of-the-art review. Heart 2014;100: 1227 – 34. [ Links ]
4. Corrado D, Basso C, Pavei A, Michieli P, Schiavon M, Thiene G. Trends in sudden cardiovascular death in young competitive athletes after implementation of a preparticipation screening program. JAMA. 2006;296: 1593–601 [ Links ]
5. Harmon KG, Asif IM, Maleszewski JJ, Owens DS, Prutkin JM, Salerno JC, et al. Incidence, etiology, and comparative frequency of sudden cardiac death in NCAA athletes: a decade in review. Circulation 2015; 132:10–9 [ Links ]
6. Maron BJ, Doerer JJ, Haas TS, Tierney DM, Mueller FO. Sudden deaths in young competitive athletes: analysis of 1866 deaths in the United States, 1980–2006. Circulation 2009; 119: 1085–92 [ Links ]
7. Corrado D, Pelliccia A, Bjornstad HH, et al. Cardiovascular pre-participation screening of young competitive athletes for prevention of sudden death: proposal for a common European protocol. Consensus Statement of the Study Group of Sport Cardiology of the Working Group of Cardiac Rehabilitation and Exercise Physiology and the Working Group of Myocardial and Pericardial Diseases of the European Society of Cardiology. Eur Heart J 2005;26:516–24. doi:10.1093/eurheartj/ehi108 [ Links ]
8. Harmon KG, Zigman M, Drezner JA. The effectiveness of screening history, physical exam, and ECG to detect potentially lethal cardiac disorders in athletes: a systematic review/meta-analysis. J Electrocardiol 2015; 48:329 – 38. [ Links ]
9. Drezner JA, Ackerman MJ, Anderson J, Ashley E, Asplund CA, Baggish AL, et al. Electrocardiographic interpretation in athletes: the Seattle criteria. Br J Sports Med. 2013;47:122-4. [ Links ]
10. Sheikh N, Papadakis M, Ghani S, Zaidi A, Gati S, Adami PE, Carré F, Schnell F, Wilson M, Avila P, McKenna W, Sharma S. Comparison of electrocardiographic criteria for detection of cardiac abnormalities in elite black and white athletes. Circulation. 2014;129:1637-49. [ Links ]
11. Riding NR, Sheikh N, Adamuz C, Watt V, Farooq A, Whyte GP, et al. Comparison of three current sets of electrocardiographic interpretation criteria for use in screening athletes Heart 2015;101:384–90. doi:10.1136/heartjnl-2014-306437 [ Links ]
12. Maron BJ, Levine BD, Washington RL, et al. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: Task Force 2: preparticipation screening for cardiovascular disease in competitive athletes: a Scientific Statement From the American Heart Association and American College of Cardiology. J Am Coll Cardiol 2015;66: 2356–61. doi:10.1016/j.jacc.2015.09.034 [ Links ]
13. Drezner JA, OConnor FG, Harmon KG et al . AMSSM Position Statement on Cardiovascular Preparticipation Screening in Athletes: Current Evidence, Knowledge Gaps, Recommendations, and Future Directions Clin J Sport Med 2016;26: 347–61. [ Links ]
14. Hainline B, Drezner J, Baggish A, et al. Interassociation consensus statement on cardiovascular care of college student-athletes. Br J Sports Med 2017;51: 74–85. [ Links ]


{kind=link}
{kind=link}