










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkNascer e Crescer
versão impressa ISSN 0872-0754versão On-line ISSN 2183-9417
Nascer e Crescer vol.27 no.1 Porto mar. 2018
EDITORIAL
Prevention of cardiovascular diseases starts in childhood
Sílvia ÁlvaresI
I Editor-in-Chief of NASCER E CRESCER – Birth and Growth Medical Journal; Department of Pediatric Cardiology, Centro Materno Infantil do Norte, Centro Hospitalar do Porto. 4099-001 Porto, Portugal. silviaalvares.dia@chporto.min-saude.pt
Atherosclerotic cardiovascular disease is still the major cause of death worldwide. The understanding of the development of atherosclerosis is essential to define prevention strategies. Autopsy and epidemiological studies have shown that this process starts early in childhood. Also the Bogalusa Heart Study and the Pathobiological Determinants of Atherosclerosis in Youth (PDAY) confirmed the presence of atherosclerotic plaques in adolescents and an association with risk factors namely increased body mass index(BMI), blood pressure, LDL-Cholesterol(C), low level of HDL-Cholesterol, diabetes mellitus and cigarette smoking. Non-invasive measures of atherosclerosis in pediatric population (carotid-intima-medial thickness and arterial distensibility) reached similar conclusions. These results appoint to the need of prevention strategies starting in childhood. There is growing evidence that health status and well-being are influenced by several aspects, namely genetics factors (30%), health care (10%), social and environmental factors (20%), and individual behaviours (40%). This means that the development of cardiovascular disease has its origins in families, and that approaches to prevention should address the developing child and adolescent and their family environment, namely health life styles.
Interventions in paediatric age, especially in children with identifiable risk factors (e.g., obesity, hypertension, diabetes mellitus, Kawasaki disease) are important in promoting cardiovascular health. Paediatric cardiologists, paediatricians and family physicians should be aware of their responsibility in cardiovascular prevention and play an active role in interventions to reduce risk factors fostering behaviour changes in an integrated perspective. Risk factors for atherosclerotic disease include dietary habits, physical activity, blood pressure, smoking/tobacco exposure, lipid and lipoprotein levels. Recently, other factors like sleep habits, stress management or depression have emerged as conditions associated with accelerated atherosclerosis. We also know that adult behaviour is conditioned by habits acquired during childhood and that use of medication will not fully eliminate cardiovascular risk, thus interventions in paediatric age are an important issue in the promotion of health and well-being.
Strategies for a better health status in adulthood include general measures to achieve health life styles, and identification and management of the child at risk for early atherosclerosis.
Screening for cardiovascular risk is recommended during routine health supervision, concerning: 1. family history, 2. diet, 3. physical activity, 4. leisure time TV/video/computer use, 5. tobacco exposure. Blood pressure (BP) should be measured in every visit in children older than 3 years; younger children need a regular BP assessment if there is a positive history of neonatal complications, congenital heart disease, urinary/renal abnormality, solid-organ transplant, malignancy, medications, or condition known to raise BP or increase intracranial pressure. Promotion of breast feeding and a diet low in saturated fat starting at age 1 year is recommended. Advocate a diet rich in fruits, vegetables, whole grains, low-fat/fat-free milk and milk products; lower in sugar and salt; with a total fat 30% of daily kcal/EER[1], saturated fat 8-10% of daily kcal/EER, monounsaturated and polyunsaturated fat up to 20% of daily kcal/EER; avoid trans fat as much as possible. Encourage moderate-to-vigorous physical activity every day and limit daily leisure screen time (TV/video/computer): no TV in childs bedroom, limit total media time to no more than 1-2 hours of quality programming per day. Advocate for a smoke-free home environment, counsel parents/ adolescents strongly about not smoking, providing explicit information about the addictive and adverse health effects of smoking or specific smoking cessation guidance.
The National Heart, Lung and Blood Institute (NHLBI), part of the National Institutes of Health, and the American Academy of Pediatrics (AAP) recommend lipid screening in all children at least once between the ages of 9 and 11 years, and again between ages 17 and 21 years. This represents a significant change from the previous guidelines (The NCEP Expert Panel on Blood Cholesterol Levels in Children and Adolescents, 1992), that advised for screening only children with a family history of heart disease (parent, grandparent, aunt, uncle, or sibling with heart attack, treated angina, CABG/stent/angioplasty, stroke, or sudden cardiac death at < 55 y in males, < 65 y in females) or high cholesterol.
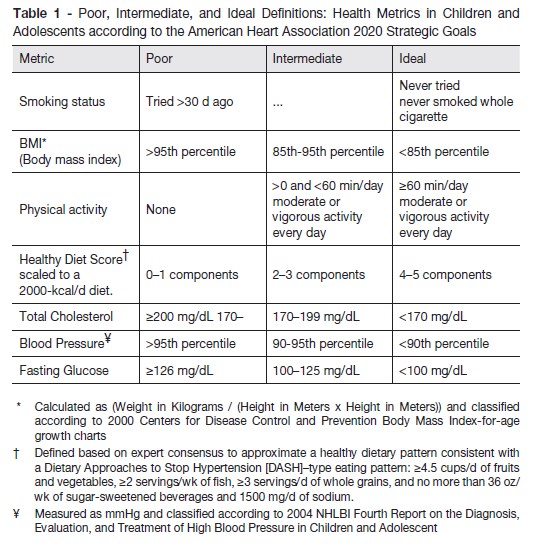
The statement of the American Heart Association (AHA): Cardiovascular Health Promotion in Children-Challenges and Opportunities for 2020 and Beyond, discusses two important factors: the promotion of ideal cardiovascular health in all children and the improvement of cardiovascular health metric scores in children currently classified as having poor or intermediate cardiovascular health. The ideal cardiovascular health status is based in health behaviors: (1) never smoked; (2) body mass index below the 85th percentile; (3) at least 60 minutes per day of moderate or vigorous physical activity; and (4) a healthy diet score, and also (1) total cholesterol less than 170mg/dL; (2) blood pressure below the 90th percentile; and (3) fasting blood glucose less than 100 mg/dL (table 1).
Most of the used strategies for cardiovascular prevention are based on education and behaviour change methodology through educational materials and self-monitoring questionnaires, teaching in clinics, schools or other community environments. The possibility of using computerized technology or web – based interventions has also been introduced with favourable outcomes. More research is needed in this area, as well the evaluation of cost effectiveness of this type of interventions. Nevertheless, it seems an appealing strategy to implement in this population particularly comfortable with the new technologies.
Cardiovascular health in the adult starts early in infancy, and population and individual-level approaches to promote health behaviours are essential. A comprehensive strategy is necessary involving patients, healthcare providers, professional organizations, community, schools, media outlets, and government agencies to protect individual peoples health and quality of life
REFERENCES
-
GBD 2013 Mortality and Causes of Death Collaborators. 2015. Global, regional, and national age–sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the global burden of disease study 2013. Lancet 385:117–1.
-
Li S, Chen W, Srinivasan SR, Bond MG, Tang R, Urbina EM, Berenson GS. Childhood cardiovascular risk factors and carotid vascular changes in adulthood: the Bogalusa Heart Study. JAMA. 2003; 290:2271–6. doi:10.1001/jama.290.17.227
-
Gidding SS, Rana JS, Prendergast C, et al. Pathobiological Determinants of Atherosclerosis in Youth (PDAY) Risk Score in Young Adults Predicts Coronary Artery and Abdominal Aorta Calcium in Middle Age: The CARDIA Study. Circulation. 2016; 133:139-46.
-
Berenson GS, Bogalusa Heart Study Investigators Bogalusa Heart Study: a long-term community study of a rural biracial (Black/White) population. Am J Med Sci. 2001; 322:293-300.
-
McMahan CA, McGill HC, Gidding SS, Malcom GT, Newman WP, Tracy RE, et al. PDAY risk score predicts advanced coronary artery atherosclerosis in middle-aged persons as well as youth Atherosclerosis. 2007; 190:370-7. Epub 2006 Mar 10.
-
American Academy of Pediatrics. Reports of the expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents. Pediatrics. 2011;128: S213–56
-
Oliveira FL, Patin RV, Escrivão MA. Atherosclerosis prevention and treatment in children and adolescents. Expert Rev Cardiovasc Ther. 2010; 8:513–28.
-
Imperatore G, Boyle JP, Thompson TJ, Case D, Dabelea D, Hamman RF, et al. Projections of type 1 and type 2 diabetes burden in the U.S. population aged <20 years through 2050: dynamic modeling of incidence, mortality, and population growth Diabetes Care. 2012; 35:2515-20.
-
Steinberger J, Daniels SR, Hagberg N, Isasi CR, Kelly AS, Lloyd-Jones D, et al; on behalf of the American Heart Association Atherosclerosis, Hypertension, and Obesity in the Young Committee of the Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; Council on Epidemiology and Prevention; Council on Genomic and Precision Medicine; and Stroke Council. Cardiovascular health promotion in children: challenges and opportunities for 2020 and beyond: a scientific statement from the American Heart Association [published online ahead of print August 11, 2016]. Circulation, 2016; 134: e236-55.
-
Kavey RE, Allada V, Daniels SR, Hayman LL, McCrindle BW, Newburger JW, et al. Cardiovascular risk reduction in high-risk pediatric patients: a scientific statement from the American Heart Association Expert Panel on Population and Prevention Science; the Councils on Cardiovascular Disease in the Young, Epidemiology and Prevention, Nutrition, Physical Activity and Metabolism, High Blood Pressure Research, Cardiovascular Nursing, and the Kidney in Heart Disease; and the Interdisciplinary Working Group on Quality of Care and Outcomes Research: endorsed by the American Academy of Pediatrics Circulation. 2006;114(24):2710-38.
-
Petersen KS, Kris-Etherton PM. Prevention of cardiovascular disease starts in childhood. Commentary, National Academy of Medicine, Washington, DC.
-
Available at: https://nam.edu/wp-content/uploads/2017/05/Prevention-of-Cardiovascular-Disease-Starts-in-Childhood.pdf.
-
Pacor JM, Younus A, Malik R, Osondu CU, Aziz M, Ogunmoroti O, et al. Prevalence of ideal cardiovascular health metrics in children and adolescents: A systematic review. Progress in Pediatric Cardiology 2016; 43:141–6
-
Pahkala K, Hietalampi H, Laitinen TT, Viikari JSA, Rönnemaa T, Niinikoski H, et al. Ideal cardiovascular health in adolescence: Effect of lifestyle intervention and association with vascular intima-media thickness and elasticity (The Special Turku Coronary Risk Factor Intervention Project for children [STRIP] study). Circulation 2013; 127:20–96.
-
Shay CM, Gooding HS, Murillo R, Foraker R. Understanding and improving cardiovascular health: An update on the American Heart Associations concept of cardiovascular health. Progress in Cardiovascular Diseases 2015; 58:41–9.
-
Chamberland K, Sanchez M, Panahi S, Provencher V, Gagnon J, Drapeau V. The impact of an innovative web-based school nutrition intervention to increase fruits and vegetables and milk and alternatives in adolescents: a clustered randomized trial International Journal of Behavioral Nutrition and Physical Activity 2017; 14:140-51
-
Chung RJ, Touloumtzis C, Gooding H, Staying Young at Heart: Cardiovascular Disease Prevention in Adolescents and Young Adults. Curr Treat Options Cardiovasc Med. 2015; 17: 61.
NOTES
[1] EER- Estimated Energy Requirements/d for age/gender

