










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkNascer e Crescer
versão impressa ISSN 0872-0754versão On-line ISSN 2183-9417
Nascer e Crescer vol.27 no.3 Porto set. 2018
https://doi.org/10.25753/BirthGrowthMJ.v27.i3.13190
CASE REPORTS | CASOS CLÍNICOS
Acromicric dysplasia and hearing loss: A case report
Displasia acromícrica e alterações auditivas: A propósito de um caso clínico
Ana Nóbrega PintoI; Miguel Bebiano CoutinhoI; Teresa SoaresI; Cecília Almeida SousaI
I Department of Otorhinolaryngology and Cervical-Facial Surgery, Centro Hospitalar do Porto. 4099-001 Porto, Portugal. ananobregapinto@gmail.com; coutinho.mb@gmail.com; teresa.soares.costa@gmail.com; director.orl@hgsa.min-saude.pt
Correspondence to
ABSTRACT
Introduction: Acromicric dysplasia is an extremely rare autosomal dominant bone dysplasia characterized by progressive growth retardation, short hands and feet, mild facial dysmorphism and generalized joint limitation. Association with ear, nose and pharyngolaryngeal alterations has been previously reported. However, little is known about the otolaryngologic aspects that may accompany this disease. We pretend to raise awareness to the otolaryngologic aspects that may accompany acromicric dysplasia and to the possible interventions that improve these patients quality of life.
Clinical Case: We present the case of a ten-year-old girl referred to the otorhinolaryngology consultation with complaints of progressive hearing loss. Hearing evaluation confirmed bilateral severe mixed hearing loss and the patient was successfully rehabilitated with bone-anchored hearing aids.
Discussion/Conclusions: Evaluation by an otolaryngologist should be part of the management of children with bone dysplasias, especially if they present with associated symptoms, to allow an early diagnosis and proper intervention.
Keywords: Bone dysplasias; hearing loss, hearing impairment rehabilitation
RESUMO
Introdução: A displasia acromícrica é uma displasia óssea extremamente rara, de transmissão autossómica dominante, caracterizada por atraso progressivo do crescimento, mãos e pés curtos, dismorfismo facial ligeiro e limitação generalizada do movimento das articulações. A associação com alterações nos ouvidos, nariz, faringe e laringe foi descrita em estudos prévios. No entanto, pouco se sabe sobre os aspectos otorrinolaringológicos que podem acompanhar esta doença. Pretende-se sensibilizar para os aspectos otorrinolaringológicos que podem acompanhar a displasia acromícrica e para as possíveis intervenções que melhoram a qualidade de vida destes doentes.
Caso Clínico: Apresentamos o caso de uma criança do sexo feminino, de dez anos de idade, referenciada à consulta de otorrinolaringologia por noção de diminuição progressiva da audição. A avaliação auditiva confirmou a existência de uma hipoacusia de mista severa bilateral e a doente foi reabilitada com sucesso com um implante osteointegrado.
Discussão/Conclusões: A observação por um otorrinolaringologista deve fazer parte da avaliação de crianças com displasias ósseas, especialmente se apresentam sintomas associados, para permitir um diagnóstico precoce e uma intervenção adequada.
Palavras-Chave: Doenças do Desenvolvimento Ósseo; hipoacusia; reabilitação auditiva
INTRODUCTION
The evaluation of children with bone dysplasias is often directed to the associated morphological and radiological alterations. However, many of these patients present with otolaryngological complaints that should be taken into account. Acromicric dysplasia (AD) is an extremely rare autosomal dominant bone dysplasia (prevalence <1/1 000 000) first described by Maroteaux et al. in 1986.1 The genetic cause of AD was shown to be heterozygous mutations in the transforming growth factor (TGF) β-binding protein-like domain 5 of the fibrillin 1 gene (FBN1).2
AD is characterized by a postnatal and progressive growth retardation resulting in short stature with a pseudomuscular build, short hands and feet, mild facial dysmorphism, generalized joint limitation and skin thickening. It is associated with some distinctive skeletal and radiologic features, such as delayed bone age, short metacarpals and phalanges, cone-shaped epiphyses, ovoid vertebral bodies and internal notch of femoral head.3-5
Less than sixty cases have been reported in the literature to date. In these cases, association with ear, nose and pharyngeal-laryngeal alterations has been reported.3-5 However, little is known about the otolaryngologic aspects that may accompany this disease.
CASE DESCRIPTION
A ten-year-old girl, diagnosed with acromicric dysplasia, was referred to the otolaryngology consultation with complaints of progressive hearing loss. The diagnosis of AD was clinically suspected by the distinctive clinical and radiological features that the patient presented (growth retardation with short stature and short limbs, brachydactyly with broad thumbs, partial syndactyly of 3rd and 4th fingers of both feet and short metacarpals and phalanges in x-ray) and was genetically confirmed by molecular analysis of the FBN1 gene. There was no familiar history.
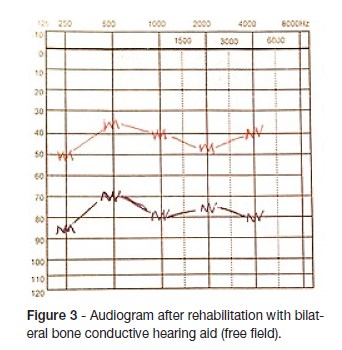
Physical examination showed a mild facial dysmorphia (figure 1) and low implantation of both ears with bilateral moderate stenosis of the external auditory canals. The audiogram revealed a bilateral severe mixed hearing loss (figure 2). She had a history of adenoidectomy and myringotomy with placement of transtympanic ventilation tubes at five years of age, with no hearing improvement. A CT scan was performed and revealed a class two middle ear malformation (Cremers classification).5
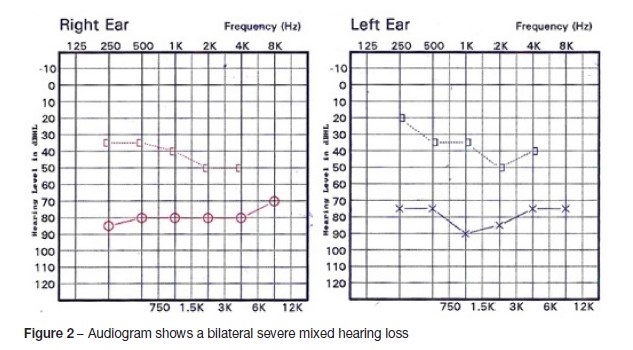
She was successfully rehabilitated with a bone-anchored hearing aid (BAHA®) in the right ear at age 11. A few years later the parents and the patient decided to place a bone-anchored hearing aid (BAHA®) in the left ear, which resulted in additional gain (figure 3).
DISCUSSION
Acromicric dysplasia is characterized by a short stature and distinctive skeletal abnormalities with normal intellectual development. Otolaryngological alterations, such as a hoarse voice and recurrent ear, tracheal and respiratory infections (such as otitis and other upper respiratory infections) have been associated with this disorder.4
The pathogenesis of this disease is related with heterozygous FBN1 mutations that are all located in exons 41 and 42 and encode TGFβ-binding protein-like domain 5 of FBN1 gene. Microfibrillar network disorganization and enhanced TGFβ signaling were consistent features in AD fibroblasts. This mutation is also associated with other disorders that present with short stature phenotypes (like geleophysic dysplasia) and with Marfan syndrome.2,5
Diagnosis is based on the typical skeletal and radiological alterations and is confirmed by molecular study of the FBN1 gene.2-5
Life expectancy of these patients is normal and no major complications, such as cardiac disease or major orthopedic problems, were described in the course of the disease.4 Nonetheless long-term follow-up of AD requires an orthopedic surveillance and annual clinical and radiological assessment is recommended.3
In terms of hearing loss rehabilitation, the bone anchored hearing aids and the conventional hearing aids are good options. In this case, with the bilateral external canal stenosis, the bone anchored hearing aid was decided and had excellent audiological results. This intervention significantly improved this patient quality of life, allowing her to continue her potential for a normal cognitive development.
Evaluation by an otolaryngologist should be part of the management of children with bone dysplasias, especially if they present with associated symptoms (hearing loss, recurrent infections and airway obstruction) to allow an early diagnosis and proper intervention.
With this clinical case the authors expect to raise awareness to the otolaryngologic aspects that may accompany this rare disease and to the possible interventions that undoubtedly improve these patients quality of life.
REFERENCES
1. Maroteaux P, Stanescu R, Stanescu V, Rappaport R. Acromicric dysplasia. Am J Med Genet 1986; 24:447-9. [ Links ]
2. Le Goff C, Mahaut C, Wang LW, Allali S, Abhyankar A, et al. Mutations in the TGFbeta binding-protein-like domain 5 of FBN1 are responsible for acromicric and geleophysic dysplasias. Am J Hum Genet 2011; 89:7–14. [ Links ]
3. Klein C, Le Goff C, Topouchian V, Odent S, Violas P, Glorion C, et al. 2014. Orthopedics management of acromicric dysplasia: follow up of nine patients. Am J Med Genet Part A. 2014; 164A:331-7. [ Links ]
4. Faivre L, Merrer M, Baumann C, Polak M, Chatelain P, Sulmont V, et al. Acromicric dysplasia: long term outcome and evidence of autosomal dominant inheritance. J Med Genet 2001; 38:745-9. [ Links ]
5. Hasegawa K, Numakura C, Tanaka H, Furujo M, Kubo T, Higuchi Y, et al. Three cases of Japanese acromicric/geleophysic dysplasia with FBN1 mutations: a comparison of clinical and radiological features. J Pediatr Endocrinol Metab. 2017; 30:117-21. [ Links ]
6. Teunissen EB, Cremers WR. Classification of congenital middle ear anomalies. Report on 144 ears. Ann Oto Rhinol Laryngol. 1993. 1002(8Pt1):606-12. [ Links ]
CORRESPONDENCE TO
Ana Nóbrega Pinto
Department of Otorhinolaryngology
and Cervical-Facial Surgery
Centro Hospitalar do Porto
Largo Professor Abel Salazar
4099-001 Porto
Email: ananobregapinto@gmail.com
Received for publication: 03.10.2017
Accepted in revised form: 26.10.2017


{kind=link}