










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkNascer e Crescer
versão impressa ISSN 0872-0754versão On-line ISSN 2183-9417
Nascer e Crescer vol.28 no.4 Porto dez. 2019
https://doi.org/10.25753/BirthGrowthMJ.v28.i4.15413
CASE REPORTS | CASOS CLÍNICOS
Case of swyer-james-macleod syndrome diagnosed in adolescence
Um caso de síndrome de swyer-james-macleod diagnosticado na adolescência
Rosa-Anita FernandesI, Leonor CunhaII, Marília LoureiroIII, Isabel RezendeII, Sílvia ÁlvaresIII, Helena FalcãoII
I Immunoallergology Unit. Hospital Pedro Hispano - Unidade Local de Saúde de Matosinhos. 4464-513 Matosinhos, Portugal. rosa.fernandes.alergo@gmail.com
II Department of Immunoallergology, Centro Hospitalar Universitário do Porto. 4099-001 Porto, Portugal. leonorcunhagraca@sapo.pt; isabelrezende26@gmail.com; falcao.helena@gmail.com
III Department of Pediatric Cardiology, Centro Materno-Infantil do Norte, Centro Hospitalar Universitário do Porto. 4050-651 Porto, Portugal. lmarilia.loureiro@gmail.com; silviaalvares.dia@chporto.min-saude.pt
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
Swyer-James-MacLeod syndrome, or unilateral hyperlucent lung syndrome, is a rare entity associated with post-infectious bronchiolitis. Clinical presentation may include recurrent chest infections or exertional dyspnea, or it may result from an incidental finding following chest X-ray. Treatment is usually individualized and ranges from conservative management to surgical intervention.
Here in is described the case of a 17-year-old boy with a history of asthma and allergic rhinitis, who was diagnosed with Swyer-JamesMacLeod syndrome in the context of a respiratory infection and careful chest x-ray examination.
This case highlights the importance of raising awareness and accurately recognizing this rare entity, in order to optimally manage patients and avoid unnecessary treatment.
Keywords: adolescent; asthma; hyperlucent lung; Swyer-James-MacLeod syndrome
RESUMO
A Síndrome de Swyer-James-MacLeod, ou pulmão hiperlucente unilateral, é uma entidade rara associada a bronquiolite pós-infeciosa. Pode manifestar-se através de infeção recorrente ou dispneia de esforço, ou constituir um achado acidental após radiografia torácica. A sua abordagem terapêutica é individualizada, variando entre tratamento conservador e abordagem cirúrgica.
Os autores descrevem o caso de um adolescente de 17 anos com antecedentes de asma e rinite alérgica, a quem foi diagnosticada síndrome de Swyer-James-MacLeod no contexto de uma infeção respiratória após análise detalhada de raio-X torácico.
Este caso evidencia a raridade desta patologia e a importância de a reconhecer precocemente, abordando-a de uma forma ótima e evitando tratamentos desnecessários.
Palavras-chave: adolescente; asma; pulmão hiperlucente; síndrome de Swyer-James-MacLeod
Introduction
Swyer-James-MacLeod syndrome (SJMS), or unilateral hyperlucent lung syndrome, is a rare entity characterized by hyperlucency of one lung, lobe, or part of a lobe.1 It was first described by Swyer and James in 1953, and in 1954 Macleod observed patients with the same characteristics, giving the syndrome its current designation.2,3 It is currently considered an acquired condition, secondary to viral bronchiolitis or pneumonitis in childhood.4 The most commonly implicated etiological agents include adenovirus types 3, 7, and 21, but also paramyxovirus, Bordetella pertussis, Mycobacterium, Mycoplasma, Influenzae, Streptococcus pneumoniae, and S. aureus.5 Most patients have unilateral involvement of the left lung.6 The condition is typically diagnosed during childhood after evaluation for recurrent respiratory infection, but diagnosis may also be established during adulthood, as some patients with little or no sequelae bronchiectasis have minor or even no symptoms.4
Case presentation
The authors describe the case of a 17-year-old adolescent with a diagnosis of asthma and allergic rhinitis to pollens, observed in the Immunoallergology clinic with complaints of fever with three days of evolution, nasal obstruction and discharge, cough with cough with sputum, and dyspnea.
At the age of two, the boy had been hospitalized due to severe pulmonary infection, and adenovirus was isolated from respiratory secretions. Since then, he displayed normal growth, with weight and height in P50-75, and reported transient rhinitis complaints (especially during spring) and bronchial symptoms in the context of lower airway infections. The boy had been regularly followed and was diagnosed with asthma and mild intermittent allergic rhinitis to pollens. He was chronically medicated with inhaled budesonide 200 μg twice a day, terbutaline 500 μg as relief therapy, and desloratadine 5 mg.
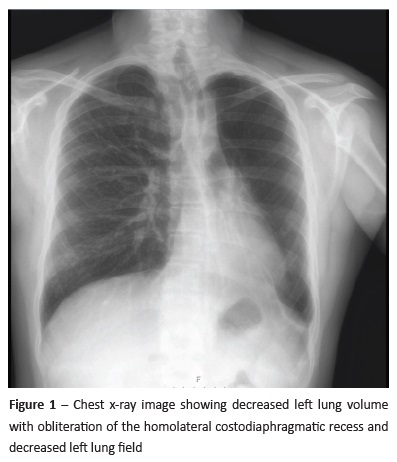
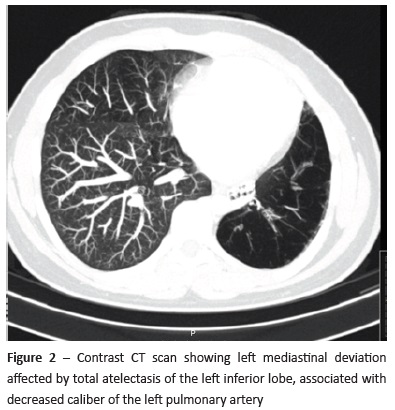
Physical examination revealed decreased respiratory sounds in the left lung and mild expiratory wheezing, with normal cardiac sounds. Transcutaneous oxygen saturation was normal. Body mass index was 22.9 kg/m2 (P50-75). No other changes were found (e.g. digital clubbing). Complete blood count (erythrocytes 5.21x106/ μL, leucocytes 11.34x103/μL, and platelet count 351x103/μL) and comprehensive metabolic panel analysis (creatinine 0.40 mg/ dL, blood urea nitrogen 29.7 mg/dL, glucose 87 mg/dL) were unremarkable. Chest x-ray showed a leftward mediastinal shift and decreased left lung field and volume, with obliteration of the homolateral costodiaphragmatic recess and hyperinflation of the right lobe (Figure 1). Contrast CT scan revealed left mediastinal deviation, conditioned by total atelectasis of the left inferior lobe, with ramification preservation and permeability of the main bronchus, associated with a decreased caliber of the left pulmonary artery. In the left apical region, fibrotic alterations were observed, and the right lung showed compensatory hyperinflation (Figure 2).
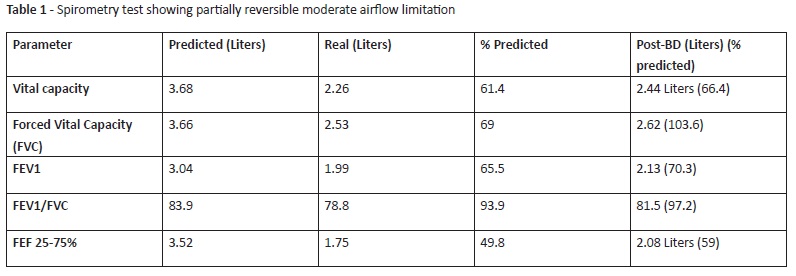
Spirometry revealed reversible airflow limitation (Table 1).
In cardiac study, two D/Doppler echocardiogram revealed mild dilation of the right cavities with trivial tricuspid insufficiency, with an estimated 35 mmHg pressure in the right ventricle, and electrocardiogram showed a ventricular preexcitation pattern, confirmed by 24-hour cardiac monitoring. Cardiac catheterization showed hypoplasia of the left pulmonary artery, with normal pulmonary pressure.
On the basis of clinical findings and imaging studies, the boy was diagnosed with SJMS. Due to alterations observed in spirometry, conservative management comprised treatment with inhaled budesonide 200 μg twice a day. Influenza and pneumococcal vaccines were administered.
Discussion
SJMS is currently considered an acquired condition resulting from infectious insults during infancy or childhood.5 The infectious agent originates an inflammatory response, which causes obliteration of peripheral airways in the infected lung. Long-term effects on the lung include destruction of the alveoli and dilation of the pulmonary parenchyma. Early infection results in destruction of bronchioles with subsequent fibrosis, compromising development of the alveolar bud. Such lung underdevelopment causes poor air intake, together with the classic imaging findings herein observed on the affected lungs.7 Pulmonary vasculature is hypoplastic, while lungs distal to the diseased bronchioles become hyperinflated, with pan-acinar emphysematous changes in some cases.1
This syndrome is quite heterogeneous. Most cases are diagnosed during childhood and the usual presentation involves recurrent chest infections.6 Less common clinical presentations include productive cough, wheezing, hemoptysis, and exertional dyspnea.5 Similarly to most SJMS cases, the present patient presented with intermittent dyspnea that was repeatedly interpreted as bronchial asthma exacerbations, with diagnosis established after an acute febrile episode that prompt chest x-ray examination.
SJMS diagnosis is based on imaging findings. Radiological study modalities usually include chest x-ray, high-resolution CT scan (HRCT), angiography, magnetic resonance angiography, angiography, and V/Q scanning.5 Characteristic radiographic findings include unilateral hyperlucent lungs with decreased broncho-vascular markings, small hilar shadow, and slight mediastinum displacement to the affected side. On CT scan, persistently low attenuation of lung tissue in the affected regions at end exhalation is common. Bronchiectasis, bronchiolectasis, atelectasis, and scarring are also observed. Pulmonary angiography can reveal hypoplasia and diminished size of the affected pulmonary artery.1 A classical triad has been described, which confirms diagnosis: unilateral hyperlucent lung, diffusely decreased ventilation, and matching decreased perfusion in the affected lung.8
In the present case, chest x-ray provided the first highly suggestive indication of this clinical entity, with HRCT confirming diagnosis. Total atelectasis of the left inferior lobe could have prompted a bronchoscopy to remove secretions and improve pulmonary re-expansion, but the parents refused the procedure due to its invasiveness and the only mild symptoms displayed by the boy.
Treatment is individualized, ranging from conservative management to surgical intervention. A conservative symptomatic approach is the mainstay of treatment, managing current and preventing future pulmonary infections.5 Chest physiotherapy, low-dose inhaled corticosteroids, and inhaled bronchodilators can be used. Influenza and pneumococcal vaccines should be administered. Surgical intervention should be considered for patients with repeated infections who do not respond to optimal medical management. Pneumectomy is the most common intervention, but some patients can be treated with lobectomy or segmentectomy.1
Bronchiectasis is the most common SJMS sequela, present in up to 78% of cases, but lung abscesses and spontaneous pneumothorax have also been reported. Both clinical manifestations and prognosis are affected by the presence and type of bronchiectasis, with the worst prognosis associated with saccular form.5 Long-term complications in adulthood include hemoptysis and pulmonary hypertension.9 There are currently no studies regarding morbidity and mortality associated with this syndrome.10
In this patient, absence of bronchiectasis in CT scan was a good prognostic sign. However, continuous follow-up with regular symptom and pulmonary function evaluation is recommended. Early and targeted treatment of pulmonary infections is key, as well as prophylaxis with influenza and pneumococcal vaccines.
This case emphasizes the relevance of a thorough chest x-ray examination while evaluating a patient with a history of recurrent respiratory symptoms. This is particularly true in cases with a history of severe respiratory infections at a young age with symptom onset thereafter. Although most cases are diagnosed in childhood, diagnosis may be missed until adolescence or adulthood in patients with little or no symptoms. In the present patient, despite numerous observations, SJMS was not diagnosed until a complementary imaging study was performed. It should be emphasized that, in cases of asthma irresponsive to standard treatment, a HRCT should be performed to exclude alternative diagnoses. SJMS should, therefore, be considered in the differential diagnosis of patients with unilateral hyperlucent lung and prompt appropriate treatment and follow-up.
REFERENCES
1. Dirweesh A, Alvarez C, Khan M, Shah N. A unilateral hyperlucent lung - Swyer-James syndrome: A case report and literature review. Respir Med Case Reports. 2017; 20:104-6. [ Links ]
2. Swyer PR, James G. A case of unilateral pulmonary emphysema. Thorax. 1953; 8:133-6. [ Links ]
3. MacLeod WM. Abnormal transradiancy of one lung. Thorax. 1954; 9:147-53. [ Links ]
4. Capela C, Gouveia P, Sousa M, Regadas M. Adult diagnosis of Swyer-James-McLeod syndrome: a case report. J Med Case Rep. 2011; 5:2. [ Links ]
5. Mehra S, Basnayake T, Falhammar H, Heraganahally S, Tripathi S. Swyer-James-MacLeod syndrome-a rare diagnosis presented through two adult patients. Respirol Case Reports. 2017;5:1-5. [ Links ]
6. Abba A, Al-Mobeireek A. Clinical spectrum of Swyer-JamesMacLeod syndrome in adults. Saudi Med J. 2003; 24:195-8. [ Links ]
7. Chaucer B, Chevenon M, Toro C, Lemma T, Grageda M. SwyerJames-MacLeod syndrome: a rare finding and important differential in the ED setting. Am Journal Emerg Med. 2016; 34:1329.e3-e4. [ Links ]
8. Wojcicki K, Sindel A, Berry A, Krieger R, Reuther W. An uncommon obliterative lung disease: Swyer-James-McLeod syndrome. Intern Emerg Med. 2015; 10:881-2. [ Links ]
9. Machado D, Lima F, Marques C, Monteiro R. Swyer-JamesMacleod syndrome as a rare cause of unilateral hyperlucent lung: Three case reports. Medicine (Baltimore). 2019; 98:e14269. [ Links ]
10. Turcu D, Dupa S, Turcanu A, Mihaescu T. A Case of Unilateral Hyperlucency of the Lung: a Rare Adult Occurrence of SwyerJames-MacLeod Syndrome. Maedica (Buchar). 2018; 13:143-6. [ Links ]
Endereço para correspondência | Dirección para correspondencia | Correspondence
Rosa-Anita Fernandes
Immunoallergology Unit
Hospital Pedro Hispano
Unidade Local de Saúde de Matosinhos
Rua Dr. Eduardo Torres
4464-513 Senhora da Hora
Email: rosa.fernandes.alergo@gmail.com
Received for publication: 10.11.2018
Accepted in revised form: 15.03.2019

