










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkNascer e Crescer
versão impressa ISSN 0872-0754versão On-line ISSN 2183-9417
Nascer e Crescer vol.29 no.1 Porto jan. 2020
https://doi.org/10.25753/BirthGrowthMJ.v29.i1.17978
REVIEW ARTICLES | ARTIGOS DE REVISÃO
What role for the pacifier in acute otitis media risk?
Qual o papel da chupeta no risco de otite média aguda?
Joana Silva PeixotoI, Cíntia Cardal FrançaI, Sílvio BargeI; Mariana BrancoII
I. General and Family Medicine, Unidade de Saúde Familiar Mais Saúde, Unidade Local de Saúde do Alto Minho. 4990-084 Ponte de Lima, Portugal. joana.speixoto@gmail.com; cintia_franca90@hotmail.com; silvioanjos80@gmail.com
II. Department of Pediatrics, Unidade Local de Saúde do Alto Minho. 4904-858 Viana do Castelo, Portugal. mariana.a.branco@hotmail.com
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
Introduction: Sucking reflex is acknowledged as a comforting mechanism for infants. When used for short periods of time, it is considered a healthy habit. Acute otitis media is one of the most frequent infections in pediatric age and has been associated with pacifier misuse.
Objectives: To review available evidence regarding the association between pacifier use in the first years of life and otitis media risk.
Methods: A literature search was conducted on several databases using MeSH terms “otitis” and “pacifiers” for guidelines, systematic reviews, randomized controlled trials, and observational studies over the last 20 years. SORT scale of the American Family Physician was used to evaluate evidence levels.
Results: A total of 56 articles were retrieved, of which four guidelines, one systematic review, and one original article were selected. According to guidelines, there is no reason to discourage pacifier use, as it can be particularly beneficial in the first six months of life. Afterwards, pacifier use should be limited to moments of falling asleep. Its use should also be avoided in infants with chronic or recurrent otitis media. The systematic review stablished pacifier use as a risk factor for recurrent acute otitis media (RAOM) which is susceptible to intervention. In the observational study, a statistically significant association was found between pacifier use and RAOM risk.
Conclusions: Pacifier use should not be actively discouraged in the first semester of life, as it can have beneficial effects for children (SORT A). Afterwards, its use should be discontinued due to increased otitis risk (SORT A).
Keywords: child; otitis; pacifier; review
RESUMO
Introdução: O reflexo de sucção é reconhecido como um mecanismo de conforto usado pelo lactente. A utilização de chupeta é considerada benéfica quando efetuada por curtos períodos de tempo. A otite média aguda é uma das infeções mais frequentes em idade pediátrica e tem sido associada ao uso indevido deste objeto.
Objetivos: Rever a evidência científica publicada sobre a associação entre utilização de chupeta nos primeiros anos de vida e risco de otite.
Metodologia: Foi efetuada uma revisão da literatura em várias bases de dados utilizando os termos MeSH “otitis” e “pacifiers”, tendo sido pesquisadas orientações, revisões sistemáticas, ensaios clínicos aleatorizados e estudos observacionais publicados nos últimos 20 anos. Foi utilizada a escala SORT da American Family Physician para avaliar os níveis de evidência.
Resultados: No total, foram identificados 56 artigos, dos quais foram selecionadas quatro orientações, uma revisão sistemática e um artigo original. De acordo com as orientações, não existe motivo para desencorajar o uso de chupeta, que pode ter efeitos protetores nos pequenos lactentes. A sua utilização deve ser descontinuada a partir do segundo semestre de vida, limitando-a aos momentos de adormecer, e deve ser evitada em crianças com antecedentes de otite. A revisão sistemática estabeleceu o uso de chupeta como fator de risco para otite média aguda recorrente (OMAR) passível de intervenção. O estudo observacional encontrou uma associação estatisticamente significativa entre o uso de chupeta e risco de OMAR.
Conclusões: O uso de chupeta não deve ser desencorajado no primeiro semestre de vida, pois pode ter efeitos benéficos para as crianças (SORT A). A partir do segundo semestre, o seu uso deve ser descontinuado devido ao risco crescente de otite média aguda (SORT A).
Palavras-chave: criança; otite; chupeta; revisão
Introduction
Nonnutritive sucking is a natural reflex for newborns and babies and is recognized as a comforting mechanism. Pacifier has been used as a method for fulfilling this innate desire. When used for short periods of time, it is considered a healthy routine; however, its prolonged use is detrimental.1
Historically, pacifiers were considered beneficial until the early 1900s, when an anti-pacifier movement spread concerns about their use leading to poor hygiene and indulgent behavior.2 Although nearly 80% of children in Western countries use pacifiers, the benefit of its use is not duly stablished at present.3
Pacifiers have multiple benefits, including analgesic effects, shorter preterm infant hospitalizations, and lower risk of sudden infant death syndrome (SIDS).4-6 Pacifier has been recommended for pain relief in newborns and infants undergoing minor Emergency Department procedures, such as heel sticks, immunization, and venipuncture.4 The benefits of its use are also documented in preterm infants regarding an improved earlier transition from enteral to bottle feeding.7 The American Academy of Pediatrics guidelines suggest offering infants pacifiers at the onset of sleep to reduce SIDS risk.6 Although the exact mechanism underlying reduction in SIDS rates is not fully understood, pacifier use may decrease the likelihood of rolling into prone position, increase arousal, and maintain airway patency. It also decreases gastroesophageal reflux and resulting sleep apnea.8
Potential complications of pacifier use include negative impact on breastfeeding, dental malocclusion, and otitis media and are more frequent with prolonged use. Pacifier use may be associated with early breast weaning or be a marker of breastfeeding difficulties; therefore, it should be avoided until breastfeeding is well established (usually by the age of one month).9,10
Although adverse dental effects may occur after the age of two years, they are more significant after the age of four. Therefore, pacifier use should be discouraged after this age.11,12
Acute otitis media (AOM) is one of the most frequent infections in pediatric age and has been associated with pacifier use. Although pacifier use does not increase the risk of respiratory infections, the mechanism by which it predisposes to AOM is not understood.13 A direct association has been reported between pacifier use frequency and AOM risk, with the main theory suggesting a pressure equilibrium alteration between the middle ear cavity and nasopharynx, with Eustachian tube function impairment.
The aim of this study was to review available evidence regarding an association between pacifier use in the first years of life and otitis media risk.
Methods
A literature search was conducted in February 2019 on several databases using the MeSH terms “otitis” and “pacifiers”. Searched databases included the National Guideline Clearinghouse, the National Health Service (NHS) Electronic Library, Cochrane Library, Database of Abstracts of Reviews of Effectiveness (DARE), Bandolier, Canadian Medical Association, the Portuguese Health Authority (DGS) database, and PubMed.
Retrieved publication types included guidelines, systematic reviews (SR) and meta-analyses (MA), randomized controlled trials (RCT), and observational studies published over the last 20 years in Portuguese, English, or Spanish language. Articles were selected if meeting the following criteria: a) population: children up to five years old; b) exposure: pacifier use; c) comparison: no pacifier use; and d) outcome: presence of AOM or recurrent otitis. Studies were excluded if not meeting inclusion criteria, diverging from the study purpose, representing duplicates, or having been included in a MA or SR.
The Strength of Recommendation Taxonomy (SORT) scale of the American Family Physician was used to assign evidence levels (EL) and assess the strength of recommendations (SR).
Results
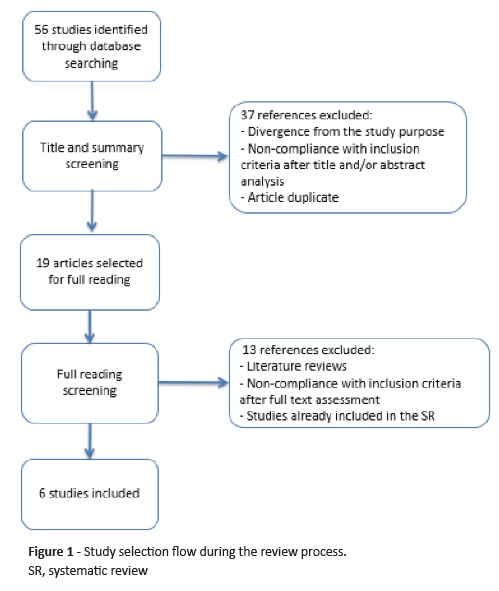
Article selection flow is depicted on Figure 1. Search strategy retrieved 56 articles, six of which met pre-defined inclusion criteria and were included in the analysis: one original article, one systematic review, and four guidelines.
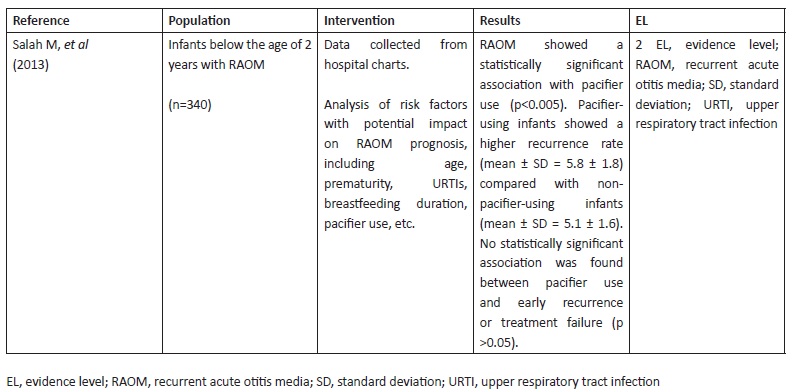
Mohamed Salah et al published a retrospective study in 2013 analysing risk factors for recurrent AOM (RAOM). RAOM was defined as three or more AOM episodes over a six-month period. The study included 340 infants below the age of two years diagnosed with RAOM, 73 (21.5%) of which were pacifier users. Data was collected from parent-fulfilled hospital charts documenting children’s medical history. In the study, RAOM was shown to have a statistically significant association with pacifier use (p <0.005). Pacifier-using children showed a higher RAOM recurrence rate (mean ± standard deviation [SD] = 5.8 ± 1.8) compared with non-pacifier-using children (mean ± SD = 5.1 ± 1.6). Early recurrence was defined as evidence of AOM signs and symptoms one month after initial improvement and treatment failure was defined as acute infection persistence or worsening for up to one week following initial treatment. The authors found no statistically significant association between pacifier use and early recurrence or treatment failure (p >0.05).14
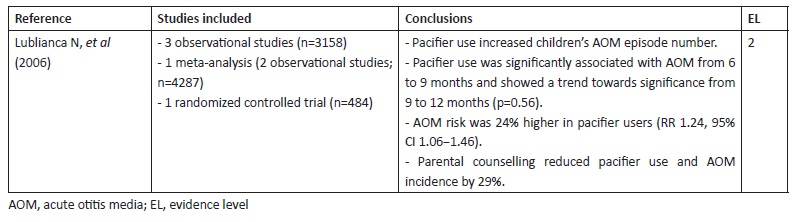
The systematic review by Lubianca Neto et al analysed evidence about modifiable risk factors for AOM and RAOM in children. In this study, RAOM was defined as three or more AOM episodes during a six-month period or at least four AOM episodes during 12 months. The authors searched MEDLINE for studies published from January 1966 to July 2005 using no language restriction and the descriptors “acute otitis media/risk factors” and included three observational studies, one MA, and one RCT addressing pacifier use as a risk factor for otitis media in infants.15 In one study, pacifier use was significantly associated with AOM development from the sixth to the ninth months of life (p<0.05) and showed a strong trend towards statistical significance in the period from nine to twelve months (p=0.056).16 According to Niemela et al, pacifier use was significantly associated with otitis media (relative risk [RR] 1.48, p=0.01, 95% confidence interval [CI] 1.08−2.02).17 In a prospective study, the same authors investigated a group of 845 children and concluded that pacifier use increased the annual incidence of AOM and was responsible for 25% of AOM cases.13 In the MA by Uhari et al, pacifier use increased AOM relative risk by 24% (RR 1.24; 95% CI 1.06−1.46).18 In the RCT conducted by Niemela et al, study intervention consisted in parental counselling regarding pacifier use, with parents advised not to use pacifier in children after the age of six months. At the end of the study, AOM prevalence in the intervention group decreased 29%. Children consistently not using pacifier in both intervention and placebo groups displayed 33% less AOM episodes. These results suggest that restricted pacifier use, limited to falling asleep moments, has the potential to reduce AOM risk and that its use should be limited to the first ten months of life, when sucking need is more pronounced and AOM risk is lower (EL 2).3
The expert panel responsible for the Italian Guidelines for AOM management recommends that infants should reduce pacifier use to the minimum (SORT A).19 Experts base their recommendation on two studies: the previously described SR from Lubianca Neto et al and the cohort study from Rovers et al.15,20 The last was performed as part of the Utrecht Health Project, which followed 495 children aged between zero and four years between 2000 and 2005. Parents filled a baseline questionnaire regarding pacifier use and potential confounders and AOM was diagnosed by general practitioners. Overall, 35% of pacifier-using children and 32% of non-pacifier-using children developed at least one AOM episode and 16% and 11% developed recurrent AOM (defined as three or more AOM episodes during the study period), respectively. The adjusted odds ratio (OR) for the correlation between pacifier use and AOM and recurrent AOM was 1.3 (95% CI 0.9−1.9) and 1.9 (95% CI 1.1−3.2), respectively.20
The Canadian Pediatric Society guidelines acknowledge pacifier use as a risk factor for otitis media, although other factors are implicated in the condition’s pathogenesis.21 The risk is proportional to use duration and frequency. Therefore, infants and children with chronic or recurrent otitis media should have a limited pacifier use (SORT A).21 One study showed that pacifiers were free of the major otitis media-causing pathogens and almost 50% of recently used pacifiers were uncontaminated.22 In another study, pacifier sucking was reported in 40% of 601 children with chronic otitis media requiring tympanostomy tubes in Toronto, Ontario.23
The same guidelines state that pacifier use is a significant risk factor for AOM, based on the previously described prospective study of children in day care centers and in the MA of otitis media risk factors.13,18 One survey to parents of children aged 12 months or younger also found an otitis media risk twice as high in pacifier users.24 This study was limited by the definition of pacifier use to more than five hours per day and by parental reporting reliability. A similar study also based on parental reporting found a higher otitis media prevalence in pacifier users (OR 1.20).16
The joint recommendations of the American Academy of Family Physicians/American Academy of Pediatrics are based on the previous studies by Niemela, Uhari, and Rovers.3,18,20 These guidelines recommend reducing or stopping pacifier use in the second six months of life to reduce otitis media risk (SORT B).7,25
In 2014, the Portuguese Health Authority (DGS) issued recommendations about AOM diagnosis and treatment in pediatric age, with pacifier use identified as one of the risk factors for AOM in healthy children.26
Discussion
One of the concerns associated with pacifier commonly expressed by parents is how long it can be used without harm to the infant. This review aimed to address this question using the most up-to-date information and evidence-based medical publications.
One of this study’s limitations is the fact that the systematic review included was based on a limited number of studies, all of which with more than ten years. Most included studies had an observational and retrospective design, allowing only to establish associations and not causality relations. On the other hand, data was based on parental reporting, which is subject to memory bias and not as accurate as physician reporting. Another study limitation is the acknowledgment that pacifier use is not the only factor implicated in AOM development, with other factors potentially involved. The role of pacifier in AOM development seems to be proportional to the time and frequency of use.
Given these facts, further studies are required to draw more robust conclusions about this subject.
Conclusion
Given available evidence, pacifier use should not be actively discouraged in the first six months of life, as it can have beneficial effects (SORT A). Nevertheless, it should be avoided until breastfeeding is well stablished. Following the second six months of life, pacifier use should be discontinued due to the higher risk of AOM (SORT A).
Observational study
(clique para ampliar ! click to enlarge)
Systematic review
(clique para ampliar ! click to enlarge)
Guidelines

(clique para ampliar ! click to enlarge)
REFERENCES
1. Levin S. Dummies. S Afr Med J. 1971; 45:237-40. [ Links ]
2. Gale CR, Martyn CN. Dummies and the health of Hertfordshire infants, 1911-1930. Soc Hist Med. 1995; 8:231-55. [ Links ]
3. Niemelä M, Pihakari O, Pokka T, Uhari M. Pacifier as a risk factor for acute otitis media: A randomized, controlled trial of parental counseling. Pediatrics. 2000; 106:483-8. [ Links ]
4. Zempsky WT, Cravero JP, American Academy of Pediatrics Committee on Pediatric Emergency M, Section on A, Pain M. Relief of pain and anxiety in pediatric patients in emergency medical systems. Pediatrics. 2004; 114:1348-56. [ Links ]
5. Pinelli J, Symington A. Non-nutritive sucking for promoting physiologic stability and nutrition in preterm infants. Cochrane Database Syst Rev. 2005:CD001071. [ Links ]
6. American Academy of Pediatrics Task Force on Sudden Infant Death S. The changing concept of sudden infant death syndrome: diagnostic coding shifts, controversies regarding the sleeping environment, and new variables to consider in reducing risk. Pediatrics. 2005; 116:1245-55. [ Links ]
7. Sexton S, Natale R. Risks and benefits of pacifiers. Am Fam Physician. 2009; 79:681-5. [ Links ]
8. Hauck FR, Omojokun OO, Siadaty MS. Do pacifiers reduce the risk of sudden infant death syndrome? A meta-analysis. Pediatrics. 2005; 116:e716-23. [ Links ]
9. Gartner LM, Morton J, Lawrence RA, Naylor AJ, O’Hare D, Schanler RJ, et al. Breastfeeding and the use of human milk. Pediatrics. 2005; 115:496-506. [ Links ]
10. Salone LR, Vann WF Jr, Dee DL. Breastfeeding: An overview of oral and general health benefits. The Journal of the American Dental Association. 2013; 144:143-51.
11. American Dental association. For the dental patient. Thumb sucking and pacifier use. The Journal of the American Dental Association. 2007; 138:1176. [ Links ]
12. Niemela M, Uhari M, Mottonen M. A pacifier increases the risk of recurrent acute otitis media in children in day care centers. Pediatrics. 1995; 96:884-8. [ Links ]
13. Salah M, Abdel-Aziz M, Al-Farok A, Jebrini A. Recurrent acute otitis media in infants: analysis of risk factors. Int J Pediatr Otorhinolaryngol. 2013; 77:1665-9. [ Links ]
14. Lubianca Neto JF, Hemb L, Silva DB. Systematic literature review of modifiable risk factors for recurrent acute otitis media in childhood. J Pediatr (Rio J). 2006; 82:87-96. [ Links ]
15. Warren JJ, Levy SM, Kirchner HL, Nowak AJ, Bergus GR. Pacifier use and the occurrence of otitis media in the first year of life. Pediatric Dentistry. 2001; 23:103-7. [ Links ]
16. Niemelä M, Uhari M, Hannuksela A. Pacifiers and dental structure as risk factors for otitis media. Int J Pediatr Otorhinolaryngol. 1994; 29:121-7. [ Links ]
17. Uhari M, Mäntysaari K, Niemelä M. A meta-analytic review of the risk factors for acute otitis media. Clin Infect Dis. 1996; 22:1079-83. [ Links ]
18. Marchisio P, Bellussi L, Di Mauro G, Doria M, Felisati G, Longhi R, et al. Acute otitis media: From diagnosis to prevention. Summary of the Italian guideline. Int J Pediatr Otorhinolaryngol. 2010; 74:1209-16. doi: 10.1016/j.ijporl.2010.08.016. [ Links ]
19. Rovers MM, Numans ME, Langenbach E, Grobbee DE, Verheij TJ, Schilder AG. Is pacifier use a risk factor for acute otitis media? A dynamic cohort study. Fam Pract. 2008; 25:233-6. [ Links ]
20. Canadian Paediatric Society. Recommendations for the use of pacifiers. Paediatr Child Health. 2003; 8:515-28. [ Links ]
21. Brook I, Gober AE. Bacterial colonization of pacifiers of infants with acute otitis media. The Journal of laryngology and otology. 1997;111:614-5. [ Links ]
22. Ford-Jones EL, Friedberg J, McGeer A, Simpson K, Croxford R, Willey B, et al. Microbiologic findings and risk factors for antimicrobial resistance at myringotomy for tympanostomy tube placement-a prospective study of 601 children in Toronto. Int J Pediatr Otorhinolaryngol. 2002; 66:227-42. [ Links ]
23. Jackson JM, Mourino AP. Pacifier use and otitis media in infants twelve months of age or younger. Pediatric dentistry. 1999; 21:255-60. [ Links ]
24. Subcommittee on Management of Acute Otitis Media. Diagnosis and Management of Acute Otitis Media. Pediatrics. 2004; 113:1451. [ Links ]
25. Direção Geral da Saúde. Diagnóstico e Tratamento da Otite Média Aguda na Idade Pediátrica. Recommendation 007/2012, updated in 28/10/2014. [ Links ]
Endereço para correspondência | Dirección para correspondencia | Correspondence
Joana Silva Peixoto
Unidade de Saúde Familiar Mais Saúde
Unidade Local de Saúde do Alto Minho
Rua da Cidade Châlette-sur-Loing, 67
4990-084 Ponte de Lima
Email: joana.speixoto@gmail.com
Received for publication: 07.06.2019
Accepted in revised form: 09.12.2019

