










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkNascer e Crescer
versão impressa ISSN 0872-0754versão On-line ISSN 2183-9417
Nascer e Crescer vol.29 no.3 Porto set. 2020
https://doi.org/10.25753/BirthGrowthMJ.v29.i3.17113
ORIGINAL ARTICLES | ARTIGOS ORIGINAIS
Characterization of the population of pregnant women attending a mental health service
Caracterização da população de mulheres grávidas seguidas num serviço de saúde mental
Tiago FerreiraI, Sara DehanovI, Catarina OliveiraI, Sara CastroI, Raquel RibeiroI, Teresa MaiaI
I Department of Mental Health, Hospital Prof. Doutor Fernando Fonseca. 2720-276 Amadora, Portugal. tiagofilipeferreira17@hotmail.com; sara.dehanov@gmail.com; catarinafpo@gmail.com; saralimacastro@gmail.com; raquel.bon.ribeiro@gmail.com; maria.t.correia@hff.min-saude.pt
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
Introduction: Psychopathological symptoms are common during pregnancy and their detection and referral to specialized care is often suboptimal. The aim of this study was to perform a descriptive analysis of sociodemographic, mental health, and obstetric features of a population of pregnant women followed at Psychiatry consultation.
Methodology: This was a cross-sectional, descriptive study of women followed both at Gynecology/Obstetrics and Psychiatry consultations of Hospital Prof. Doutor Fernando Fonseca between 2014 and 2016. A total of 76 women were included, for whom pre-defined features associated in the literature with risk of developing psychopathological symptoms during pregnancy were collected.
Results and Discussion: Risk factors identified in the development of depressive symptoms included absence of an affective relationship during pregnancy (n=11; 14.5%), being first-generation immigrant (n=17; 22.4%), and substance use before (n=18; 23.7%) or during (n=10; 13.1%) pregnancy. Sample was divided into women with previous Psychiatry follow-up who became pregnant (n=44; 57.9%) and women referred to Psychiatry consultation during pregnancy (n=32; 42.1%). In the second group, 18.8% (n=6) of referrals were from primary health care, being relevant to understand whether this represents an under-referral. Prescription of 21 risk category D drugs was identified, alerting to the need of caution in pharmacological prescription and of considering non-pharmacological options (e.g., cognitive-behavioral therapy) for management of these cases.
Conclusions: Risk factors identified in this study represent an opportunity to optimize clinical practice and improve these patients’ follow-up.
Keywords: health; perinatal care; pregnancy; psychopathology
RESUMO
Introdução: Alterações psicopatológicas são comuns durante a gravidez e a sua deteção e referenciação a cuidados especializados é frequentemente deficitária. O objetivo deste estudo foi efetuar uma análise descritiva de dados sociodemográficos, de saúde mental e obstétricos de uma amostra de grávidas em seguimento em consulta de Psiquiatria.
Material e Métodos: Este foi um estudo transversal e descritivo. A amostra foi selecionada por cruzamento dos processos de doentes com seguimento em consulta de Ginecologia/Obstetrícia e Psiquiatria no Hospital Prof. Doutor Fernando Fonseca entre 2014 e 2016. Foram obtidos 76 processos, tendo sido colhidas e analisadas variáveis previamente identificadas na literatura como estando associadas a risco de desenvolvimento de alterações psicopatológicas durante a gravidez.
Resultados e Discussão: Foram identificados fatores de risco para o desenvolvimento de sintomas depressivos, nomeadamente ausência de relacionamento afetivo durante a gestação (n=11; 14,5%), ser imigrante de 1ª geração (n=17; 22,4%) e consumos toxicofílicos antes (n=18; 23,7%) ou durante (n=10; 13,1%) a gravidez. A amostra foi dividida entre mulheres com acompanhamento pregresso em Psiquiatria que engravidaram (n=44; 57,9%) e mulheres referenciadas para consulta de Psiquiatria durante a gestação (n=32; 42,1%). Neste segundo grupo, 18,8% (n=6) das referenciações foram feitas a partir dos cuidados de saúde primários, sendo importante perceber se tal se trata de uma sub-referenciação. Foram prescritos 21 fármacos da categoria de risco D, o que alerta para a necessidade de precaução na prescrição farmacológica e de considerar alternativas não farmacológicas (e.g. terapia cognitivo-comportamental) na orientação destes casos.
Conclusões: Este estudo permitiu identificar fatores de risco para psicopatologia, representando uma oportunidade de otimizar a prática clínica e o seguimento destas doentes.
Palavras-chave: cuidados perinatais; gravidez; psicopatologia; saúde mental
Introduction
Psychopathological symptoms are common during pregnancy. According to the literature, prevalence of psychiatric illness among pregnant women in clinical samples varies from 15% to 29%.1 These values may correspond to underdiagnosis and to subsyndromal levels of psychopathology.1,2 Psychiatric disorders, specifically with anxious and depressive symptoms, may have repercussions in pregnant women in the form of more frequent and pronounced accessory symptoms (such as vomiting or nausea) and increased risk of obstetric complications. However, they may also affect the child via biological (e.g., hypothalamic-pituitary-adrenal axis) or relational and developmental (e.g., changes in mother-infant bonding pattern, delays in cognitive and motor development) effects.3-5
Follow-up of pregnant women with psychiatric illness poses multiple difficulties, including regarding pharmacotherapeutic options, given gestation-related contraindications, risk of medication interruption or non-acceptance, risk of psychiatric symptom relapse, and need for urgent intervention regarding mental health to avoid negative effects on mother and fetus. In addition, psychopathological symptoms often go unnoticed in prenatal exams, and follow-up is sometimes insufficient.4,6 Some explanatory hypotheses for this lack of detection and adherence are related to health service providers, including psychopathology underdetection in Primary Health Care (PHC) and Obstetric Services, lack of psychoeducational information for women, lack of knowledge or absence of a systematic approach from professionals, and fear of case mismanagement or bad practice.4,7,8 Some barriers to seeking screening and help are related to women themselves, such as preference to deal with mood problems on their own, fear of losing parental rights due to symptom disclosure, fear of medication, and not distinguishing which emotions are “normal” or not during pregnancy. Lack of family member involvement of other sources of social support can also hinder detection and treatment of mental health disorders.8,9 Additionally, economic (especially in low-income women), logistical, and cultural/linguistical barriers should also be considered.10
Several studies, mainly reviews and meta-analyses, have sought to untangle risk factors associated with development of anxious and depressive symptomatology during pregnancy. However, this association is more consistent in some studies than others. Absence of social support (especially from partners), stressful life events, personal or family psychiatric history, substance abuse, obstetric complications during pregnancy, and unplanned pregnancy have all been associated with depressive symptoms during pregnancy.4,5 Relevance of these factors in the population of pregnant women should be assessed, in order to plan targeted interventions.
Few studies are available in the literature describing psychopathology risk factors and how to refer and follow this group of patients. Therefore, the aim of this study was to conduct a descriptive analysis of sociodemographic, mental health, and obstetric features of a sample of pregnant women with follow-up both at Obstetrics and Psychiatry consultation of Hospital Prof. Doctor Fernando Fonseca (HFF), to investigate and improve knowledge about this patient population profile.
Methods
This was a cross-sectional and descriptive study. Sample was obtained by cross-selecting patients with follow-up both at Gynecology/Obstetrics and Psychiatry consultation of HFF between January 2014 and December 2016. Inclusion criteria comprised patients (1) with at least one gestation during the considered three-year period and (2) referred to Psychiatry consultation during pregnancy or with follow-up in Psychiatry before the beginning of pregnancy.
Pre-defined socio-demographic (age, nationality, marital status), mental health (substance abuse before and during pregnancy, family history of psychopathology [namely during pregnancy], psychiatric diagnosis, psychopathological symptoms, psychotherapeutic and psychopharmacological treatment), and obstetric (gravidity and parity, obstetric complications in the considered pregnancy, risk pregnancy, unplanned or unwanted pregnancy) data were collected and described.
Data was retrieved from clinical records of the first Gynecology/Obstetrics consultation and first Psychiatry consultation after pregnancy. To schematize data collection and description, sample was divided into a group of women with previous Psychiatry follow-up who became pregnant during the considered three-year period − Group 1 (G1) − and a group of women who were already pregnant at the time of Psychiatry referral during that same period − Group 2 (G2). In G1, data regarding socio-demographic and mental health features was retrieved from medical records of the first psychiatry consultation after pregnancy detection. In G2, the same data was retrieved from medical records of the first Psychiatry evaluation following referral. The only exception was that in G1 “substance abuse before pregnancy” data had to be verified in previous Psychiatry consultations.
Descriptive statistical analysis was performed using the Statistical Package for Social Sciences®, version 23 and Microsoft Excel 2016®. Absolute and relative frequencies were used as descriptive measures, and mean (M) and standard deviation (SD) as central tendency measures.
Results
Of 246 cases initially identified, 170 were excluded for not meeting inclusion criteria, namely for absence of at least one gestation during the considered time period or absence of psychiatric clinical data.
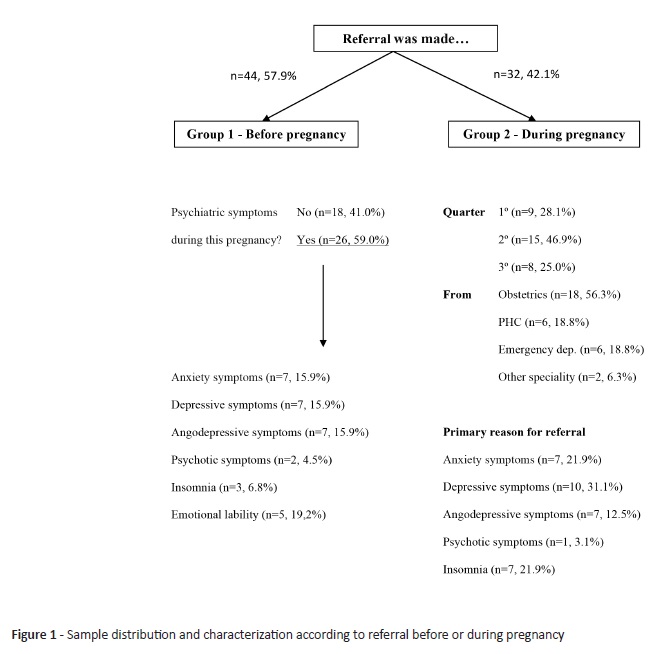
A total of 76 pregnant women were included in the study, with a mean (SD) age of 33.6 (±6.7) years. These were divided into two groups: women followed in Psychiatry before pregnancy (G1; n=44, 57.9%) and women referred to Psychiatry during pregnancy (G2; n=32, 42.1%; Figure 1).
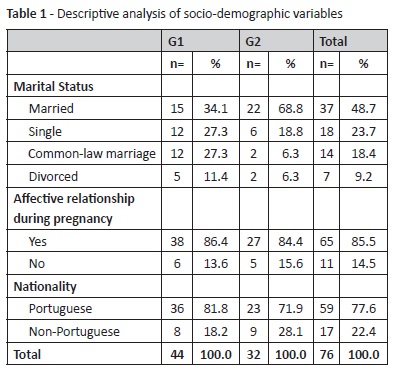
Socio-demographic data of the two groups is presented in Table 1. Regarding marital status, 37 women (37.0%) were married and 14 (18.4%) were in a common-law marriage. Although 25 women (32.9%) were single (n=18, 23.7%) or divorced (n=7, 9.2%), only 11 women (14.5%) denied having an affective relationship during pregnancy. Seventeen women (22.4%) were first-generation immigrants, while the remaining (n=59, 77.6%) had Portuguese nationality.
At least 18 women (23.7%) reported substance use before pregnancy (tobacco n=16, 23.7%; cannabinoids n=4, 5.3%; alcohol n=3, 3.9%; cocaine n=2, 2.6%; LSD n=1, 1.3%). This number reduced to ten women (13.1%) during pregnancy (tobacco n=10, 13.2%; cannabinoids n=2, 2.6%), corresponding to a 55.6% decrease in substance use.
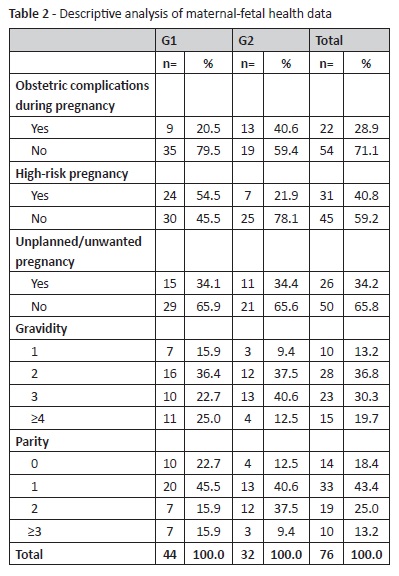
Obstetric health data is presented in Table 2, specifically obstetric complications during current pregnancy (n=22, 28.9%), classification as high-risk pregnancy (n=31, 40.8%), and occurrence of unplanned or unwanted pregnancies (n=26, 34.2%). Data regarding gravidity (M±DP 2.7±1.30) and parity (M±DP 1.4±1.12) is also presented. It should be noted that ten women were pregnant for the first time (13.2%) and 62 women were multiparous (81.6%).
Family history of psychiatric illness was established in 24 women (31.6%). However, presence or absence of family history of psychopathology during pregnancy was only registered in 14 clinical records (18.4%) and identified in two patients (2.6%). Thus, this information could not be retrieved from clinical records in 81.6% of cases (n=62).
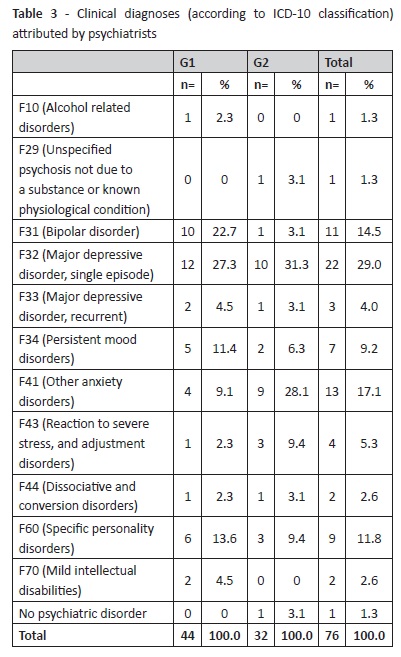
Table 3 depicts psychiatric diagnoses established by the psychiatrist according to ICD-10 classification. Most frequent diagnoses in G2 were depressive (n=10, 31.2%) and anxiety (n=9, 28.1%) disorders, such as panic disorder or generalized anxiety disorder. In G1, depressive episodes were also identified as the most frequent diagnosis (n=12, 27.3%), and bipolar affective disorder as the second most common diagnosis (n=10, 22.7%).
Regarding treatment, 59 women (77.6%) were already receiving or started pharmacotherapy (G1 n=32, 42.1%; G2 n=27, 35.5%) and 16 (21.1%) were receiving or started psychological counseling (G1 n=9, 11.8%; G2 n=7, 9.2%). A total of 88 different medications were prescribed in consultation, 21 (23.9%) of which were category D drugs (17 of which benzodiazepines).
Discussion
Results from this analysis identified risk factors for psychopathology in pregnant women. Some are potentially manageable through proper referral and health care surveillance.
These women’s family and social support during medical follow-up or through the help of other professionals is relevant and should be investigated. Lack of social support, poor relationship, or absence of a partner during pregnancy are frequently cited as possible risk factors for anxious or depressive symptoms.4,5 The percentage of women with no affective relationship in this sample was 14.5%. A study by Maia T (2014) that assessed determinants of mother-infant relationship in a sample of pregnant women (n=92) followed at PHC maternal health consultation in the same geographic area of the present study reported that 25.0% of women were single/separated, with a higher prevalence of depression in this subgroup.11 This value was higher in the present study (32.9%), reinforcing the urgent need for attention to these women.
In this study, the proportion of first-generation immigrant women (22.4%) was higher than the proportion of foreign women among hospital patients (8%).12 According to the literature, immigrant mothers have increased psychological vulnerability, particularly in the postpartum.13,14 A study by Almeida LM et al. (2016) found an increased risk of postpartum depression and lower satisfaction with social support among migrant mothers.14 In addition, disparities in psychopathology diagnostic and treatment rates in migrant women tend to occur, with cultural and linguistic barriers to access and continued health care as possible explanations.13 In the study by Maia T (2014), 34.8% of pregnant women were first-generation immigrants, and this was associated with a higher depression prevalence.11 Hence, the high representativeness of this subgroup in this study and its association with depressive symptomatology risk alerts to the need for particular focus on integration and follow-up of these women, namely at PHC.
In this study, the percentage of women with substance use during pregnancy was comparable to other studies (Cook et al., 2017) regarding tobacco (13.2% vs. 12-25%) and cannabinoid (2.6% vs. 1.8-16.6%) smoking, while alcohol and other illicit substance consumption was null.15 A 55.6% decrease in these consumptions was reported between the period before and during gestation (62.5% tobacco reduction, 50% cannabinoids reduction, and alcohol, cocaine, and LSD withdrawal). However, it is acknowledged that this reduction is not always maintained, with frequent relapses during postpartum. Substance use is one of risk factors with greater intervention potential, especially when compared to factors intrinsic to women and their family.5,15 Therefore, it should be a primary intervention target, with referral to specialized teams whenever necessary and appropriate psychoeducation during consultation. It should also be noted that retrieved figures may be underestimated due to women or physician underreporting.
Although family history of psychopathology can be perceived, its presence or absence during pregnancy was often not registered by clinicians in anamnesis. This factor should be considered when assessing psychopathology risk in pregnancy and postpartum, as some studies suggest that perinatal depression (and particularly postpartum depression) has a familial component.16 Thus, this data should be systematically collected during clinical practice consultations.
In this sample, 26 women (34.2%) admitted having an unwanted or unplanned pregnancy, what is associated with angodepressive symptomatology in the literature.4,5,17 Unwanted or unplanned pregnancies should be evaluated in clinical practice, as well as existence of social and economic support, as they will not necessarily translate into harmful consequences if properly managed.
A positive association between obstetric risk and depression rate is reported in the literature.4,17 In this sample, a high percentage of obstetric complications during pregnancy (n=22, 28.9%) and high-risk pregnancy (n=31, 40.8%) was uncovered. However, the bias intrinsic to “high-risk pregnancy” criteria should be considered. In the hospital where this data was collected, criteria for potential high-risk pregnancy includes being less than 18 or over 35 years old; presenting comorbid medical pathologies (arterial hypertension, diabetes, autoimmune disease, endocrine pathology, etc.); being previously followed at Psychiatry; and presenting placenta previa. Those women previously attend a screening visit, in which those who maintain high-risk patient classification during follow-up are selected. This process has intrinsic variability, and the high percentage of high-risk pregnancies in G1 (54.5%) and proportion of women referred from obstetrics in G2 possibly reflect this.
The association between parity and psychopathology risk during pregnancy has been investigated, with conflicting results. Previous studies showed a correlation between depressive symptoms during pregnancy and both lower and higher parity.4 Some studies report no differences regarding this, such as the study by Bassi (2017), which found that depression levels did not differ between primiparous and multiparous women.18 A study by Sockol (2015) suggested that multiparous women had higher levels of certain depression and anxiety risk factors, particularly interpersonal risk factors, which could be addressed in therapeutic interventions.19 Moreover, the same author proposed that primiparous women would benefit from cognitively-focused interventions, while mothers with older children would benefit from family-based or interpersonal interventions. In the present study, this second stance is particularly valuable among 81.2% multiparous women, suggesting that family-based and interpersonal interventions should be considered when designing a therapeutic plan for these patients.
Distribution according to previous referral or during pregnancy
G2 had a predominance of referrals from the Obstetric Department (56.3%) compared with PHC (18.8%). Considering that the greater pregnancy volume is followed at PHC, it is relevant to understand if this represents an under-referral and how that could be optimized. To facilitate pregnant women access to and follow-up in specialized care, studies have recommended measures − including adapted follow-up models (e.g., schedules adjusted to prenatal consultations) −, protocols for detection and guidance of women at risk − namely in PHC and Obstetrics, possibly involving screening surveys −, and better articulation between PHC, Obstetrics, and Psychiatry services. Women with severe prior psychiatric illness, namely in peripartum, and with other important risk factors, should be referred to Psychiatry.5,7
Predominance of depressive and anxious symptomatology was observed in both groups, in line with the most frequent psychopathological symptoms reported during pregnancy.1,2,4 A similar pattern was observed for ICD-10 diagnoses in women referred to consultation during pregnancy. However, a high prevalence of women with bipolar affective disorder diagnosis was observed in G1, in agreement with the fact that these women had longitudinal follow-up in Psychiatry. In women with previously recognized psychiatric disease, resurgence of symptoms or new episodes during pregnancy and puerperium should be focused.
Therapeutic approach
In a study by Ferracini et al (2017) evaluating 305 medical prescriptions for 58 women (31 pregnant, 27 breastfeeding) and respective risk category (according to FDA classification), 15 (13.8%) received category D and 2 (1.8%) category X drugs.20 Using the same classification, prescription of 21 category D drugs - corresponding to 23.9% of all prescriptions − during pregnancy was detected in this study. Besides noteworthy by itself, this percentage is superior to Ferracini study. Within chosen antidepressants, and as expected from other samples and guidelines, selective serotonin reuptake inhibitors (mainly sertraline) have been more frequently used.6,21,22
A meta-analysis by Van Ravensteyn (2017) found a robust moderate effect of cognitive-behavioral therapy for major depression during pregnancy and positive results for body-oriented interventions.23 This prompts reflection on the role of non-pharmacological approaches as legitimate treatment options for these patients.
The main limitations of this study are its cross-sectional nature, which prevents causality inference, relatively small sample size, and possible selection bias (e.g., exclusion of women followed in private practice in both specialties).
Conclusion
This study describes risk factors and characteristics of pregnant women followed in Psychiatry. Retrieved results identified some critical points that should be object of intervention. It is vital to perceive these women’s social support network, especially in the immigrant subpopulation. Incisive action should be taken regarding substance use cessation during and after pregnancy. Referral and longitudinal follow-up of women with high-risk pregnancies and/or psychopathology should also be addressed. Referral from PHC accounted only for a small percentage of cases in this sample, what should be investigated and involvement of these professionals promoted. Finally, clinicians should carefully explore existing pharmacological and non-pharmacological treatment options (e.g., cognitive-behavioral therapy, body oriented interventions) and avoid prescription of category D or X drugs, namely benzodiazepines.
In summary, this study enabled to identify existing risk factors and specific features associated with this population referral. Retrieved results prompt reflection on mental disease during pregnancy and its management in PHC, Obstetrics, and Psychiatry services and indicate aspects requiring special attention from health professionals and with the potential to be integrated in clinical practice
REFERENCES
1. Vesga-Lopez O, Blanco C, Keyes K, Olfson M, Grant BF, Hasin DS. Psychiatric Disorders in Pregnant and Postpartum Women in the United States. Arch Gen Psychiatry. 2008; 65:805-15. [ Links ]
2. Esteves M. Doença mental na Gravidez. (Tese para obtenção de grau de Mestre em Medicina). Inst Ciências Biomédicas Abel Salazar - Univ do Porto. 2012. [ Links ]
3. Kingston D, Tough S, Whitfield H. Prenatal and Postpartum Maternal Psychological Distress and Infant Development : A Systematic Review. Psychiatry Hum Dev. 2012; 43:683-714. [ Links ]
4. Macedo AF, Pereira AT. Saúde mental perinatal. LIDEL, editor. Lisboa; 2014. [ Links ]
5. Ulrich F, Petermnan F. Consequences and Possible Predictors of Health-damaging Behaviors and Mental Health Problems in Pregnancy - A Review. Geburtshilfe Frauenheilkd. 2016; 76:1136-56. [ Links ]
6. NICE (National Collaborating Centre for Mental Health), Antenatal and Postnatal Mental Health: The NICE Guideline on Clinical Management and Service Guidance, The British Psychological Society & The Royal College of Psychiatrists. 2007. [ Links ]
7. Weinreb L, Byatt N, Moore Simas TA, Tenner K, Savageau JA. What Happens to Mental Health Treatment During Pregnancy? Women’s Experience with Prescribing Providers. Psychiatr Q. 2014; 85:349-55. [ Links ]
8. Byatt N, Simas T, Lundquist R, Johnson J, Ziedonis D. Strategies for improving perinatal depression treatment in North American outpatient obstetric settings. J Psychosom Obstet Gynecol. 2012; 33:143-61. [ Links ]
9. Kingston D, Austin MP, Heaman M, McDonald S, Lasiuk G, Sword W, et al. Barriers and facilitators of mental health screening in pregnancy. J Affect Disord. 2015; 186:350-7. [ Links ]
10. Kopelman R, Moel J, Mertens C, Stuart S, Arndt S, O’Hara M. Barriers to Care for Antenatal Depression. Psychiatr Serv. 2008; 59:429-32. [ Links ]
11. Maia T. Determinants of mother-baby relationship evaluated during pregnancy. (Tese para obtenção de grau de Doutor) Escola de Saúde Pública - Universidade Nova de Lisboa. 2014. [ Links ]
12. Instituto Nacional de Estatística 2015. Anuário Estatístico da Área Metropolitana de Lisboa, Edição de 2016. [ Links ]
13. Latif Z. The maternal mental health of migrant women. A Race Equality Foundation Briefing Paper. 2014. [ Links ]
14. Almeida, LM, Costa-Santos, C, Caldas, JP, Dias, S, Ayres-de-Campos, D. The impact of migration on women’s mental health in the postpartum period. Revista de Saúde Pública. 2016; 50(0). [ Links ]
15. Cook JL, Green CR, de la Ronde S, Dell CA, Graves L, Ordean A, et al. Epidemiology and Effects of Substance Use in Pregnancy. J Obs Gynaecol Can. 2017; 39:906-15. [ Links ]
16. Murphy-Eberenz K, Zandi P, March D, Crowe R, Scheftner W, Alexander M, et al. Is perinatal depression familial? J Affect Disord. 2006; 90:49-55. [ Links ]
17. Biaggi A, Conroy S, Pawlby S, Pariante C. Identifying the women at risk of antenatal anxiety and depression: A systematic review. J Affect Disord. 2016; 191:62-77. [ Links ]
18. Bassi M, Delle Fave A, Cetin I, Melchiorri E, Pozzo M, Vescovelli F, et al. Psychological well-being and depression from pregnancy to postpartum among primiparous and multiparous women. J Reprod Infant Psychol. 2017;35:183-95. [ Links ]
19. Sockol L, Battle C. Maternal attitudes, depression, and anxiety in pregnant and postpartum multiparous women. Arch Women’s Ment Heal. 2015;18:585-93. [ Links ]
20. Ferracini AC, Rodrigues AT, Visacri MB, Stahlschmidt R, Silva NMOD, Surita FG, et al. Potential Drug Interactions and Drug Risk during Pregnancy and Breastfeeding: An Observational Study in a Women’s Health Intensive Care Unit. Rev Bras Ginecol Obs. 2017;39:258-64. [ Links ]
21. Alwan S, Reefhuis J, Rasmussen S, Friedman J. Patterns of antidepressant medication use among pregnant women in a United States population. J Clin Pharmacol. 2011;51:264-70. [ Links ]
22. Chaudron L. Complex Challenges in Treating Depression During Pregnancy. Am J Psychiatry. 2013;170:12-20. [ Links ]
23. van Ravesteyn L, Lambregtse-van den Berg M, Hoogendijk W, Kamperman A. Interventions to treat mental disorders during pregnancy: A systematic review and multiple treatment meta-analysi. PLoS One. 2017;12:e0173397.
Endereço para correspondência | Dirección para correspondencia | Correspondence
Tiago Ferreira
Department of Mental Health
Hospital Prof. Doutor Fernando Fonseca
IC19, 2720-276 Amadora
Email: tiagofilipeferreira17@hotmail.com
Received for publication: 05.03.2019. Accepted in revised form: 16.03.2020

