











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Cytomegalovirus (CMV) has been identified as an important viral pathogen in humans for more than a century. CMV histopathology was first described in 1904, but it was not until 1957 that the virus was isolated by Craig et al.1 CMV is a member of the human herpesvirus family and infects multiple human cell types, including fibroblasts, epithelial cells, endothelial cells, macrophages, and myocytes. Over the last several decades, the prevalence and relevance of CMV as a human pathogen became more apparent. Congenital CMV (cCMV) infection occurs frequently. Birth prevalence is around 1% and 11% of infants are symptomatic at birth.1,2 CMV infection is the most common cause of nonhereditary sensorineural hearing loss. In addition to congenital and perinatal infection, CMV is associated with significant morbidity in immunocompromised patients, including chorioretinitis, pneumonia, colitis, and neuropathy.1 During pregnancy, CMV transmission can occur due to maternal primary infection in previously seronegative women or after a non-primary infection (reactivation or reinfection by a new viral strain) in women with preconceptional immunity.3 In proven cases of CMV non-primary infection (NPI) very different serologic and molecular patterns may be observed and routine serologic testing may fail to assist in diagnosis.4,5 This case report illustrates pitfalls of serologic analysis in CMV NPI and discusses the respective underlying rationale.
Case report
A 37-year-old mother delivered a male infant after 34 weeks by cesarean section. Maternal CMV serology prior to conception showed positive immunoglobulin (Ig) G (15.3 AU/mL; reference value <1.1) and negative IgM (0.438 index; reference value <1.1), indicating CMV infection in the past. Other serology tests, including hepatitis B virus surface antigen, human immunodeficiency virus, venereal disease research laboratory, rubella virus, and toxoplasmosis in all trimesters showed no evidence of acute infection. Routine ultrasound (US) screening revealed fetal echogenic bowel at 20 weeks of gestation (WG) and fetal growth restriction with absent diastolic flow in the umbilical artery at 33+5 WG. At that time, the mother was admitted for observation and administration of antenatal corticosteroids for fetal lung maturation. The boy was born four days later, with Apgar scores of 6 and 9 at 1 and 5 min, respectively, with a birth weight of 1780 g in the 10th percentile (P10), 42 cm of length (P10), and 31 cm of head circumference (P50). He was admitted to the Neonatal Intensive Care Unit with respiratory distress and initially treated with nasal continuous positive airway pressure (nCPAP) during the first six hours of life, receiving a mean airway pressure of 6 cm H2O and with an oxygen requirement of 21%. On day one of life, diffuse jaundice, petechiae on trunk and limbs, and hepatosplenomegaly were observed on physical examination. Laboratory studies showed decreased platelet count (105,000/μL) and hyperbilirubinemia (total bilirubin level at 9.7 mg/L). Based on physical and laboratory findings, cCMV infection was suspected. At this time, due to risk of CMV transmission through breast milk, the mother was advised to stop breastfeeding. A preterm infant formula was started and maintained until peripartum maternal serology results were known. Abdominal US performed on the second day of life confirmed hepatosplenomegaly and cranial US revealed enlargement of lateral ventricles (right ventricle = 13.3 mm; left ventricle = 11.3 mm). Urine CMV PCR testing was positive, confirming cCMV infection, with a peripheral blood viral load higher than 5,000 copies/mL. Maternal serology at the time of diagnosis was the same as prior to conception, with negative IgM and no elevation of IgG titers. Ophthalmological evaluation of the newborn performed on the ninth day of life was normal, but neonatal hearing screening revealed lack of bilateral response. Due to auditory and neuroimaging (cranial US) findings, the child started antiviral treatment with oral valganciclovir (16 mg/kg per dose every 12 hours), with neutropenia (absolute neutrophil count of 600/uL) as the only side effect detected on the seventh day of treatment. Evolution was marked by good clinical and biological improvement, with jaundice and petechiae regression and platelet count increase to normal levels on the 16th day of life. Brain magnetic resonance imaging (MRI) performed on the 20th day of life showed diffuse hypersignal along the cerebral hemispheres on T2-weighted images, especially in the temporo-parietal regions. Lateral ventricles were large, with no signs of intraventricular tension. No calcifications or other abnormalities were identified. Antiviraltherapywas administered forsix months.
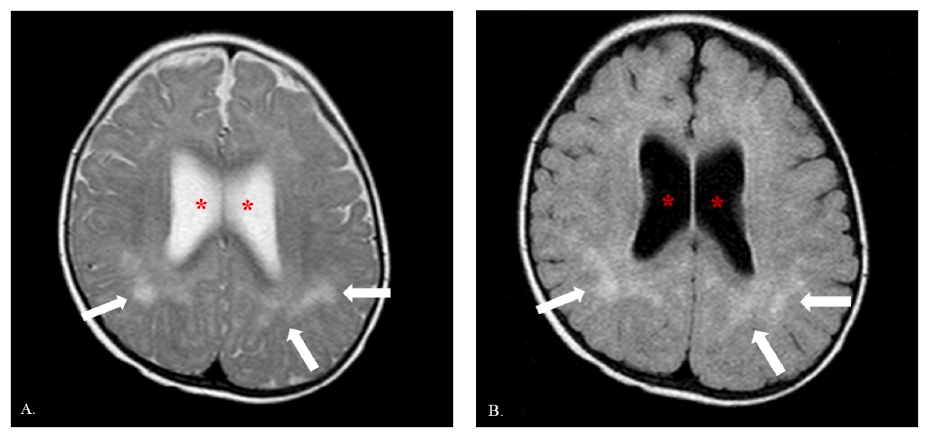
Regular follow-up visits have been conducted since discharge. On the second month of life, mild bilateral sensorineural hearing loss (15%) was detected. At four months of age, the patient was fully recovered from hearing loss Brain MRI was repeated at twelve months of age, showing multiple white matter hyperintense lesions on T2-weighted sequences and FLAIR sequences onboth cerebral hemispheres, mainly in the corona radiata and temporal regions, associated with ventriculomegaly. These findings were consistent with sequelae from cCMV infection (Figure 1). The boy is currently seventeen months old and presents normal hearing and ophthalmological and neurodevelopment evaluation.
Discussion
Exposure to CMV can occur from almost all body fluids.1 CMV can be maternally transmitted during pregnancy or perinatal period from exposure to genital secretions during delivery. In addition, the infection can occur postnatally after exposure to human milk, blood products, or community sources.1 Very premature babies are at higher risk of symptomatic CMV infection acquired from human milk, due to their immature immune system and paucity of maternal antibodies.6 Postnatal CMV infection in this population can present as sepsis-like illness, including respiratory symptoms (pneumonitis), hepatomegaly, thrombocytopenia, neutropenia, and lymphocytosis.
During pregnancy, CMV transmission can occur due to maternal primary infection in previously seronegative women. Alternatively, in women who are seropositive before pregnancy, cCMV infection may result from reactivation or acquisition of a new CMV strain.
It was previously believed that non-primary infections had a low transmission rate due to preconceptional immunity. However, it has been recently reported that cCMV infection can occur more often in infants of preconceptionally seropositive women.3,7
Sensorineural hearing loss, the main long-term complication of this congenital infection, occurs in 12.6% of all cases (18% of symptomatic and 9% of asymptomatic infants).8 It is estimated that one in every five cases of pediatric sensorineural hearing loss is due to cCMV infection. Prognosis improves with earlier infection detection and intervention, thereby making it potentially preventable or treatable.9
Despite detailed knowledge about the epidemiology and pathogenesis of this disease, CMV screening during pregnancy remains controversial. Testing costs, the high proportion of asymptomatic infants, potentially adverse psychosocial effects, and absence of effective preventive measures against fetal transmission are acknowledged barriers to screening implementation. Because of this, asymptomatic cases not identified at birth may be diagnosed too late to initiate antiviral therapy, which is associated with beneficial effects on hearing and neurodevelopment if initiated within the first month of life.9
In Portugal, the Directorate-General of Health (DGS) recommends preconceptional screening of CMV-specific antibodies which, in cases of clinical or ultrasonographic primoinfection suspicion, enables comparing laboratory values and facilitates diagnostic procedures.10
The gold standard in the serological diagnosis of primary CMV infection is maternal seroconversion based on detection of IgG antibodies against CMV or presence of serum anti-CMV specific IgM antibodies combined with low-avidity anti-CMV IgG antibodies.
IgG antibodies show low antigen avidity during the early weeks after primary infection. They progressively mature, initially acquiring moderate and then high avidity. This process reflects immune response maturation, with high-avidity IgGs maintained for many years.11 Therefore, low CMV IgG avidity is an accurate indicator of primary infection within the preceding three to four months, whereas high avidity can be considered a good indicator of non-primary infection or past infection.
Early cCMV diagnosis following non-primary maternal infection is difficult in both the prenatal and postnatal periods due to ambiguous interpretation of maternal serology and fetal US and to non-specific neonatal presentation.4,12 In most series, diagnosis of recurrent infection is based on an increase of CMV IgG titer (along with high CMV IgG avidity index) and/or positive CMV IgM. However, positive CMV IgM and significant CMV IgG raise can be observed in other, much more frequent clinical situations than CMV NPI: nonspecific immune system stimulation, maternal auto-immune disorders, and other cross-reacting herpetic infections.13,14 Additionally, according to the literature, in proven cases of maternal CMV NPI, very different serologic and molecular patterns may occur: positive or negative CMV IgM, significant CMV IgG raise or stability, positive or negative blood viral load, or fluctuant CMV IgG avidity.4 This explains why routine serologic testing may fail to help diagnosis, and disease identification can be challenging based on this approach. The number of seropositive women with NPI during pregnancy is in fact unknown.15-17 Another unresolved issue is whether transplacental transmission is most often consecutive to reactivation or reinfection.
In the present case report, no CMV IgG titer increase was observed and IgM titers remained negative in the peripartum period. The authors believe that this fact was probably due to virus reactivation during pregnancy. Indeed, the immune system may have not been stimulated in this patient because the CMV strain responsible for NPI was the endogenous one.4
The fetal compartment can be studied through non-invasive (US) and invasive (amniocentesis) methods. The latter should be carried out more than 6 weeks after the presumed maternal infection and after 20−21 weeks of gestation.5,18 Multiple US changes can be found in infected cases, including periventricular calcification, cerebral ventriculomegaly, echogenic bowel, or fetal growth restriction (FGR). However, US sensitivity is poor, allowing to correctly identify no more than 20% of infected infants.19 Fetal echogenic bowel is a nonspecific marker commonly observed in normal fetuses that may confuse or mask cCMV infection diagnosis, as in this case. In contrast, amniocentesis followed by real-time PCR provides an optimal means for diagnosing fetal infection, with good specificity and sensitivity (92−98% and ≈90%, respectively).20 However, the pros and cons of this invasive procedure should be discussed on a case by case basis.
After birth, cCMV is diagnosed through identification of the viral genome in urine, blood, saliva, or cerebrospinal fluid in the first three weeks of life.9
In the present case, the combination of prenatal (echogenic bowel and FGR), clinical (petechiae, jaundice, and hepatosplenomegaly) and laboratory (thrombocytopenia and hyperbilirubinemia) findings raised suspicion of cCMV diagnosis. The decision to initiate antiviral treatment was based on neuroimaging findings (even though they were not pathognomonic) together with auditory findings.
No antiviral drugs are currently licensed for cCMV treatment.21 Expert recommendations are based on two randomized controlled trials (RCTs) of six weeks of ganciclovir and in one RCT of six months of valganciclovir.22,23 Due to lack of evidence from a significant number of RCTs, the literature is unclear on whether mild and asymptomatic cases and those with isolated hearing loss should receive antiviral therapy.9
Much of the debate around treating less severely affected babies relates to the potential side effects of current antiviral drugs. Significant neutropenia is frequently observed in infants undergoing antiviral treatment. This is less commonly reported with valganciclovir than with ganciclovir (21% vs 65%) and generally occurs during the first month of treatment, as in the present case.21
The pathological neuroimaging findings in this patient at 12 months of age raised the possibility of worse prognosis in absence of treatment. Despite these changes, the child displayed normal neurodevelopment. Additionally, this case also highlights the unpredictability and great individual variability of CMV infection.
It should be reinforced that all women who are or intend to become pregnant, especially those who contact with young children, are at increased risk of CMV exposure and should be educated that the risk of infection can be significantly reduced by safe-handling techniques, such as use of latex gloves and rigorous hand washing after handling diapers or following exposure to respiratory secretions.24
Conclusion
In conclusion, this case highlights the pitfalls of CMV serology interpretation in non-primary infection during pregnancy. Since preexisting maternal CMV immunity provides incomplete protection, cCMV should be considered in fetuses or newborns with suggestive signs of infection, even in preconceptionally seropositive mothers, as early diagnosis has the potential to reduce the risk of negative outcomes.

