











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
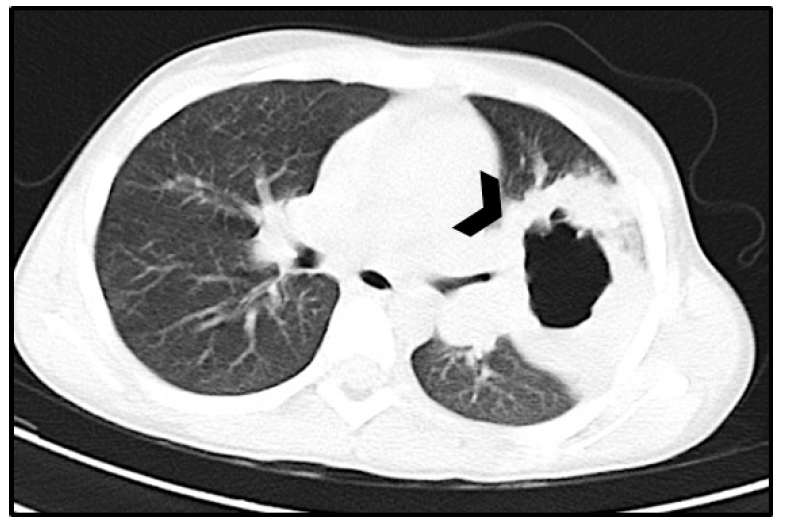
An eight-year-old Caucasian girl was admitted to the Emergency Department with a five-day history of generalized skin lesions associated with high fever and cough for the past two days. No sick contacts were reported. The girl had an unremarkable prior medical history and up-to-date vaccination, which did not include varicella vaccination. On examination, she appeared ill and febrile, with a generalized maculovesicular rash compatible with resolving varicella, without signs of cutaneous superinfection. She also presented with moderate respiratory distress (tachypnea and chest retractions). On chest auscultation, diminished breath sounds were noted on the left hemithorax. The girl was hemodynamically stable, with pulse oximetry of 95% on room air. Chest radiograph revealed a rounded and air-dense image with thickened walls, suggestive of central tissue loss (Figure 1). Blood work showed elevated inflammatory markers - total leucocytes of 18,000x103/ul (neutrophils 83%, with mild lymphopenia 1,320x103/ul) and C-reactive protein of 24.4 mg/dL. Chest computed tomography (CT) was performed, confirming the presence of a left superior lobe lesion with 60 x 50 x 50 mm presenting with a thick enhancing wall containing air (Figure 2).
What is your diagnosis?

Figure 1 Chest X-ray on admission showing a round and air-dense image with thickened walls suggestive of central tissue loss on the left hemithorax (black arrow).
Discussion
The girl was diagnosed with necrotizing pneumonia complicating a primary varicella infection and was admitted for parenteral antibiotic treatment and supportive therapy. She was treated with intravenous ceftriaxone and clindamycin, with progressive clinical improvement. The girl remained febrile for approximately eight days after admission. Blood culture was sterile. She was discharged home after a two-week course of parental antibiotics followed by an oral course of amoxicillin/clavulanate for a total of four weeks. At the six-month follow-up visit, total radiographic resolution and no immunodeficiency was found in additional studies.
Primary infection with varicella-zoster virus (VZV) is common during infancy. The condition has a generally benign clinical course characterized by fever and a typical generalized pruritic maculovesicular rash. Nevertheless, there is an acknowledged (although rare) association with severe complications related to bacterial superinfection (cellulitis, fasciitis, toxic shock syndrome, pneumonia) or VZV infection itself (cerebellitis, encephalitis, pneumonia). The most frequently described complication is bacterial superinfection of skin lesions. Bacterial pneumonia is a rare complication in immunocompetent children.1
Prolonged fever duration and a high number of skin lesions can increase the probability of complications.2 High and persistent fever (unusual in the resolving state of varicella) usually four to five days into the skin eruption can be a warning sign of possible concomitant bacterial infection, namely pulmonary complications (abscess, pneumonia, or other), especially in infants and small children.2 Even in the absence of respiratory distress or other classic symptoms, it is reasonable to order a chest x-ray to exclude pulmonary complications and admit the patient for medical surveillance.
Pulmonary complications of primary varicella infection can have two main presentations: hypoxemic interstitial varicella pneumonia, more frequent in adults and immunocompromised children or small infants, being one of the main causes of death in this setting in the latter;3,4 and secondary pulmonary bacterial infection (bacterial pneumonia, necrotizing pneumonia, amongst others), mainly due to Pneumococcus, Group A Streptococcus, and Staphylococcus aureus and mostly occurring in immunocompetent children.2-5
The pathogenesis of pulmonary bacterial complications in immunocompetent children is thought to derive from skin barrier disruption and virus-induced immunosuppression.2 In fact, VZV seems to induce a transient immunosuppression by altering the bactericidal function of neutrophils and weakening the mucosa of the respiratory system, potentially promoting the development of bacterial infections.2
A conservative management approach is usually recommended for pulmonary abscess and necrotizing pneumonia, consisting of a two-to-three-week course of parenteral antibiotics for uncomplicated cases, followed by a course of oral antibiotics until completing a total of four to six weeks.6 The antibiotic choice should be guided by Gram stain and culture results, when available, with initial empiric regimens including agents with aerobic and anaerobic coverage. Treatment regimens should include a penicillinase-resistant agent active against S. aureus and also comprise anaerobic coverage, typically with clindamycin or clavulanic acid. If Gram-negative bacteria are suspected or isolated, an aminoglycoside should be added. In cases of pulmonary abscess, early CT-guided percutaneous aspiration or drainage is recommended, as it can accelerate recovery and reduce the course of parenteral antibiotic therapy. For severely ill patients or those who fail to improve after seven to ten days of appropriate antimicrobial therapy, surgical intervention should be considered.6
Overall, the prognosis is good and most children become asymptomatic within seven to ten days of treatment, although fever can persist longer (sometimes for as long as two to three weeks).6 Radiologic abnormalities commonly resolve in one to three months, as in the present case, but can persist for years.6
The World Health Organization currently recommends VZV vaccination in routine childhood immunization programs in countries where varicella represents a significant public health burden.7 However, vaccine coverage should be attained and sustained above 85-90% to prevent a shift in VZV infection towards older ages, with increased morbidity and mortality, and an unpredictable impact on herpes zoster epidemiology.7
In summary, the authors reinforce the need for active surveillance of children diagnosed with varicella, informing parents on the usual clinical course of VZV and explaining the warning signs that require urgent referral to medical examination. In line with this and similarly to the present clinical case, any child presenting with rash suggestive of varicella or a recently confirmed diagnosis and with unusually prolonged fever and/or respiratory distress should be promptly examined, and pulmonary complications of the disease actively excluded.
This case reflects a serious, rare, and atypical complication of primary varicella infection in an immunocompetent child. The clinical scenario and radiologic findings serve an educational purpose.
Authorship
Miguel Bernardo - Conceptualization; Data Curation; Formal Analysis; Writing Original Draft; Writing Review & Editing
Ana Isabel Igreja - Conceptualization; Formal Analysis; Writing Original Draft; Writing Review & Editing
Joana Carvalho - Conceptualization; Formal Analysis; Supervision; Writing Original Draft; Writing Review & Editing
Helena Pereira - Conceptualization; Formal Analysis; Supervision; Writing Original Draft; Writing Review & Editing

