











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
A previously healthy nineteen-month-old boy presented to the Emergency Department with vomiting, abdominal pain, and prostration with three days of evolution and fever for a day. There was no history of drooling, refusal to feed, or changes in bowel movements. The parents initially associated these symptoms with the introduction of cow’s milk into the diet. No further information was provided. On physical examination, the child appeared ill, but there were no other specific findings. Additional investigations were requested. Laboratory tests showed elevated inflammatory parameters, and abdominal ultrasound showed no changes. A chest x-ray showed a round, double-ring, radiopaque foreign body, without ectopic air, around T4-T5, approximately 20 millimeters, suspected to be a battery (Figure 1), and the child was immediately referred for endoscopic removal.
What is your diagnosis?
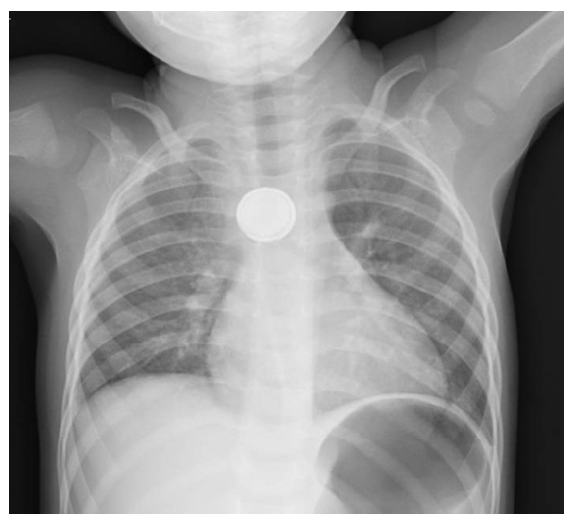
Figure 1 Chest radiograph showing a round, double-ring, radiopaque image around T4-T5 suspected of being a coin or a battery. The double ring/halo determined that it was a battery.
Discussion
Foreign body ingestion is a common problem between the ages of six months and three years.3 Most caregivers report a history of foreign body ingestion, which did not occur in this case.1,3
When ingestion is not witnessed or reported, suspicion should be raised in children with intellectual disability, since clinical symptoms are not specific.1 Stridor, drooling, fussiness, chest pain, abdominal pain, fever, feeding refusal, wheezing, and respiratory distress are all possible manifestations of foreign body ingestion.1,4
Management of foreign body ingestion depends on the type of foreign body (button batteries, magnets, sharp/pointed objects, food impaction, coins/blunt objects, superabsorbent objects), its location within the gastrointestinal tract, timing of the ingestion, clinical presentation, and patient size.4 The approach may be expectant in some cases or require emergent removal in others.1,4
Imaging with conventional radiograph of the neck, chest, and abdomen should be considered in all patients with suspected foreign body ingestion, even if the suspected object is not radiopaque, due to the possibility of other swallowed objects or ectopic air indicating perforation.1 Distinguishing between similarly shaped objects, such as coins and button batteries, can be difficult but is essential for a correct approach. Therefore, the radiograph should be carefully examined to distinguish between a coin and a battery.1 A double ring/halo sign on an anteroposterior radiograph suggests the presence of a battery.1,3,4
Coins are the most commonly ingested foreign bodies and are usually not an emergency.1)-(3 When a coin is located in the esophagus, removal is considered if there are severe clinical symptoms or if the coin does not move spontaneously after 24 hours of ingestion.1 A battery in the esophagus can rapidly cause serious health hazards due to its capacity for caustic injury, requiring early diagnosis and emergent removal to prevent complications.3,4
Possible complications of a battery lodged in the esophagus include mucosal burns, perforation, stricture, vocal cord paralysis, tracheoesophageal fistula, mediastinitis, bleeding (from an aortoenteric fistula), and death.1,3,4 Damage can be induced in only one hour and involve all layers of the esophagus in only four hours.3 Emergent endoscopic removal of the battery is the main approach.3,4
Conclusion
In the present case, the ingestion was not witnessed, and the symptoms evolved over 72 hours. This highlights the importance of the differential diagnosis of foreign body ingestion in the considered age group due to the potential consequences of ingestion of this type of material.
Authorship
Ana Catarina Fernandes - Writing - original draft; Writing - review & editing
Mariana Gaspar - Data curation; Investigation; Resources
Maria Bandeira Duarte - Data curation; Investigation; Resources
Alexandra Gavino - Writing - original draft; Writing - review & editing
Aldina Lopes - Project administration; Supervision; Validation

