











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
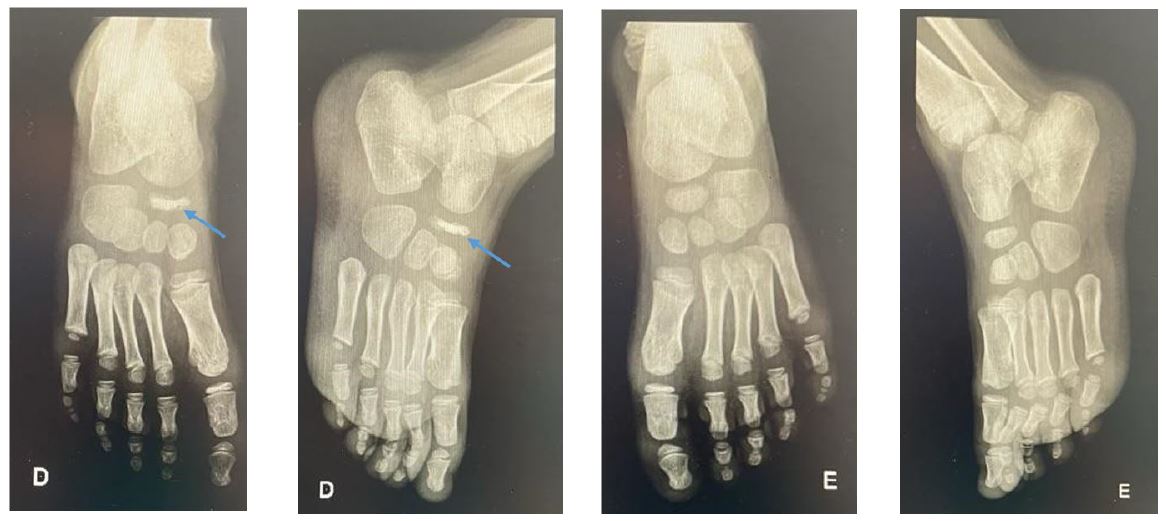
A previously healthy four-year-old boy was referred to the Orthopedic Department for right foot pain and intermittent limp with several weeks of evolution. His mother denied trauma, fever, or recent respiratory or gastrointestinal infection. Because the most common cause of limping at this age is transient synovitis, the hips were examined, but the findings were normal with symmetrical range of motion. There were no abnormal findings in the spine or feet, no swelling or joint redness, and gait was normal. Pelvic radiograph showed no alterations. Feet radiographs showed navicular collapse of the right foot with irregular areas of bone sclerosis and normal findings on the left foot (Figure 1).
What is your diagnosis?
Development
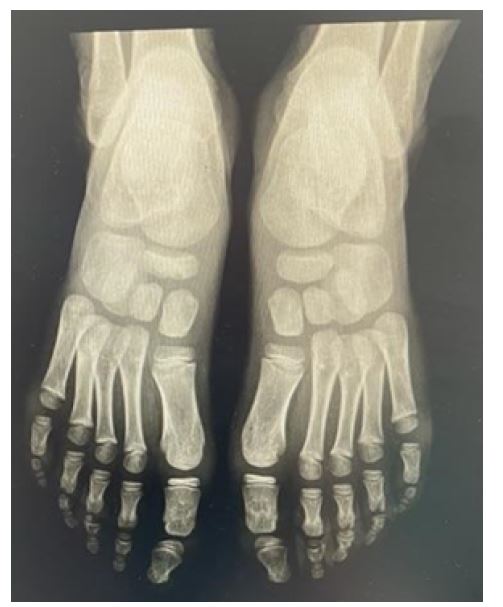
Pain control with analgesics, rest, and avoidance of physical activity were recommended. After four months, the patient was asymptomatic. At the end of two years of follow-up, he had no foot mobility or gait limitations. Radiographically, the navicular bone of the right foot had almost regained its normal anatomic structure, with more regular edges and less sclerosis compared with the left foot (Figure 2).
Discussion
Kohler’s disease is a rare osteochondrosis in children that causes pain and swelling of the midfoot.1-4 A clear cause remains unknown, but it is probably multifactorial.4,5 One of the most accepted hypotheses is that microtrauma of the ossification nucleus of the navicular bone by the remaining tarsal bones leads to disruption of the vascular supply, resulting in avascular necrosis.5 The navicular bone is subjected to constant forces between the astragalus and the cuneiform bones.3 Due to its later ossification (approximately five years if there are multiple ossification centers, being the last tarsal bone to ossify), damage to the navicular cartilage by surrounding structures can lead to ischemia.5
The main symptoms are mechanical midfoot pain, swelling, intermittent limping, and inability to bear weight.1 Affected children typically walk on the lateral portion of the foot.6 Limping may be the only clinical sign, making diagnosis difficult and often delayed.1 At earlier ages, pain location may be difficult to assess.1 Rarely, there may be redness on the dorsum of the foot.1 In this case report, the child had a normal physical examination, which may have delayed diagnosis. In most cases, there is no history of associated trauma.5 The condition is usually unilateral, but may be bilateral in 15-25% of cases.3,5 It affects more male children (male to female ratio 6:1) between the ages of two and seven years, and typically has a later mean age of presentation in boys compared to girls (5-6 years vs. 3.5-4.5 years), as the ossification process also occurs later in boys .1-3,5
The diagnosis is established by plain radiography of the foot, which should be performed under load.5 The most common radiographic finding is flattening of the navicular bone with irregular areas of sclerosis and loss of normal trabecular bone architecture.1,3 It may also present with small areas of fragmentation.3 Because the normal ossification pattern of the navicular bone can produce radiographic findings also seen in patients with Kohler’s disease, it is important to emphasize that the diagnosis depends on the presence of clinical symptoms.5 Given these normal variations in the ossification pattern of the navicular bone, it is also important to perform a radiograph of both feet to compare atypical findings, as was done in this case. The typical radiographic findings in this case combined with the described symptoms were compatible with Kohler’s disease. Computed tomography or magnetic resonance imaging are not indicated unless there is diagnostic doubt, as they do not add relevant information to the therapeutic decision.5 Some authors suggest that scintigraphy may be used at an early stage when the radiograph appears normal and shows less uptake due to decreased blood supply.2 However, scintigraphy is not often necessary2 and the decision to perform it must take into account the high dose of radiation to which the child will be exposed. The differential diagnosis should include inflammatory arthritis, infection and, less commonly, posterior tibial tendinitis, accessory navicular, or tarsal coalitions.5 If pain and limp complaints persist longer than expected, further evaluation should be initiated to exclude other diagnoses.3
Treatment recommendations include rest, limited weight bearing, and pain management with nonsteroidal anti-inflammatory drugs.1 If the pain is mild, the use of crutches may be recommended.5 If the pain is moderate to severe, immobilization for about four to eight weeks with a walking boot (which is more practical and better tolerated by children), a short-leg walking cast, or a plaster splint seems to reduce the duration of symptoms from ten to fifteen months to three to four months.3-6 Surgery is not indicated.5
Kohler’s disease is a self-limiting disease with an excellent prognosis and no sequelae1,6, as seen in this case. Regardless of treatment, the same final radiographic findings and clinical outcomes are expected.3 Follow-up visits should be continued until symptoms resolve.5 Serial radiographs show progressive restoration of the anatomic shape of the bone as vascularization normalizes.3,5 Radiographic resolution usually occurs in one to three years, but may occur as early as four months or as late as four years.1,7
KEY POINTS
Kohler’s disease is a benign, transient cause of limping and foot pain in children caused by avascular necrosis of the navicular bone.
Diagnosis requires a high index of suspicion based on clinical symptoms and typical radiographic signs.
The disease is self-limiting and has no sequelae regardless of treatment.
Further investigation is indicated only if symptoms persist.

