











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
A 14-year-old male with attention deficit hyperactivity disorder (ADHD), currently treated with lisdexamphetamine, and a two-year history of episodic constipation treated with polyethylene glycol was admitted to the pediatric ward with complaints of progressively less frequent and harder stools over the past two months, refractory to medical treatment (polyethylene glycol, milk of magnesia, and glycerin suppositories). He also reported abdominal pain, initially diffuse but localized to the hypogastric region over the past month, with progressive abdominal distension. He denied asthenia, pallor, or weight loss.
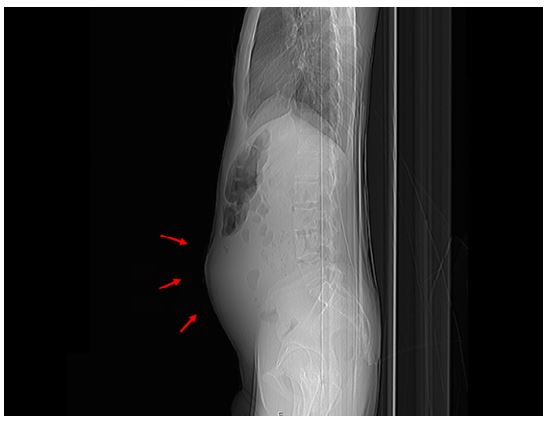
Physical examination revealed a thin appearance (body mass index = 16.9 kg/m2, z-score = -1.33), a distended and painful abdomen with tenderness, and a palpable mass with a rock-hard consistency in the hypogastric region. Abdominal radiograph (Figure 1) showed marked abdominal distension without air-fluid levels. Abdominal ultrasound revealed a large heterogeneous retroperitoneal mass in the midline of the abdomen and another lobulated hypoechoic mass near the rectum, suggestive of conglomerate lymph nodes or neoplasm.
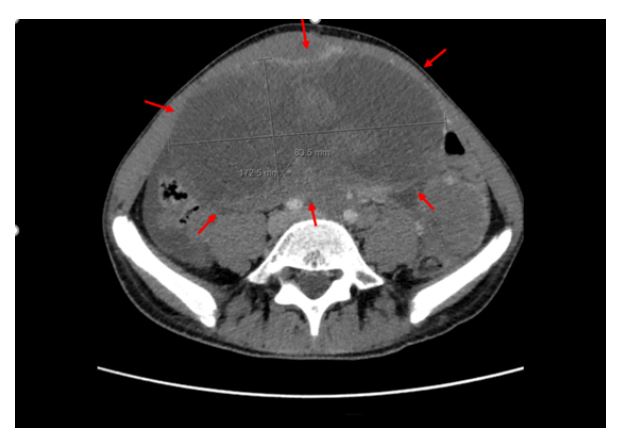
To further characterize these findings, an abdominopelvic computed tomography scan was performed (Figure 2), which revealed a midline mesenteric mass measuring 17.3 x 8.4 cm, along with multiple other ill-defined masses in the abdominal, retroperitoneal, and pelvic regions with areas of necrosis highly suggestive of an aggressive neoplastic process. In addition, there was evidence of peritoneal carcinomatosis and liver metastases. Complete blood count and biochemistry, including uric acid and lactate dehydrogenase levels, were within normal ranges.
What is your diagnosis?
Discussion
The diagnosis of desmoplastic small round cell tumor (DSRCT) was established by anatomopathologic examination of the mass in conjunction with immunohistochemistry and confirmed by cytogenetic analysis, which revealed the presence of the t(11;22) translocation responsible for the EWSR1-WT1 gene fusion.
DSRCT is an extremely rare and aggressive tumor of the serosal lining of the abdomen that predominantly affects Caucasian male adolescents. It is characterized by the recurrent t(11;22)(p13;q12) chromosomal translocation resulting in the fusion of the EWSR1 gene on chromosome 22q12 with the WT1 gene on chromosome 11p13.1
The patient in this case is currently being managed at a clinical cancer centre and has undergone chemotherapy, surgery, and radiotherapy with only a partial response. The prognosis remains poor due to the limited availability of effective treatment options.2
Constipation is a common problem in Pediatrics, with more than 95% of cases having a functional etiology. In adolescents, factors such as eating disorders, school stressors, and attention-deficit/hyperactivity disorder (ADHD) can promote or exacerbate constipation. Although rare, underlying causes must be considered in the presence of red flags.3
In this case, despite the patient’s history of functional constipation and ADHD, the sudden onset of bowel obstruction combined with localized abdominal pain, progressive abdominal distension refractory to medical treatment, and a palpable pelvic mass should be recognized as warning signs warranting further evaluation. Constitutional symptoms may not always be present as DSRCT is a rapidly progressive tumor.
Authorship
Sara Monteiro - Investigation; Methodology; Visualization; Writing - original draft
Beatriz Teixeira - Investigation; Methodology; Visualization; Writing - original draft
Cristiana Couto - Investigation; Methodology; Visualization; Validation; Writing - review & editing
Gisela Silva - Conceptualization; Methodology; Investigation; Supervision; Visualization; Validation; Writing - review & editing

