Imaging cases
Vulvar mass in a newborn: Should we worry?
Massa vulvar num recém-nascido: Deve ser uma preocupação?
1 Department of Pediatrics, Hospital de Vila Franca de Xira, Unidade Local de Saúde Estuário do Tejo. 2600-009 Vila Franca de Xira, Portugal. madalena.malato@hotmail.com; ines_ips93@hotmail.com; danielaframos88@gmail.com
Abstract
The authors describe the case of a newborn female with an ovoid interlabial genital mass, anterior to the vaginal introitus. The diagnosis of paraurethral cyst or Skene’s duct cyst was established. This diagnosis is clinical and it is important to be aware of the differential diagnoses. Management is conservative in most cases, with spontaneous resolution within weeks. The condition has a favorable prognosis.
Keywords: cyst; Neonatology; newborn; paraurethral
Resumo
É descrito o caso de um recém-nascido do sexo feminino com uma massa genital interlabial ovóide anterior ao intróito vaginal. Foi estabelecido o diagnóstico de quisto parauretral ou quisto do ducto de Skene. Este diagnóstico é clínico, sendo importante conhecer os diagnósticos diferenciais. A abordagem passa por uma atitude expectante na maior parte dos casos, com resolução espontânea em semanas. O quisto parauretral tem bom prognóstico, sem risco de sequelas ou recorrência.
Palavras-chave: quisto; Neonatologia; parauretral; recém-nascido
A term female newborn was delivered by emergency cesarean section due to respiratory distress requiring invasive ventilatory support. Her birth weight was 3035g.
Although the pregnancy was poorly monitored, third trimester obstetric ultrasound and maternal serologies were normal.
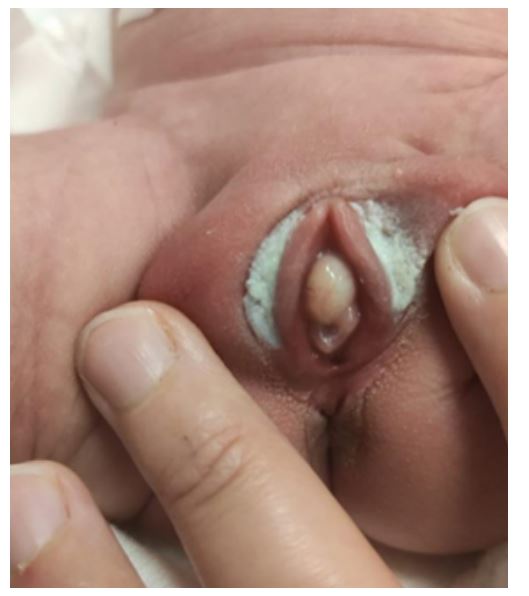
The girl presented with an ovoid, tender, yellowish, 12 mm x 17 mm interlabial mass, located anterior to the vaginal introitus (Figure 1). Although the mass partially covered the urethral meatus, normal voiding was observed. The remainder of the physical examination was unremarkable. Renal and bladder ultrasound showed no abnormalities.
The mass resolved spontaneously at two months of age.
Diagnosis
Paraurethral cyst or Skene’s duct cyst.
Discussion
Paraurethral cyst is a rare benign condition with either congenital or acquired etiology. It is rare in the newborn and the etiology remains unknown. Possible causes include exposure to maternal estrogen, dislocation of the urothelium and obstruction or stenosis of the Skene’s duct.1) It presents as a tender, yellowish, ovoid mass adjacent to the external urethral meatus and is usually asymptomatic. The diagnosis is clinical. Renal and bladder ultrasound allows to exclude associated complications or abnormalities.1
The location and displacement of the urethral meatus by the mass are characteristic of a paraurethral cyst. Differential diagnoses include imperforate hymen with hydrocolpos, rhabdomyosarcoma of the vagina, prolapsed urethra, ectopic ureterocele, and urethral diverticulum.2
The approach is usually expectant, with spontaneous resolution within weeks. Surgery, most commonly with needle aspiration, is reserved for paraurethral cysts with urinary obstruction.1),(3) Resolved paraurethral cysts have no long-term sequelae or the risk of recurrence.
Authorship
Madalena Torrado Malato - Conceptualization; Visualization; Writing - original draft; Writing - review & editing
Inês Pereira Soares - Writing - original draft; Writing - review & editing
Daniela Ramos - Conceptualization; Supervision
References
1. Costantino E, Ganesan GS. Paraurethral cysts in newborn girls. BMJ Case Reports. 2016 Oct 25. DOI: https://doi.org/10.1136/bcr-2016-216689;
[ Links ]
2. Nakamura E, Shintaku S, Horii M, Manabe H, Hirano Y, Koichi Murono. Early Regression of Paraurethral Cyst in a Neonate. Pediatrics & neonatology. 2014 Jun 1;55(3):225-7. DOI: https://doi.org/10.1016/j.pedneo.2012.12.005;
[ Links ]
3. Yilmaz Y, Celik IH, Dizdar EA, Demirel G, Yurttutan S, Erdeve O, et al. Paraurethral cyst in two female newborns: Which therapy option? Scandinavian Journal of Urology and Nephrology. 2011 Jul 20;46(1):78-80. DOI: https://doi.org/10.3109/00365599.2011.599337.
[ Links ]












 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink