










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkMedicina Interna
versão impressa ISSN 0872-671X
Medicina Interna vol.24 no.3 Lisboa set. 2017
https://doi.org/10.24950/rspmi/61/2017
CASOS CLÍNICOS / CASE REPORTS
Acidemia Metabólica Grave Após Enterocistoplastia de Aumento: Caso Clínico
Severe Metabolic Acidemia After Augmentation Enterocystoplasty: Clinical Case
Beatriz Frutuoso1, Helena Moreira2, Paulo Torres-Ramalho3, Luís Lopes3
1Serviço de Medicina Interna do Centro Hospitalar Vila Nova de Gaia/ Espinho, Vila Nova de Gaia, Portugal
2Serviço de Medicina Interna do Centro Hospitalar de São João, Porto, Portugal
3Serviço de Medicina Intensiva do Centro Hospitalar de São João,Porto, Portugal
RESUMO
A acidose metabólica hiperclorémica é uma complicação tardia frequente da ileocistoplastia de aumento e apenas raramente os doentes apresentam acidemia sintomática. Uma mulher de 64 anos com história de ileocistoplastia de aumento três meses antes foi admitida no serviço de urgência por fadiga, dor abdominal, náuseas e vómitos. Analiticamente, apresentava elevação dos parâmetros inflamatórios, disfunção renal, aumento ligeiro da amílase e lípase séricas e acidemia hiperclorémica grave. O diagnóstico inicialmente proposto foi pancreatite aguda. Contudo, atendendo ao diagnóstico diferencial de acidemia com gap aniónico normal, devido à perda de bicarbonato, a hipótese de acidemia pós ileocistoplastia era mais consistente. O tratamento com bicarbonato endovenoso e oral foi instituído, observando-se melhoria clínica e analítica. É essencial prever as alterações metabólicas pós procedimento e considerar todos os diagnósticos possíveis, de modo a diagnosticar e tratar precocemente, prevenindo a morbilidade associada.
Palavras-chave:Acidose; Bexiga Urinária/cirurgia
ABSTRACT
Hyperchloremic acidosis is a late frequent complication of augmentation ileocystoplasty, but only rarely patients develop symptomatic acidemia. A 64-year-old woman, with history of augmentation ileocystoplasty three months before, was admitted in the emergency department complaining of fatigue, abdominal pain, nausea and vomits. Analytical evaluation presented an elevation of the inflammatory parameters, renal dysfunction and a slight elevation of serum amylase and lipase, as well as severe hyperchloremic acidemia. The first diagnosis hypothesis was thought to be acute pancreatitis. However, attending to the differential diagnosis of metabolic acidemia with normal anion gap and due to bicarbonate loss, the hypothesis of acidemia after ileocystoplasty was more consistent. Treatment with endovenous and oral bicarbonate was instituted and clinical and analytical improvement were observed. It is essential to foresee the metabolic complications of this procedure and consider all possible diagnoses in order to diagnose and treat early, preventing associated morbidity.
Keywords:Acidosis; Urinary Bladder/surgery
Introduction
Vesical augmentation is a surgical technique used for the treatment of patients with small and hyperactive bladders of high pressure and low accommodation who do not respond to medical therapy. The main goals are to increase the bladder functional capacity with lower filling pressures. Usually, an intestinal segment is incorporated as a patch into the bladder.1,2 Metabolic acidosis is a late complication associated to this procedure when ileum or colon are used for the augmentation.1-4 Metabolic acidosis is common, but only rarely causes symptomatic acidemia, requiring endovenous alkalinizing therapy.5
The authors describe a case of severe metabolic acidemia following an augmentation ileocystoplasty.
Clinical Case
A 64-year-old woman was admitted in the emergency department complaining of fatigue, abdominal pain, nausea and vomits for the previous three days.
She had history of pharmacologically controlled arterial hypertension and type 2 diabetes mellitus causing retinopathy and nephropathy. Surgical history was relevant for cholecystectomy due to vesical calculi four years before; gastric bypass for obesity two years before with consequent dumping syndrome (weakness after meals, nausea, abdominal distention and cramps and two to three liquid dejections per day since the surgery). She was also submitted to an augmentation ileocystoplasty three months before the admission because of genito-urinary tuberculosis. Her usual prescription was amlodipine 5 mg/day, metformin 1000 mg/day, linagliptin 5 mg/day and pantoprazole 40 mg/ day.
At the emergency department, she was orientated in time and space, hemodynamically and electrically stable (blood pressure: 101/40 mm Hg; cardiac frequency: 87 bpm), apyretic (tympanic temperature of 36.1ºC), tachypneic (respiratory rate: 29 cpm), but with no other signs of respiratory stress. She presented dry mucous membranes and exhibited a dolorous abdomen to palpation, mostly in the superior quadrants. Laparotomy incision was well-healed with no signs of infection. No other alterations were observed at physical examination.
Arterial gasometry revealed pH: 7.08; pCO2: 14 mm Hg; pO2: 71.7 mm Hg; HCO3: 4.1 mEq/L; anion gap (AG): 7 mmol/L. Analytical evaluation presented: leucocytes: 12.720/uL (N: 4000-11.000), C-reactive protein (CRP):63.3 mg/L (N < 3), urea/creatinine: 110/3.49 mg/dL (N: 10- 50/0.51-0.95), K: 5.3 mmol/L (N: 3.5-5.1), Cl: 124 mEq/L (N: 101-109); amylase/lipase: 127/289 U/L (N:22-80/7-60). No other alterations were observed. Urinalysis had urinary pH: 6.5 and proteinuria 2.50 g/L (N < 0.15). Abdominal ultrasonography did not show any new relevant alterations. Electrocardiogram revealed sinus rhythm at 92 bpm.
The initial diagnosis hypothesis was thought to be acute pancreatitis and pre-renal exacerbation of the chronic renal disease causing metabolic acidemia.
She was admitted in a polyvalent intermediate care unit. She was started on crystalloid fluids, endovenous sodium bicarbonate 8.4% (NaHCO3) initially at 200 mL/hour and then at 125 mL/hour, endovenous analgesics and kept on nothing by mouth status.
Within four hours she was clinically better, with no abdominal pain and no vomits. Repeated gasometries showed slow progressive improvement of the metabolic acidemia.
Blood tests taken 12 hours later demonstrated a decrease in inflammatory parameters (leucocytes: 8.030/uL; CRP: 51 mg/L), improvement in renal function (urea/creatinine: 98/ 2.94 mg/dL) and normal ionogram and serum amylase and lipase. Given the rapid resolution of the abdominal symptoms and normalization of amylase and lipase and the absence of alterations in the ultrasonography the case was again reviewed. The hypothesis of hyperchloremic metabolic acidemia after recent augmentation ileocystoplasty was then considered.
She initiated oral diet 12 hours after the admission, with good tolerance, and was switched to oral NaHCO3 supplementation at 48 hours. By that time metabolic acidosis was corrected and all analytical alterations were reversed. The patient remained stable and was transferred to a general ward to titrate bicarbonate dose. She was discharged home five days later, asymptomatic, with the prescription of 1000 g/day of oral NaHCO3.
She was evaluated in urologic consult and had no further episodes of metabolic acidosis in the six months after the discharge.
Discussion
Vesical augmentation is a surgical option to treat neurogenic and non-neurogenic bladder dysfunction when pharmacological and minimal invasive treatments were unsuccessful. It has a role in the management of inflammatory bladder disorders, as post-radio and chemotherapy cystitis, schistosomiasis, tuberculosis - as the case presented – and interstitial cystitis, which lead to a low capacity and poorly compliant bladder.1
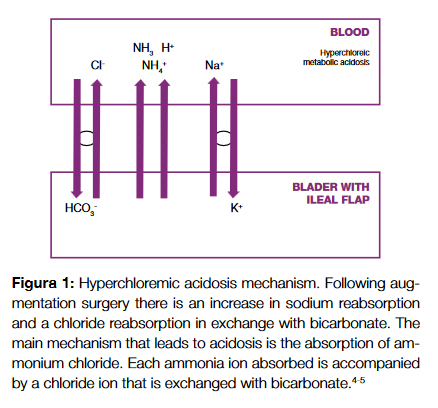
Metabolic disturbances are amongst the late complications of this procedure. The most frequent is hyperchloremic metabolic acidosis, especially when ileum or colon are used. The bowel segment retains its absorbing and secreting characteristics leading to reabsorption of ammonium, hydrogen ions and sodium and the secretion of bicarbonate, resulting in a chronic acid load (Fig. 1).1-5 Patients with baseline renal insufficiency are at greater risk for the development of persistent metabolic acidosis because compensatory mechanisms for these metabolic changes are impaired.6,8-10
The frequency and severity of this complication varies with bowel segment length, contact time, patient comorbidities and pre-existing renal insufficiency.8,10 Case reports describe frequencies as different as 8% to 48% for metabolic acidosis, but only 4% to 15% for symptomatic acidemia.4,6,7,11,12
Most patients are asymptomatic. In more severe cases symptoms are often unspecific: weakness, fatigue, anorexia, nausea, thirst.8,10
Diagnosis is based on clinical history and arterial blood gas analysis. Gasometry reveals a hyperchloremic metabolic acidosis, characterized by a decrease in arterial pH (<7.35) because of a low serum bicarbonate concentration (<22 mE- q/L), resulting in a normal anion gap.
Normal anion gap metabolic acidosis is a consequence of loss of bicarbonate or bicarbonate precursors as happens in 1)severe diarrhea or other gastrointestinal losses or 2) type 2 (proximal) renal tubular acidosis (RTA) or a decreased renal acid excretion in case of 3) renal insufficiency or 4) types 1 and 4 (distal) RTA.13
Given these differential diagnoses, the clinical history is key to determine the definitive diagnosis, but there are other complementary exams that may be valorised.14 A urine pH evaluation superior to 5.5 in a patient with acidemia is characteristic of type 1 RTA, but may be observed in cases of elevated ammonium excretion; urinary AG is a measure of urinary NH4+ and its elevation points to a renal acidification defect, as in distal RTA; the ejection fraction of HCO3- is useful in the diagnosis of proximal RTA and the urine-blood PaCO2 gradient after a HCO3- loading in patients with distal RTA helps differentiate a permeability defect from other defects; a low level of citrate in the urine is found in distal RTA. Furthermore, measuring the transtubular potassium gradient is useful in determining the etiology of hyperkalemia or hypokalemia associated with metabolic acidosis.
This patient was admitted with unspecific abdominal complaints and had elevated inflammatory parameters and serum lipase and amylase that led to the first erroneous hypothesis of acute pancreatitis. This diagnosis did not explain the hyperchloremic metabolic acidemia. Additionally, the normal ultrasonography and rapid normalization of the inflammatory parameters and serum amylase and lipase helped exclude it, prompting the investigation of another cause. The patient had severe non-compensated metabolic acidemia with normal anion gap and a cause that fitted the differential diagnosis: history of augmentation ileocystoplasty three months before. In fact, chronic renal disease may, in severe cases, cause per se metabolic acidosis. The same applies to diarrhea due to dumping syndrome. Still, both the renal impairment and the dumping syndrome, were previously present and the patient had never had acidosis. Moreover, there was a more immediate and probable cause to the acidemia. Despite the low probability of both pathologies being responsible for the acidemia, they could have contributed to increase the severity of the acidosis.
The urinary pH was elevated due to reabsorption of ammonium. In this case, no further complementary tests were taken, as the diagnosis was established based on the most evident cause.
Due to ileal absorption of potassium, patients submitted to ileocystoplasty have, most often, hypokalemia (Fig. 1).1,5,9 This patient, on the contrary, presented in the emergency department with a mild hyperkalemia that rapidly reversed without potassium lowering agents. We attributed this alteration to worsening of the renal function and consequent inability to excrete potassium. As the renal function improved there was a normalization of the ionogram.
Treatment of non-symptomatic metabolic acidosis is based on alkalinizing therapy with oral sodium bicarbonate or, as alternative, sodium citrate.5,8 Due to the severity of the acidemia in this case, it was necessary initial endovenous reposition that was replaced for an oral formulation once the pH and HCO3 target values were achieved.
This case intends to alert to the importance of preoperative counselling and timely follow-up. It is, perhaps, necessary to better educate the patient to recognize the signs of possible complications, and make clear written records in discharge notes and/or follow up consults signaling probable complications, especially in patients more prone to them. More so, this case also aims to reiterate the need of a complete clinical history and systematic differential diagnosis review to easier enlighten the more plausible diagnosis for each patient.
Conclusion
Hyperchloremic acidosis is a well described late complication of augmentation ileocystoplasty, but only rarely causes symptomatic acidemia. Gasometry is the most important complementary exam. Treatment is based on alkalinizing therapy with bicarbonate. In more severe cases hospitalization for endovenous therapy is required.
It is essential to foresee the metabolic complications of this procedure and consider all possible diagnosis to treat early and prevent associated morbidity.
References
1.Veeratterpillay R, Thorpe AC, Harding C. Augmentation cystoplasty: Contemporary indications, techniques and complications. Indian J Urol. 2013;29:322-7. [ Links ]
2.Sountoulides P, Laguna MP, de la Rosette JJ. Complications following augmentation cystoplasty; prevention and management. Central Eur J of Urol. 2009;62:216-21. [ Links ]
3.Gerharz EW, Turner WH, Kalble T, Woodhouse CR. Metabolic and functional consequences of urinary reconstruction with bowel. BJU Int. 2003;91:143-9. [ Links ]
4.Escudero RM, Patiño GE, Fernández ER, Gil MJ, García EL, Alonso AH, et al. Bladder augmentation using the gastrointestinal tract. Indication, follow up and complications. Arch Esp Urol. 2011;64:953-9. [ Links ]
5.Mills RD, Studer EU. Metabolic consequences of continent urinary diversion. J Urol. 1999;161:1057-66. [ Links ]
6.Khoury JM, Timmons SL, Corbel L, Webster GD. Complications of enterocystoplasty. Urology. 1992;40:9-14. [ Links ]
7.Hautmann RE, de Petriconi R, Gottfried HW, Kleinschmidt K, Mattes R, Paiss T. The ileal neobladder: complications and functional results in 363 patients after 11 years of followup. J Urol. 1999;161:422-8. [ Links ]
8.Vasdev N, Moon A, Thorpe AC. Metabolic complications of urinary intestinal diversion. Indian J Urol. 2013;29:310-5. [ Links ]
9.Pravin K Rao, Alan J Iverson, Edmund S Sabanegh. Augmentation Cystoplasty Technique. Medscape. [accessed in 14 Dec 2016]. Available from: http://emedicine.medscape.com/article/443916-technique#c4. [ Links ]
10.Eldred-Evans D, Khan F, Abbaraju J, Sriprasad S. An unrecognized case of metabolic acidosis following neobladder augmentation cystoplasty. Int J Surg Case Rep.2015;11:129-31. [ Links ]
11.Cheng KC, Kan CF, Chu PS, Man CW, Wong BT, Ho LY, et al. Augmentation cystoplasty: Urodynamic and metabolic outcomes at 10-year follow-up. Int J Urol. 2015;22:1149-54. [ Links ]
12.Benchekroun A, Lachkar A, Hadab A, Soumana A, Farih MH, Belahnech Z, et al. Augmentation enterocystolplasty. 35 cases. Ann Urol. 1998;32:290-4. [ Links ]
13.Emmett M, Szerlip H. Approach to the adult with metabolic acidosis. UpToDate. [accessed 01 Jan 2017]. Available from: https://www.uptodate.com/contents/approach-to-the=-adult-with-metabolic-acidosis?source-search_result&search=Approach+to+the+adult+with+metabolic+acido-sis&selectedTitle=1%7E150. [ Links ]
14.Yeung SCJ. Hyperchloremic Acidosis Workup. Medscape. [accessed 07 June 2017]. Available from: http://emedicine.medscape.com/article/240809-overview. [ Links ]
Correspondência:Beatriz Frutuoso beatriz.frutuoso@chvng.min-saude.pt
Serviço de Medicina Interna, Centro Hospitalar Vila Nova de Gaia/Espinho,
Rua Conceição Fernandes, 4434-502, Vila Nova de Gaia
Conflicts of interest: The authors have no conflicts of interest to declare.
Financing Support: This work has not received any contribution, grant or scholarship.
Confidentiality of Data: The authors declare that they have followed the protocols of their work center on the publication of data from patients.
Protection of Human and Animal Subjects: The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Protecção de Seres Humanos e Animais: Os autores declaram que não foram realizadas experiências em seres humanos ou animais
Direito à Privacidade e Consentimento Informado: Os autores declaram que nenhum dado que permita a identificação do doente aparece neste artigo.
Conflitos de Interesse: Os autores declaram a inexistência de conflitos de interesse na realização do presente trabalho
Fontes de Financiamento: Não existiram fontes externas de financiamento para a realização deste artigo
Recebido: 08/03/2017
Aceite: 14/05/2017

