










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkMedicina Interna
versão impressa ISSN 0872-671X
Medicina Interna vol.27 no.3 Lisboa jul. 2020
https://doi.org/10.24950/O/19/20/3/2020
ARTIGOS ORIGINAIS / ORIGINAL ARTICLES
Nutritional Status as a Risk Factor in a Cohort of Geriatric Patients in a Specialized Convalescence Unit
Estado Nutricional como Factor de Risco numa Coorte de Pacientes Geriátricos numa Unidade de Convalescença Especializada
Miguel Ardérius1  https://orcid.org/0000-0001-9325-0452
https://orcid.org/0000-0001-9325-0452
Marta Fournier2,3 https://orcid.org/0000-0002-3664-791X
Mariana Alves1 https://orcid.org/0000-0002-1369-8423
Helena Bárrios3 https://orcid.org/0000-0002-9012-3770
Maria João Duarte3 https://orcid.org/0000-0001-5333-5283
Manuel Caldas de Almeida3 https://orcid.org/0000-0002-4486-2898
1Serviço de Medicina III, Centro Hospitalar Lisboa Norte, Lisboa, Portugal
2USF Santo Condestável, Lisboa, Portugal
3Hospital Residencial do Mar, Bobadela, Portugal.
Abstract:
Introduction: Malnutrition is frequent in the elderly and is a healthcare problem. Our objective was to characterize the elderly population admitted to a convalescence unit and relate the nutritional status on admission with functional and health-related outcomes.
Methods: All patients over 65 years old admitted to a convalescence unit during an 18-month period were analysed in regard to nutritional, functional and socio-familial status, risk of falling and risk of developing pressure ulcers.
Results: Hundred eighty one patients, 57.5% females, aged 80.0±7.1 years old were included. Mini Nutritional Assessment classified 1/3 as undernourished and 66.3% as at risk for malnutrition. The great majority did not have a good socio-familial situation. Almost 2/3 had high risk of falling. Over 80% had no or mild risk for developing pressure ulcers. Over half were discharged home. Moderate correlations were found between nutritional status and both dependence for activities of daily living (ADL) and risk of developing pressure ulcers.
Discussion: We found a high incidence of malnutrition, dependence for ADL, socio-familial problems and high risk of falling. We found a statistically significant relation between nutritional status and risk of developing pressure ulcers, constituting an important alert that nutritional evaluation and support may have a crucial role in people’s quality of life.
Conclusion: Our findings are concerning and support the recommendations to routinely screen for malnutrition and provide nutritional support in all healthcare settings. To the best of our knowledge, this was the first survey of malnutrition and its implications carried out in a Portuguese convalescence unit.
Keywords: Accidental Falls; Aged; Convalescence; Geriatrics; Hospital Units; Malnutrition; Nutrition Assessment; Pressure Ulcers; Socioeconomic Factors.
Resumo:
Introdução: A malnutrição é frequente no idoso e é um problema de saúde pública. O objectivo foi caracterizar a população idosa internada numa unidade de convalescença e relacionar o estado nutricional à admissão com o aumento de complicações.
Métodos: Todos os pacientes com mais de 65 anos admitidos numa unidade de convalescença num período de 18 meses foram analisados no que respeitava a estado nutricional, funcional e sócio-familiar, risco de queda e risco de desenvolvimento de úlceras de pressão.
Resultados: Cento oitenta um pacientes, 57,5% mulheres, idade 80,0±7,1 anos. O Mini Nutritional Assessment classificou 1/3 como desnutridos e 66,3% em risco de desnutrição. A grande maioria não tinha uma boa situação sóciofamiliar. Cerca de 2/3 tinham alto risco de queda. Mais de 80% tinha risco baixo de desenvolver úlceras de pressão. Mais de metade teve alta para o domicílio. Correlações moderadas foram encontradas entre o estado nutricional e tanto o grau de dependência como o risco de desenvolver úlceras de pressão.
Discussão: Encontrámos uma alta incidência de malnutrição, dependência nas actividades de vida diária, problemas socio-familiares e alto risco de queda. Encontrámos uma relação estatisticamente significativa entre o estado nutricional e o risco de desenvolver úlceras de pressão, constituindo um importante alerta que a avaliação e suporte nutricionais podem ter um papel crucial na qualidade de vida.
Conclusão: O que encontrámos é preocupante e suporta as recomendações para rotineiramente rastrear a malnutrição e proporcionar suporte nutricional em todos os níveis de cuidados de saúde. Tanto quanto sabemos, esta foi a primeira avaliação de malnutrição e problemas associados levada a cabo numa Unidade de Convalescença da Rede Nacional de Cuidados Continuados Integrados em Portugal.
Palavras-chave: Avaliação Nutricional; Convalescença; Desnutrição; Factores Socioeconómicos; Idoso; Quedas Acidentais; Úlceras de Pressão; Unidades de Hospitalares
Introduction
The Portuguese population is aging fast, from 1 125 458 (11.4%) habitants over 65 years old in 1981 to 1 693 493 (16.4%) in 2001 and to 2 010 064 (19%) in 2011, meaning that there are now 128 elders for every 100 youngsters.1
According to the American Society for Parental and Enteral Nutrition, malnutrition is a state which combines varying degrees of overnutrition or undernutrition that lead to change in body composition and diminished function.
Malnutrition is frequently described in the elderly, being a relevant healthcare problem by itself.2 It is also associated with other problems, including increased risks of falling3,4 or of developing pressure ulcers,5 poor rehabilitation outcome,6,7 increased length of hospital stay and higher mortality.8
An older population has higher healthcare needs and, sometimes, need for specialized care, due to frailty and higher frequency of hospital admissions. In Portugal, there is a network of institutions that provide continuity of healthcare and social support to people in a situation of dependence, called Rede Nacional de Cuidados Continuados Integrados (RNCCI). This network includes convalescence units with the objective of helping people recover autonomy and maximize quality of life.
Our aim was to characterize the population admitted to a convalescence unit and relate the nutritional status on ad- mission with independence for activities of daily living (ADL), risk of falling, risk of developing pressure ulcers and discharge destination.
Methods
A unicentric observational retrospective study was conducted. Clinical data from all patients over 65 years old admitted to a 30 bed RNCCI convalescence unit during an 18-month period (from July 2016 to December 2017) was analysed. Patients that had not been discharged by the end of the study period were excluded.
Data was obtained by review of the clinical files and included: socio-demographic variables (age in years, gender, length of stay in days and discharge destination in days), anthropometric measures (height, weight, mid-upper arm circumference, nutritional status [Mini Nutritional Assessment], independence for ADL [Katz ADL Scale], risk of falling [Morse Fall Scale], risk of developing pressure ulcers [Braden Scale] and socio-familial status [Gijon Scale]):
· Mini Nutritional Assessment (MNA) uses anthropometric measurements (weight, height and weight loss), global parameters (lifestyle, medication and mobility), dietary parameters (number of meals, food intake, fluid intake and autonomy of feeding) and subjective assessment (self-perception of health and nutrition) to distinguish, with very high sensitivity and specificity, 3 groups: adequate nutritional status (≥24), at risk for malnutrition (17-23.5) and protein-calorie undernutrition (<17).9-11
· The Katz ADL Scale assesses functional status on adequacy of performance of 6 functions (bathing, dressing, toileting, transferring, continence and feeding) using a 3-point scale, resulting in a score from 6 to 18, with a higher score associated with greater dependence.12 We chose to divide patients in 3 groups: independent (6), partially dependent (7-12) and completely dependent (>12).
· The Braden Scale is a tool for predicting the risk of developing pressure ulcers. Examining 6 criteria (sensory perception, skin moisture, physical activity, mobility, nutritional status and friction/shear), categorizes 5 groups: no risk (19-23 points), mild risk (15-18 points), moderate risk (13-14 points), high risk (10-12 points) and very high risk (<10 points).
· The Morse Fall Scale examines 6 criteria (history of falling, comorbidities, ambulatory aid, intravenous therapy, gait and mental status), categorizing 4 groups: no risk (0 points), low risk (1-25 points), moderate risk (25-45 points) and high risk (>45 points).
· The Gijon Scale evaluates socio-familial status using 5 criteria (familial situation, economic situation, habitation, social relationships and support from surrounding community), categorizing 3 groups: good/acceptable social situation (5-9 points), at risk of social problem (10-14 points) and established social problem (≥15 points).
Data was systematically collected at patient’s admission in the unit. Data was presented in absolute (n) and relative values (%). Patients were compared according to MNA as at risk of malnutrition or undernourished.
All statistical analysis was performed using SPSS Statistics v20.0 Due to large sample size parametric tests were applied. The student t-test was used for continuous variables, and the chi-square test was used for categorical variables. Pearson correlation was used to measure the statistical association between two continuous variables. A 2-tailed value of p<0.05 was considered significant.
Results
Population: During the 18-month period, 181 patients fulfilled the chosen criteria. Gender distribution had a slight predominance of females (57.5%, n = 104) and age was 80.0 ± 7.1 years old. Most came from an acute care hospital (53.6%, n = 97) or from home (37.0%, n = 67), with the remainder (9.4%, n = 17) coming from another continuing care facility (including nursing homes). The length of stay was 54.6 ± 25.8 days.
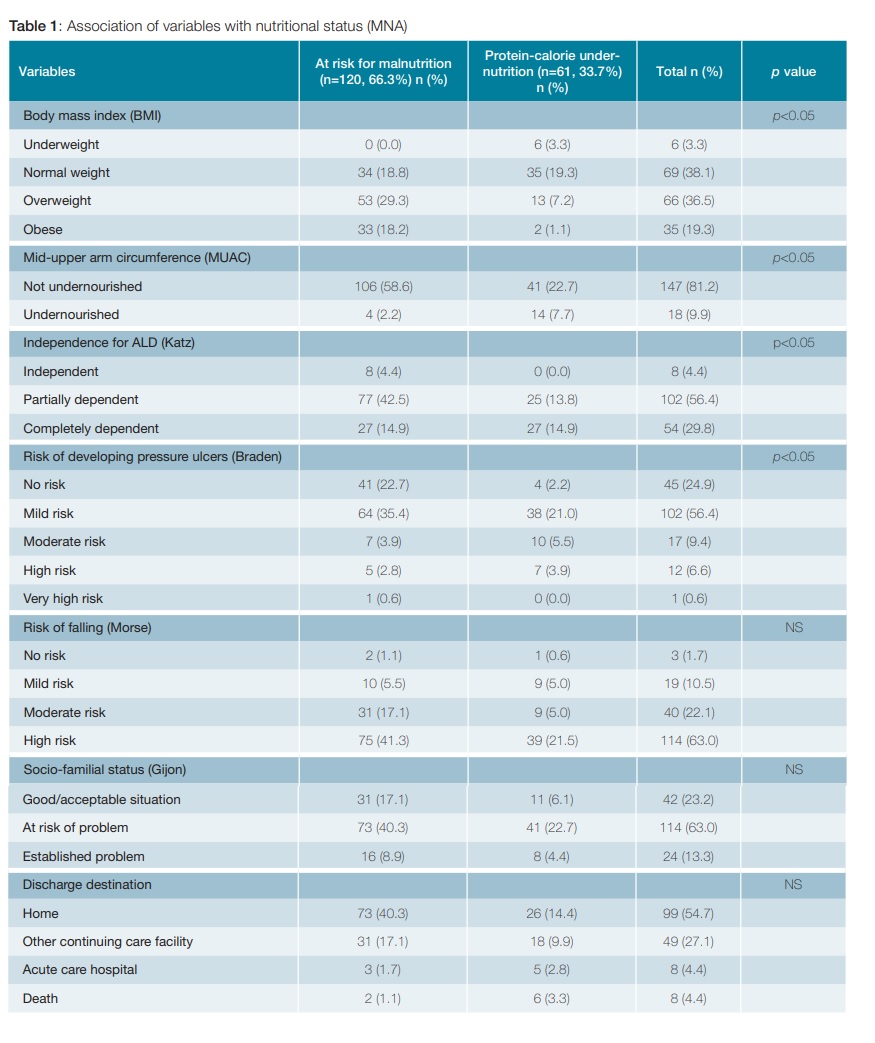
Nutritional status: According to the MNA, 33.7% (n = 61) of the population had protein-calorie undernutrition and all the others (66.3%, n = 120) were at risk for malnutrition – Table 1.
The body mass index (BMI) was 26.1 ± 4.8, with 38.1% (n = 69) classified as normal weight, 3.3% (n = 6) as underweight and 55.8% (n = 101) as overweight/obese – Table 1. All underweight patients had been classified by the MNA as having protein-calorie undernutrition. As expected, a strong positive correlation between BMI and MNA was found (p = 0.508, p < 0.001).
Mid-upper arm circumference (MUAC) measurements classified the large majority (81.2%, n = 147) as not undernourished – Table 1. Of the 18 patients (9.9%) classified as undernourished according to MUAC, 77.8% (n = 14) had also been classified by the MNA as having protein-calorie undernutrition. Also as expected, a strong positive correlation between
MUAC and MNA was found (p = 0.553, p < 0.001).
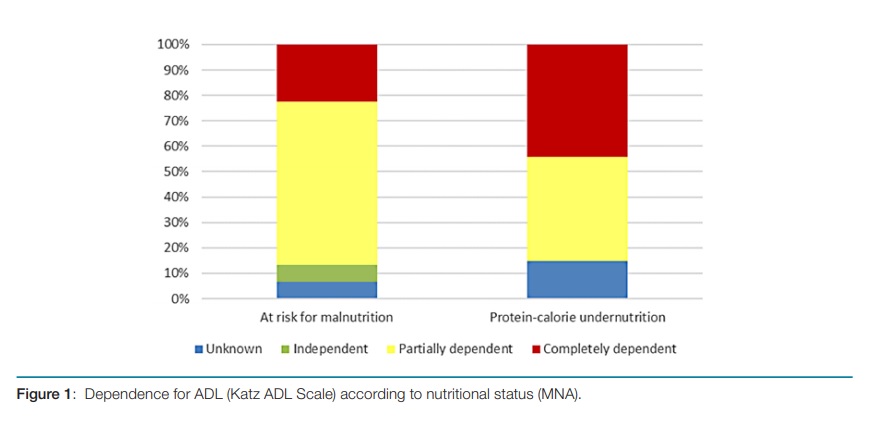
Independence for ADL: The majority of this population was partially (56.4%, n = 102) or completely dependent (29.8%, n = 54) for ADL, with only 4.4% (n = 8) being fully independent – Table 1 and Fig. 1. Differential analysis showed an inverse moderate correlation with the nutritional status (p =-0.427, p < 0.001), meaning that protein-calorie under nutrition is associated with greater dependence.
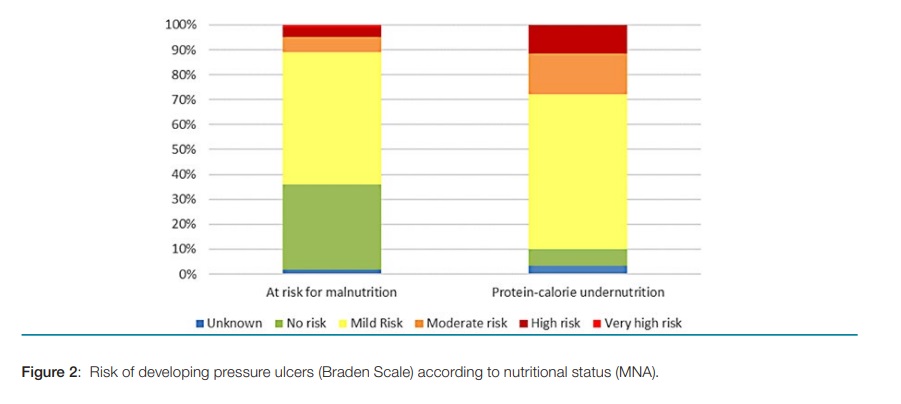
Risk of developing pressure ulcers: Using the Braden Scale, we found that the majority had either no risk (24.9%, n = 45) or mild risk (56.4%, n = 102) of developing pressure ulcers – Table 1 and Fig. 2. Differential analysis showed a moderate positive correlation with the nutritional status (p = 0.372, p < 0.001).
Risk of falling: According to the Morse Fall Scale, most of the population (63.0%, n = 114) had high risk of falling – Table 1. Differential analysis based on nutritional status showed no correlation.
Socio-familial status: Using the Gijon Scale, we found that most of this population (63.0%, n = 114) was at risk of social problems or had already an established social problem (13.3%, n = 24) – Table 1. There was no correlation between socio-familial status and nutritional status.
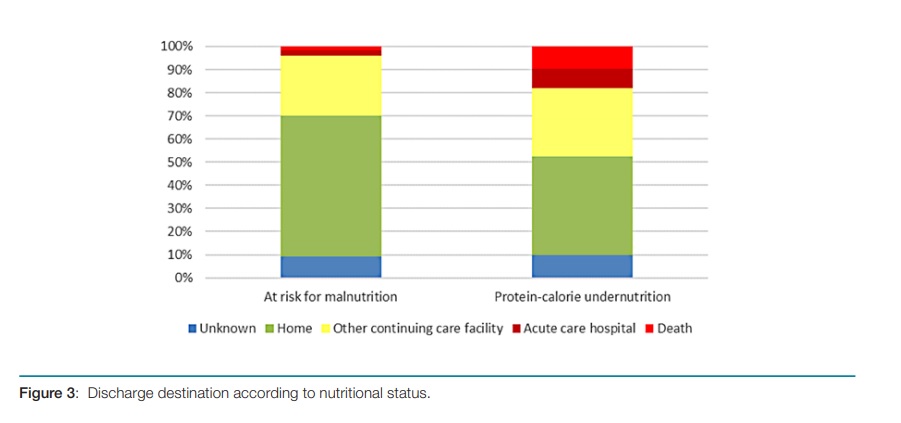
Discharge destination: The majority (54.7%, n = 99) of the patients was discharged home, 27.1% (n = 49) were trans- ferred to another continuing care facility, 4.4% (n = 8) were transferred to acute care hospitals and 4.4% (n = 8) died – Table 1. Although there was a higher percentage of deaths and transfers to acute care hospitals or other continuing care facilities in undernourished patients – Fig. 3 – we found no statistical significance in this association.
Discussion
We believe the chosen criteria provides a good representation of the elderly population that is admitted to Convalescence Units. The fact that half had come from an acute care hospital is relevant, but in accordance with the expected higher need for medical care in this population. The length of stay was highly variable, reflecting the heterogeneity of rehabilitation needs.
Using the MNA, we found that all patients were at least at risk of malnutrition, with about a third being undernourished. A strong positive correlation between MNA and both BMI and MUAC was found, reinforcing the high sensitivity and specificity of the MNA evaluation. Analysing only the BMI and the MUAC, only a very small part was classified as underweight/ undernourished, supporting the assumption that anthropometric measures by themselves have a low sensitivity and are insufficient as screening tools for nutritional status.13,14
We found that only a small minority of this population was fully independent and that patients with greater dependence for ADL also have a higher risk of malnutrition. This is in accordance with other published data.15
We found a high incidence of socio-familial problems and high risk of falling in our sample. However, neither of these factors had a significant relation with nutritional status, probably meaning a multifactorial etiology.2-4 However, socio-familial status is a well-known important factor for malnutrition and should be kept in mind when trying to find long-term solutions to this huge problem.
We found that over 80% of the population had mild or even no risk of developing pressure ulcers. However, we found a statistically significant relation between the nutritional status and the risk of developing pressure ulcers. Bearing in mind that pressure ulcers are a very significant problem in the elder, this constitutes an important alert that nutritional evaluation and support may have a crucial role in people’s quality of life.
The discharge destination shows that, although the majority was able to return home, a considerable part needed continued support in another continuing care facility. The number of patients that needed to be transferred to an acute care hospital or that died in this unit reflects the frailty and complexity of this elderly population.
Conclusion
There are complex associations between age, malnutrition, dependence for ADL, socio-familial problems, risk of falling, risk of developing pressure ulcers and general health.
Nutritional assessment in the elderly is a complex diagnostic procedure that should include not only anthropometric measures, but also standardized assessment tools and other clinical parameters as they constitute an important early alert to the need of nutritional support.
Our findings, namely the high prevalence of malnutrition and the associated increased risk for complications, are concerning and support the recommendations to routinely screen for malnutrition and provide nutritional support in all health care settings.9
To the best of our knowledge, this was the first survey of malnutrition and associated issues carried out in a Convalescence Unit of the RNCCI in Portugal. It would be useful that similar research was carried out in other national institutions for the evaluation and comparison of results, in order to better define measures to be adopted in clinical practice in the future.
REFERENCES
1. Instituto Nacional de Estatística. Censos 2011 Resultados Definitivos - Portugal.Lisboa: INE; 2012. [ Links ]
2. Donini LM, Scardella P, Piombo L, Neri B, Asprino R, Proietti AR, et al. Malnutrition in elderly: Social and economic determinants. J Nutr Heal Aging. 2013;179-15. doi: 10.1007/s12603-012-0374-8. [ Links ]
3. Westergren A, Hagell P, Sjodahl Hammarlund C. Malnutrition and risk of falling among elderly without home-help service: a cross sectional study. J Nutr Health Aging. 2014;18:905-11. doi: 10.1007/s12603-014-0469-5. [ Links ]
4. Neyens J, Halfens R, Spreeuwenberg M, Meijers J, Luiking Y, Verlaan G, et al. Malnutrition is associated with an increased risk of falls and impaired activity in elderly patients in Dutch residential long-term care (LTC): A cross-sectional study. Arch Gerontol Geriatr. 2013;56:265-9. doi: 10.1016/j.archger.2012.08.005. [ Links ]
5. Brito PA, Generoso S de V, Correia MI. Prevalence of pressure ulcers in hospitals in Brazil and association with nutritional status - A multicenter, cross-sectional study. Nutrition. 2013;29:646-9. doi: 10.1016/j.nut.2012.11.008. [ Links ]
6. Marshall S, Bauer J, Isenring E. The consequences of malnutrition following discharge from rehabilitation to the community: A systematic review of current evidence in older adults. J Hum Nutr Diet. 2014;27:133-41. doi: 10.1111/jhn.12167. [ Links ]
7. Wakabayashi H, Sashika H. Malnutrition is associated with poor rehabilitation outcome in elderly inpatients with hospital-associated deconditioning: a prospective cohort study. J Rehabil Med. 2014;46:277-82. doi: 10.2340/16501977-1258. [ Links ]
8. Rasheed S, Woods RT. Malnutrition and Associated Clinical Outcomes in Hospitalized Patients Aged 60 and Older: An Observational Study in Rural Wales. J Nutr Gerontol Geriatr. 2013;32:71-80. doi: 10.1080/21551197.2012.753772. [ Links ]
9. Cederholm T, Barazzoni R, Austin P, Ballmer P, Biolo G, Bischoff SC, et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin Nutr. 2017;36:49-64. doi: 10.1016/j.clnu.2016.09.004. [ Links ]
10. Vellas B, Guigoz Y, Garry PJ, Nourhashemi F, Bennahum D, Lauque S, et al. The mini nutritional assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition. 1999;15:116-22. doi: 10.1016/S0899-9007(98)00171-3. [ Links ]
11. Guigoz Y, Vellas B, Garry P. Mini Nutritional Assessment: a practical assessment tool for grading the nutritional state of elderly patients. Facts Res Gerontol. 1994;4(suppl 2):15-59. [ Links ]
12. Katz S, Ford A, Moskowitz R, Jackson B, Jaffe M. Studies of Illness in the Aged - The Index of ADL: A Standardized Measure of Biological and Psychosocial Function. JAMA. 1963;185:914. doi: 10.1001/jama.1963.03060120024016. [ Links ]
13. Barkoukis H. Nutrition Recommendations in Elderly and Aging. Med Clin North Am. 2016;100:1237-50. doi: 10.1016/j.mcna.2016.06.006. [ Links ]
14. Volkert D, Beck AM, Cederholm T, Cruz-Jentoft A, Goisser S, Hooper L, et al. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin Nutr. 2018. doi: 10.1016/j.clnu.2018.05.024. [ Links ]
15. Streck DR, Eggert E, Sobottka E, Adams T, Moretti CZ. Research, participation and social transformation: Notes on the unfolding of a research practice. Int J Action Res. 2011;7:175-95. doi: 10.1688/1861-9916_IJAR_2011_02_Streck. [ Links ]
Responsabilidades Éticas
Conflitos de Interesse: Os autores declaram a inexistência de conflitos de interesse na realização do presente trabalho.
Fontes de Financiamento: Não existiram fontes externas de financiamento para a realização deste artigo.
Confidencialidade dos Dados: Os autores declaram ter seguido os protocolos da sua instituição acerca da publicação dos dados de doentes.
Proteção de Pessoas e Animais: Os autores declaram que os procedimentos seguidos estavam de acordo com os regulamentos estabelecidos pelos responsáveis da Comissão de Investigação Clínica e Ética e de acordo com a Declaração de Helsínquia da Associação Médica Mundial.
Proveniência e Revisão por Pares: Não comissionado; revisão externa por pares.
Ethical Disclosures
Conflicts of interest: The authors have no conflicts of interest to declare. Financing Support: This work has not received any contribution, grant or scholarship
Confidentiality of Data: The authors declare that they have followed the protocols of their work center on the publication of data from patients.
Protection of Human and Animal Subjects: The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Provenance and Peer Review: Not commissioned; externally peer reviewed.
© Autor (es) (ou seu (s) empregador (es)) e Revista SPMI 2020. Reutilização permitida de acordo com CC BY-NC. Nenhuma reutilização comercial.
© Author(s) (or their employer(s)) and SPMI Journal 2020. Re-use permitted under CC BY-NC. No commercial re-use.
Correspondence / Correspondência:
Miguel Ardérius – miguel_arderius@hotmail.com
Serviço de Medicina III, Centro Hospitalar Lisboa Norte, Lisboa, Portugal
Avenida Professor Egas Moniz
1649-035 Lisboa
Received / Recebido: 12/02/2020
Accepted / Aceite: 16/08/2020
Publicado / Published: 28 de Setembro de 2020


{kind=link}
{kind=link}
{kind=link}
{kind=link}