










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkMedicina Interna
versão impressa ISSN 0872-671X
Medicina Interna vol.27 no.3 Lisboa jul. 2020
https://doi.org/10.24950/O/34/20/3/2020
ARTIGOS ORIGINAIS / ORIGINAL ARTICLES
Gender Differences in Acute Ischemic Stroke Treatment
Diferenças de Género no Tratamento de Fase Aguda do Acidente Vascular Cerebral Isquémico
Anna Taulaigo1  https://orcid.org/0000-0003-3475-4647
https://orcid.org/0000-0003-3475-4647
Bárbara Pedro2 https://orcid.org/0000-0003-0862-6262
Marisa Mariano3 https://orcid.org/0000-0002-1814-2854
Ana Paiva Nunes3 https://orcid.org/0000-0002-5573-1551
1Unidade Funcional Medicina 2, Hospital Curry Cabral, Centro Hospitalar Universitário de Lisboa Central, Lisboa, Portugal.
2Serviço de Medicina 2, Hospital Professor Doutor Fernando Fonseca, Amadora, Portugal.
3Unidade CerebroVascular do Centro Hospitalar Universitário de Lisboa Central, Lisboa, Portugal.
Abstract:
Introduction: In order to personalize stroke treatment, it is important to know if there are differences between genders in clinical features, acute phase treatment and outcomes.
Material and Methods: Longitudinal retrospective study that included patients with ischemic stroke, admitted in a stroke unit during a 30 months period and treated with thrombectomy with or without thrombolysis. The objective was to assess gender differences.
Results: Of 594 patients included, 50% were women. At admission, women had higher median age (78 vs 73 years), higher modified Rankin Score (mRS) and higher median National Institutes of Health Stroke Scale (NIHSS). No gender differences were found in treatment type, median time between symptoms onset and computed tomography, between computed tomography and thrombolysis and with respect to revascularization success. Disability expressed by mRS and mortality at 3 months were similar between genders. More women had atrial fibrillation (AF) (51% vs 35%), nevertheless, less women with known AF were receiving anticoagulant therapy before the event, compared to men (38% vs 52%).
Discussion: Even if women were older and had worse premorbid functional status, no gender differences were evident with regard to acute phase treatment efficacy and medium-term outcomes.
Conclusion: In women, age should not limit acute phase treatment of stroke and decisions should be individualized.
Keywords: Brain Ischemia/drug therapy; Sex Factors; Stroke/drug therapy.
Resumo:
Introdução: Na abordagem personalizada do acidente vascular cerebral (AVC) é importante definir se existem diferenças de género relativamente às caraterísticas clínicas, tratamento de fase aguda e resultados.
Material e Métodos: Estudo longitudinal retrospetivo que incluiu doentes com AVC isquémico admitidos na Unidade Cerebro Vascular, durante 30 meses, tratados com trombectomia com ou sem trombólise prévia, com o objetivo de avaliar diferenças de género.
Resultados: De 594 doentes, 50% eram mulheres apresentando, à admissão, idade mediana maior (78 vs 73 anos), maior pontuação na escala modificada de Rankin (mRS) e na National Institutes of Health Stroke Scale (NIHSS). Não houve diferenças no tipo de tratamento, no tempo mediano entre o início dos sintomas e tomografia computadorizada (TC), entre o tempo TC-trombólise ou na eficácia da revascularização. A disabilidade expressa pelo valor de mRS e a mortalidade aos 3 meses foram sobreponíveis entre géneros. Mais mulheres sofriam de fibrilhação auricular (FA) (51% vs 35%), no entanto menos mulheres com FA conhecida recebiam terapêutica anticoagulante antes do evento, comparativamente aos homens 38% vs 52%).
Discussão: Apesar das mulheres apresentarem idade mais elevada e maior grau de dependência, não existiram diferenças de género na eficácia do tratamento de fase aguda nem nos resultados a médio prazo.
Conclusão: No género feminino, a idade não deve constituir uma limitação à realização de terapêutica de fase aguda do AVC.
Palavras-chave: Acidente Vascular Cerebral/tratamento farmacológico; Factores Sexuais; Isquemia Cerebral/tratamento farmacológico.
Introduction
Worldwide, stroke is the second leading cause of death and the first one of long-term disability.1 There is increasing recognition of gender differences with regard to stroke risk factors, etiology and symptoms, but gender effect on outcomes and response to treatment is less clear. Overall, stroke is more prevalent in men, with an age-adjusted man: woman ratio of 1.41, except in the age group of more than 85 years, where it is more prevalent in women.2,3 However, women have a higher risk of stroke throughout their lives than men, which is attributed to the fact that they have a higher average life expectancy and accumulation of risk factors is considered more likely.2-4
When stroke is experienced, women are on average about four years older than men, and the premenopausal phase gives native cerebrovascular protection provided by sex hormones.2,3,5 So, age is the most important independent risk factor for stroke, as well as a negative predictor of clinical outcome, as showed in studies conducted in different ethnicities.4-6 There are differences in risk factor profiles between men and women, for example, hypertension and atrial fibrillation are more frequent in women. However, not only do risk factors and their distribution vary by gender, but also their associated effect, estimated by relative risk. For example, although diabetes mellitus is more prevalent in men with stroke, it has a stronger effect on stroke risk in women (relative risk of 2.1-6.6 in women versus 1.3-2.3 in men). The same is true for metabolic syndrome and tobacco.7,8 Moreover women have female-specific risk factors related to endogenous hormones, exogenous hormones and pregnancy/puerperium, even if their role in risk prediction is not completely understood.9 Stroke of ischemic etiology and intracerebral hemorrhage are more frequently observed in men (ratio man: woman of 1.55 and 1.60, respectively), while subarachnoid hemorrhage is more frequent in women (ratio man: woman of 0.84).2 According to the National Institutes of Health Stroke Scale (NIHSS), there are more women (44%) than men (36%) experiencing more severe stroke. In addition, the frequency of in-hospital medical complications and death is higher among women, and even those who survive, disability is more severe.10,11 Mortality rate between men and women less than 45 years old is identical, but in the 45-74 age group, women have lower mortality rates, however this advantage decreases with advancing age.5 Effort is being made to better understand gender differences with regards to stroke treatment and outcomes, but results are heterogeneous and inconsistent. Most of the data derives from studies that have not been conducted exclusively to assess this purpose. Understanding gender differences in stroke is crucial to reduce disparities and provide prompt, equitable and personalized treatment.
Material and Methods
STUDY DESIGN AND POPULATION
The study is a retrospective longitudinal study. We adopted the following inclusion criteria:
1) Patients admitted to the Stroke Unit of Hospital de São José with the diagnosis of Acute Ischemic Stroke, between January 1, 2016 and June 30, 2018;
2) Age ≥ 18 years old;
3) Acute phase treatment that included thrombectomy (isolated thrombectomy versus thrombectomy and thrombolysis);
4) Thrombectomy performed in our center. Regarding exclusion criteria, we excluded patients < 18 years old, but we did not establish an upper age limit and patients were considered eligible if inclusion criteria were satisfied. Moreover, we decided to exclude patients who underwent thrombectomy in other centers, because thrombectomy is considered an operator-dependent technique and the results might be influenced by the volume of procedures in each center. With respect to thrombolysis, some patients received thrombolysis in the hospital of admission and were transferred to our center to perform endovascular treatment, following acute phase treatment protocol established in Lisbon metropolitan area.
DATA COLLECTION
Data were obtained from the platform Safe Implementa- tion of Treatment in Stroke (SITS)’, an anonymous prospective international registry of all acute stroke patients submitted to acute reperfusion therapies.
VARIABLES
Premorbid functional status was defined with the modified Rankin Scale (mRS).12 A mRS ≤ 2 indicates good functional status without dependency in activities of daily living. A Stroke severity was expressed by the National Institutes of Health Stroke Scale (NIHSS).13 Results of the revascularization treatment were expressed by modified Treatment in Cerebral Ischemia Scale (mTICI), with a grade of 2b or 3 indicating a satisfactory revascularization result.14
OUTCOMES
The primary endpoint was to assess gender differences regarding risk factors, severity, treatment and prognosis in patients undergoing acute phase stroke treatment with thrombectomy (isolated thrombectomy versus thrombectomy and thrombolysis). The secondary endpoint was to perform a sub-group analysis according to the occlusion location: M1 occlu- sion (M1), M2 occlusion (M2) or basilar occlusion (BA).
STATISTICAL ANALYSIS
Continuous variables with non-normal distribution were expressed as median (interquartile range, IQR), as well as ordinal variables. Comparisons between continuous variables with a non-normal distribution were made using non-parametric tests. Dichotomous categorical variables were compared using Chisquare test. With respect to categorical variables, percentages refer to column percentages. Binary logistic regression was used to further explore association between gender and clinical variables. Variables suggesting a statistically significant gender difference at bivariate analysis were included in the logistic regression analysis. The goodness-of-fit of the model was evaluated with the Hosmer-Lemeshow test (with p < 0.05 indicating poor fit). Due to smaller sample sizes, multivariate analysis was not performed in subgroups. All statistical analyses were performed using version 23.0 of SPSS for Windows® (SPSS Inc., Chicago, IL, USA). For all tests, a p value < 0.05 was considered statistically significant. Logistic regression results were expressed as odds ratios (OR) and 95% confidence interval (CI).
RESULTS
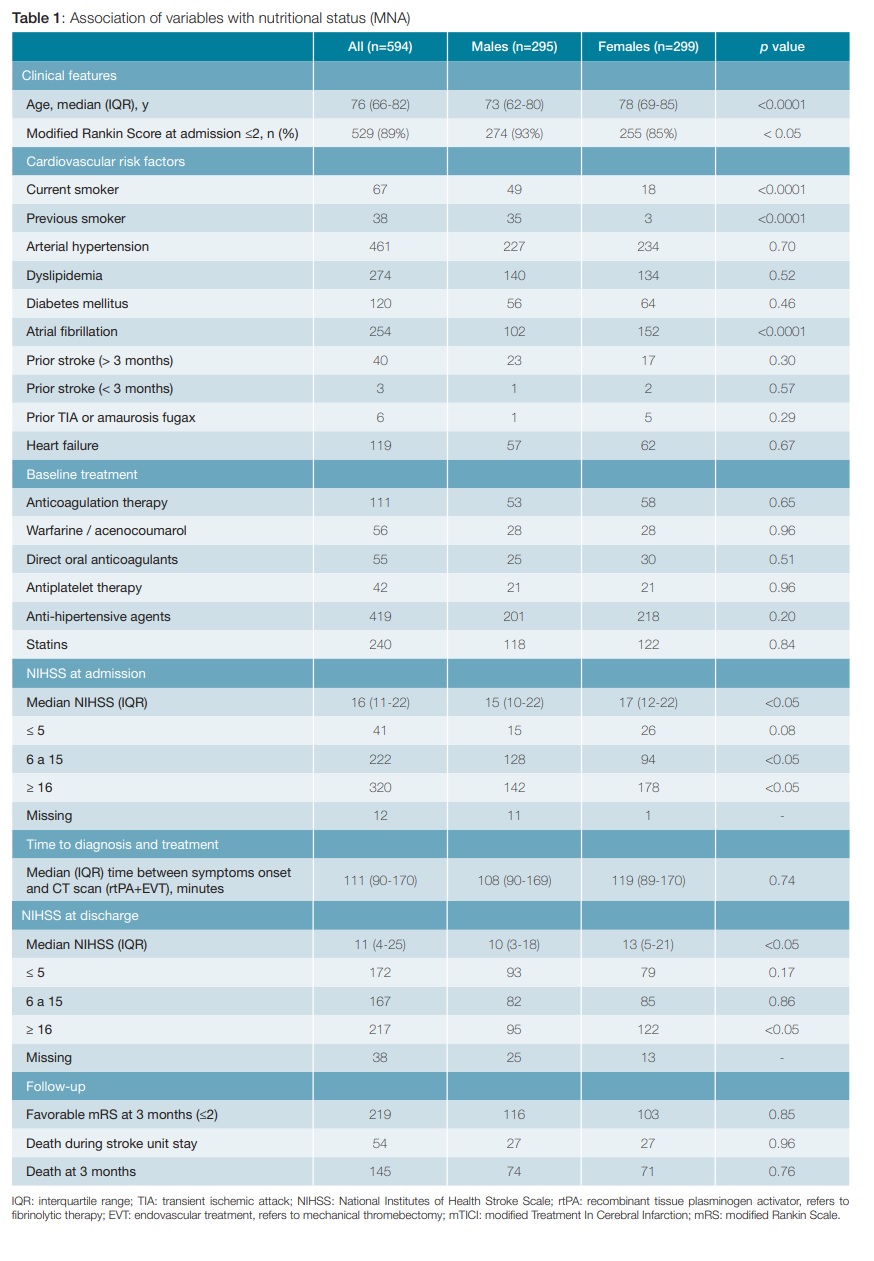
Among 669 patients evaluated, 594 satisfied inclusion criteria. Two patients were less than 18 years old and 73 patients did not undergo mechanical thrombectomy in our center. Males were 295 (49.7%) and females 299 (50.3%). Considering vas- cular territory submitted to thrombectomy, 259 patients had a medium cerebral artery (MCA) segment M1 occlusion, 74 patients had a MCA segment M2 occlusion and 42 patients had a basilar artery occlusion. Patients’ characteristics are sum- marized in Table 1. Median age (IQR) was 76 (66-82) years, higher in females (78 vs 73 years; p < 0.0001). Modified Rankin Scale (mRS) at admission was ≤ 2 in 93% of males and 85% of females (p < 0.05).
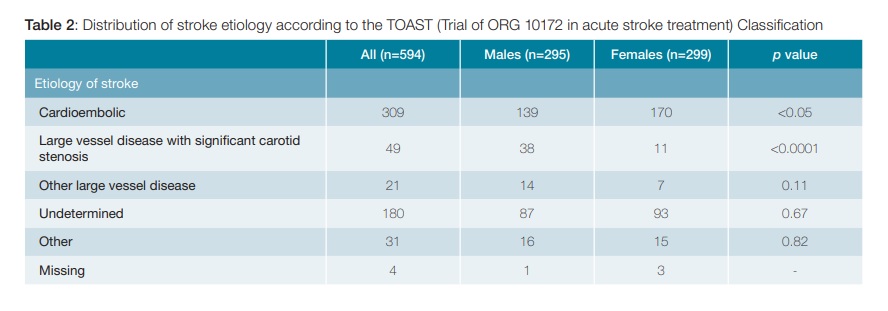
With regards to cardiovascular risk factors, current or previous tobacco use was more common in men (28.5% vs 7%; p < 0.0001), while known atrial fibrillation was more common in women (51% vs 35%; p < 0.0001). There was no difference between genders in therapy at baseline. Median (IQR) NIHSS at presentation was 16 (11-22), significantly higher in females (17 vs 15; p 0.04). Intermediate NIHSS values (6-15) were more common in male patients, while high values (>15) were more common in female patients, with statistically significant difference (p < 0.05). Median (IQR) time from symptoms onset to first brain CT scan was 111 (90-170) minutes and median (IQR) time from CT scan to fibrinolytic therapy was 18 (8-33) minutes. No differences in gender were evident from this data. Patients submitted to fibrinolytic therapy and mechanical thrombectomy were 331 (55.7%), while 263 (44.3%) received only mechanical thrombectomy. Final modified Treatment in Cerebral Infarction score (mTICI) was favorable (2b or 3) in 82.3% of patients, with no gender differences with statistical significance. When evaluating clinical outcomes, median NIHSS at discharge was significantly higher in females than males (13 vs 10; p = 0,013). Functional outcome was favorable (mRS ≤ 2) at three months in 37% of patients, with no gender differences. No gender differences were evident regarding inpatients’ mortality (54 patients; 9%), as well as three months mortality (145 patients; 24%). Data on stroke etiology are shown in Table 2. Overall, the most frequent etiology was cardioembolic stroke (309; 52%), followed by stroke by undetermined source (180; 30%) and large vessel atherosclerosis with significant carotid stenosis (49; 8%). While the former was significantly more common in women (57 vs 47%; p < 0.05), the latter was more prevalent in men (13 vs 4%; p < 0.0001).
Age, premorbid functional status expressed by mRS, atrial fibrillation, previous or current tobacco use, stroke severity at admission and discharge (NIHSS), cardioembolic etiology and large vessel disease with significant carotid stenosis were included in the logistic regression analysis, using gender as a dependent variable (data not shown in tables). The Hosmer-Lemeshow p value for the model was 0.17. Compared to men, females were older (OR 1.03; 95% CI 1.02-1.04; p 0.03) and more frequently had a mRS >2 (OR 2.0; 95% CI 1.1-3.6; p 0.02). Regarding risk factors, women had more AF (OR 2; 95% CI 1.2-3.5; p 0.01) but were less likely smokers (OR 0.4; 95% CI 0.2-0.8; p 0.007) or previous smokers (OR 0.08; 95% CI 0.02-0.26; p < 0.0001). Despite a trend for more severe strokes in women, multivariate analysis did not confirm the bi-variate analysis. There was no difference in females compared to males when considering NIHSS ≥ 16 (moderate to severe or severe strokes) at admission (OR 1.4, 95% CI 0.9-2-1; p 0.06) or discharge (OR 1; 95% CI 0.7-1.5; p 0.8). With respect to etiology, females were less likely to have large vessel disease with significant carotid stenosis (OR 0.3; 95% CI 0.1-0.6; p 0.002), but cardioembolic strokes were not more frequent in females overall (OR 0.6; 95% CI 0.3-1; p 0.06).
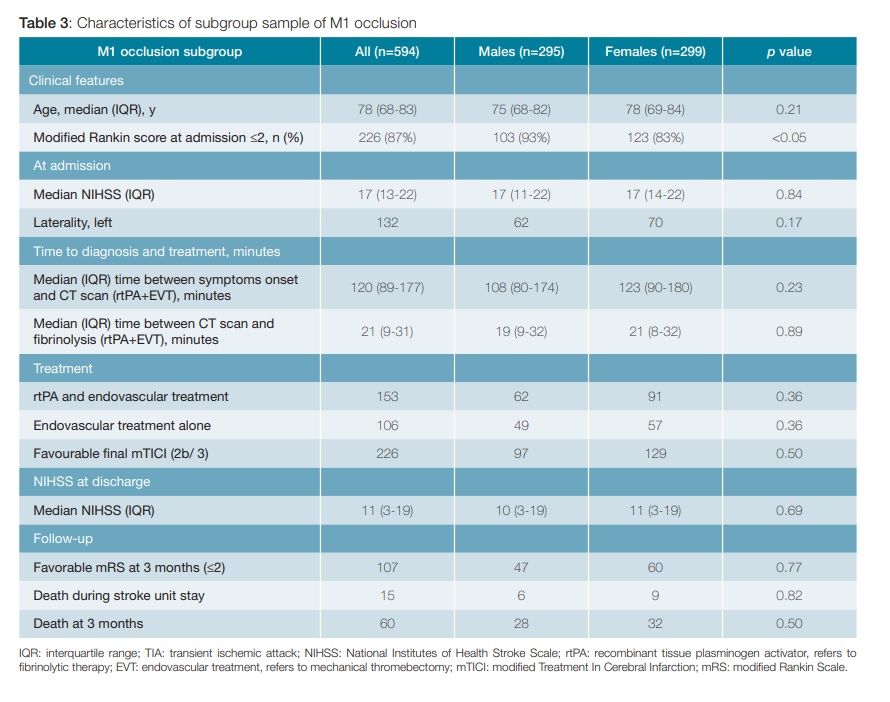
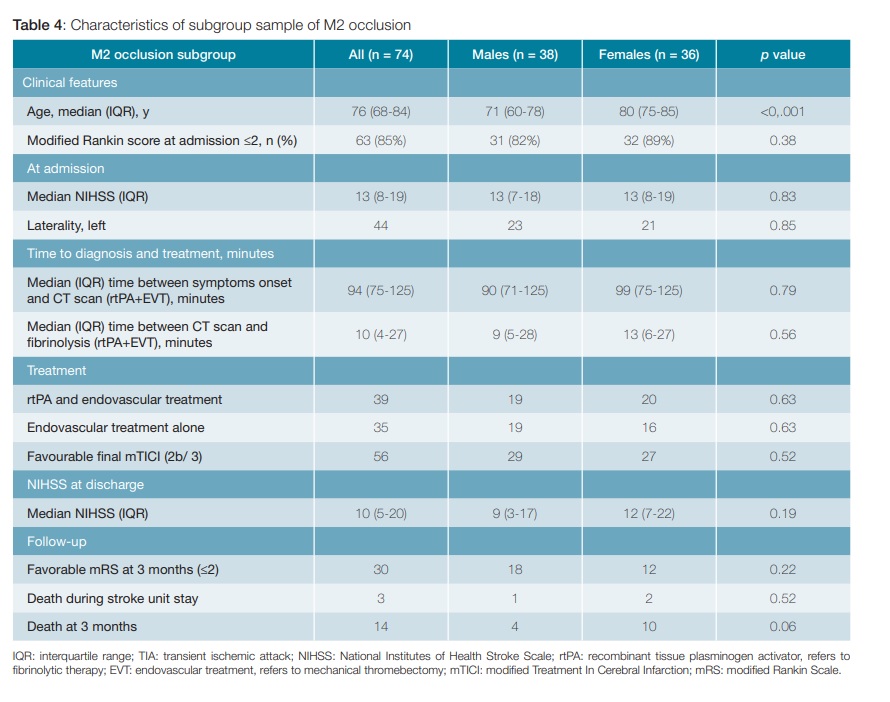
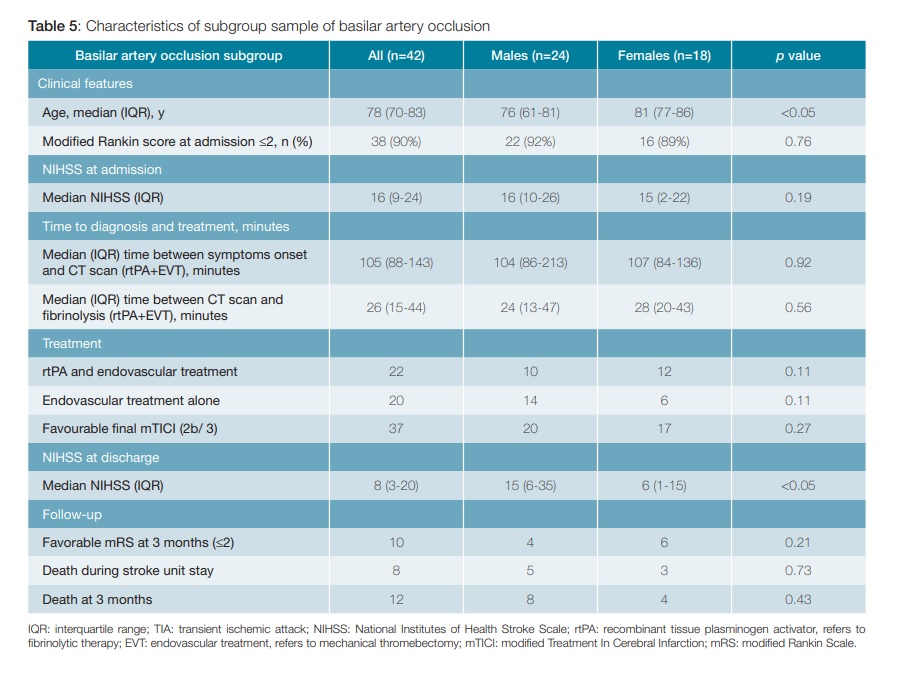
When we consider M1, M2 and BA subgroup, cardioembolic strokes are more frequent in women than men with BA occlusion, while large vessel atherosclerosis with significant carotid stenosis is more prevalent in men than women with M1 occlusion. In M1 occlusion subgroup, median age is similar between genders, however women had worse functional status at inclusion, having a mRS ≤ 2 in 83% of cases compared to 93% in males (p < 0.05) (Table 3). Subgroup analysis showed that women with M2 occlusion and BA occlusion are older than men (Table 4 and 5). With regards to laterality in MCA occlusions, there were no differences between men and women.
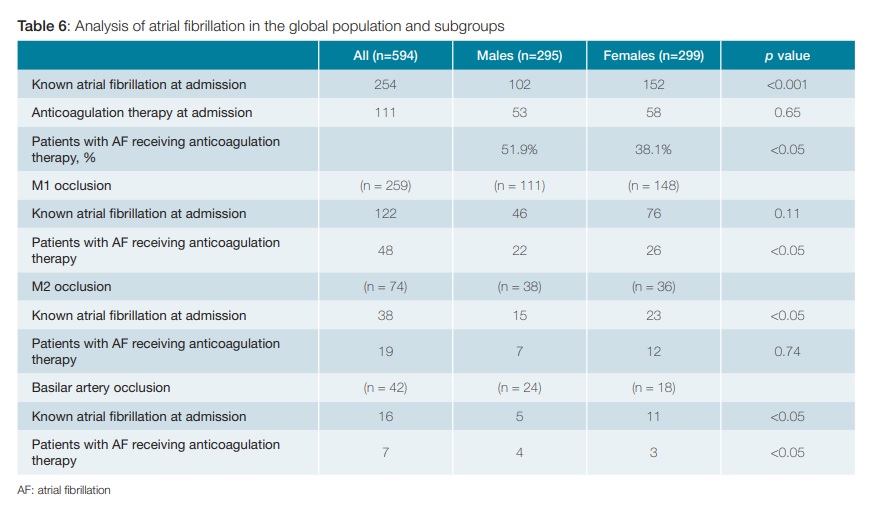
As shown in Table 3 and 4, no statistically significant gender differences were evident in M1 and M2 occlusion subgroup, when considering time to diagnosis, time to treatment, type of treatment received, success of revascularization, functional outcome and mortality. The NIHSS at discharge is similar between genders in M1 and M2 occlusion subgroups but is higher in males in BA occlusion group. Atrial fibrillation was more prevalent in females than males overall, and the difference still exists in M2 occlusion and BA occlusion subgroups (Table 6). Nevertheless, less women with known AF were receiving oral anticoagulation therapy at inclusion (38.1 vs 51.9%; p < 0.05). This difference was evident in M1 and BA occlusion subgroups as well. Due to shortness of stroke unit stay, data on anticoagulation at discharge were not analyzed.
Discussion
In this study of almost 600 patients with ischemic stroke, women presented stroke later in their life. However, age alone does not seem to be associated to worse outcome and this is relevant for acute phase treatment decisions. Men have a better premorbid functional status (mRS ≤2 in 93% of men versus 85% of women). Further studies are required to assess if premorbid functional status gender difference persists when adjusting for potential confounders, for example age and comorbidities.
Stroke severity at admission seems to be higher in women, although multivariate analysis did not confirm this data. According to the literature, pre-morbid disability and high stroke severity are in turn associated with poor stroke related functional outcomes.15 Some studies report more severe disability and higher in hospital mortality in women. In our work, despite premorbid disability and stroke severity at admission, women did not experience higher mortality rates and functional status seems to be comparable to men at 3 months follow-up. The main aim of acute phase treatment in stroke is to prevent long term disability and evaluation of gender differences in functional outcome is crucial. The benefit of hospitalization in a Stroke Unit is known and equal between genders, even if some works suggest that women might have longer length of stay, less functional recovery and less response to rehabilitation.16-20 In our population, outcomes at 3 months seem to be similar between genders. Nevertheless, the use of mRS as unique parameter to assess outcome might have limitations, for instance it does not distinguish between motor and cog- nitive disability. Moreover, a three months period is a limited time and it should be useful to assess a wider interval from stroke.
As expected, among risk factors atrial fibrillation is more prevalent in women, while tobacco use is more prevalent in men. In literature, cardioembolic etiology and atrial fibrillation are more frequent in women.21,22 We have also found this difference in the global population and in the subgroups M2 and BA occlusion in bivariate analysis. Acknowledging differences regarding stroke risk factors and etiology could be important in a primary prevention perspective. In our study, female patients with known AF were treated less frequently with anticoagulant therapy on admission (38.1% vs 51.9%; p <0.05) and this statistical difference between genders remains in the analysis of subgroups M1 and BA occlusion. It is important to note that there are contraindications to the use of anticoagulation, case by case evaluation was unfeasible and beyond the purpose of this work and this should be taken into account when interpreting this data. Nevertheless, it seems to suggest an existing disparity, which is in line with existing evidence, that can be improved with the education of health professionals and the reinforcement of rational medical considerations.23 This disparity might be related to the fact that women are older and with higher disability, leading clinicians to underestimate prevention benefit or overestimate bleeding risk and possible harm. In our opinion, age and comorbidities should not constitute an a priori contraindication to anticoagulation, as cardioembolic stroke is a preventable cause of morbidity and mortality.24 Further research and studies focusing on anticoagulation therapy prescription, compliance and tolerance are needed.
Other aspects unique to women are not specifically addressed in our study but are relevant both in primary and in secondary prevention. For instance, stroke risk should be taken in account when prescribing menopause hormone replacement therapy, which seems to lead to an increased risk.9
Regarding treatment eligibility, available data are heterogeneous. Most of the studies do not show gender differences in eligibility rates for intravenous thrombolysis. The most common exclusion criterion for both men and women is late arrival at the hospital. In contrast to most of the evidence, few works show that women could be less likely to receive thrombolysis than men. Moreover, some works suggest that women might have longer door-to-imaging and door-to-needle times. It is important to point out that most of the studies were not designed to assess gender differences as main objective. Studies that specifically assessed gender as outcome modifier with thrombolysis treatment were inconclusive.16,25-30 In our study no sex statistical differences were found in the choice of treatment (thrombolysis and/or thrombectomy). We also show similar times of median time between symptoms onset and CT scan, and median time between CT scan and fibrinolysis. Our findings emphasize that adherence with a stroke performance program not only improves care but also helps to avoid sex disparity. Nevertheless, we only included in our study patients who received acute phase treatment and it would be useful to conduct an analysis on patients who are considered not eligible, to assess if gender differences exist, for instance delayed arrival to the hospital in women as suggested by some literature. It is crucial to highlight that these aspects can be influenced by aspects like culture and educations, and results obtained in a particular context should not be generalized.16
With respect to endovascular treatment, there are no studies directly aimed to compare eligibility and outcomes of endovascular treatment in men and women with large vessel occlusion, but two recent post-hoc and subgroup analysis suggest no gender difference in treatment efficacy and outcomes.31,32 It is generally agreed that recanalization is the most important factor of good outcome in patients with ischemic stroke and large vessel occlusion, however this information is limited for genders.16 In our case, subgroup analysis is limited by small sample size and no data are available addressing gender issues in specific occlusion sites. Moreover, benefit of mechanical thrombectomy in basilar artery occlusion is still a matter of debate.33 In the subgroup analysis, there is only statistical differences related to age in the M2 and BA subgroup, with women being older than men. In the M1 subgroup, the age is similar between the two genders, however women have a greater degree of dependence. Analysis of etiology with respect to occlusion type was made (data not shown in tables). In the M1 occlusion, the etiology of large vessel disease with significant carotid stenosis is more prevalent in men, while in BA occlusion, the cardioembolic etiology is more prevalent in women, with statistical significance in both cases. Nevertheless, we would like to highlight equity in treatment access regarding times of intervention and choice of reatment between genders and comparable revascularization results.
The most important limitations of this study are the fact of being a retrospective study, with a small sample of subgroups. Moreover, modified Rankin Scale might not be the best way to express post morbid disability, hiding more subtle differences in functional outcome and quality of life. Besides that, the short length of hospitalization in our Stroke Unit limits the introduction of anticoagulant therapy, and it was not possible to verify if there was a gender difference in anticoagulation at discharge after identification of cardioembolic stroke.
Conclusion
Sex differences exist fundamentally with regard to higher age, higher dependency at admission in women and risk factors distribution as well. No substantial differences in symptoms-to-imaging times, access to thrombolysis or thrombectomy, or outcomes have been reported. Age should not limit acute phase treatment of stroke because decisions should be individualized. Much remains to be learned about differences in stroke between women and men. The reasons for gender disparity are multifactorial and additional tools are needed to help implement stroke quality improvement programs and interventions to reduce specific gender disparities in stroke care. Further research is needed to improve stroke risk profiles and treatments for both women and men, particularly on outcomes in elderly patients and on eligibility of women for endovascular procedures.
REFERENCES
1. Feigin VL, Nichols E, Alam T, Bannick MS, Beghi E, Blake N, et al. Global, regional, and national burden of neurological disorders, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18:459–80. doi: 10.1016/S1474-4422(18)30499-X
2. Appelros P, Stegmayr B, Terent A. Sex differences in stroke epidemiology: A systematic review. Stroke. 2009;40:1082–90. doi: 10.1161/STROKEA-HA.108.540781
3. Roger VL, Go AS, Lloyd-Jones DM, Adams RJ, Berry JD, Brown TM, et al. Heart disease and stroke statistics-2011 update: A report from the American Heart Association. Circulation. 2011;123:e18–209. doi: 10.1161/CIR.0b013e3182009701
4. Rojas JI, Zurrú MC, Romano M, Patrucco L, Cristiano E. Acute ischemic stroke and transient ischemic attack in the very old-risk factor profile and stroke subtype between patients older than 80 years and patients aged less than 80 years. Eur J Neurol. 2007;14:895–9. doi: 10.1111/j.1468-1331.2007.01841.x
5. Reeves MJ, Bushnell CD, Howard G, Gargano JW, Duncan PW, Lynch G, et al. Sex differences in stroke: epidemiology, clinical presentation, medical care, and outcomes. Lancet Neurol. 2008;7:915–26. doi: 10.1016/S1474-4422(08)70193-5
6. Seshadri S, Beiser A, Kelly-Hayes M, Kase CS, Au R, Kannel WB, et al. The lifetime risk of stroke: Estimates from the framingham study. Stroke. 2006;37:345–50. doi: 10.1161/01.STR.0000199613.38911.b2
7. Almdal T, Scharling H, Jensen JS, Vestergaard H. The independent effect of type 2 diabetes mellitus on ischemic heart disease, stroke, and death: A population-based study of 13 000 men and women with 20 years of follow-up. Arch Intern Med. 2004;164:1422–6. doi: 10.1001/archin-te.164.13.1422
8. Boden-Albala B, Cammack S, Chong J, Wang C, Wright C, Rundek T, et al. Diabetes, Fasting Glucose Levels, and Risk of Ischemic Stroke and Vascular Events: Findings from the Northern Manhattan Study (NOMAS). Diabetes Care. 2008;31:1132–7. doi: 10.2337/dc07-0797
9. Demel SL, Kittner S, Ley SH, McDermott M, Rexrode KM. Stroke Risk Factors Unique to Women. Stroke. 2018;49:518–23. doi: 10.1161/STROKEAHA.117.018415
10. Arboix A, Oliveres M, García-Eroles L, Maragall C, Massons J, Targa C. Acute Cerebrovascular Disease in Women. Eur Neurol. 2001;45:199–205. doi: 10.1159/000052130
11. Roquer J, Rodríguez Campello A, Gomis M. Sex differences in first-ever acute stroke. Stroke. 2003;34:1581–5. doi: 10.1161/01.STR.0000078562.82918.F6
12. van Swieten JC, Koudstaal PJ, Visser MC, Schouten HJ, van Gijn J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke. 1988;19:604–7. doi: 10.1161/01.str.19.5.604
13. Brott T, Adams HP, Olinger CP, Marler JR, Barsan WG, Biller J, et al. Measurements of acute cerebral infarction: a clinical examination scale. Stroke. 1989;20:864–70. doi: 10.1161/01.str.20.7.864
14. Zaidat OO, Yoo AJ, Khatri P, Tomsick TA, von Kummer R, Saver JL, et al. Recommendations on Angiographic Revascularization Grading Standards for Acute Ischemic Stroke. Stroke. 2013;44(9):2650–63. doi: 10.1161/STROKEAHA.113.001972
15. Lisabeth LD, Reeves MJ, Baek J, Skolarus LE, Brown DL, Zahuranec DB, et al. Factors Influencing Sex Differences in Poststroke Functional Outcome. Stroke. 2015;46:860–3. doi: 10.1161/STROKEAHA.114.007985
16. Bushnell C, Howard VJ, Lisabeth L, Caso V, Gall S, Kleindorfer D, et al. Sex differences in the evaluation and treatment of acute ischaemic stroke. Lancet Neurol. 2018;17:641–50. doi: 10.1016/S1474-4422(18)30201-1
17. Gattringer T, Ferrari J, Knoflach M, Seyfang L, Horner S, Niederkorn K, et al. Sex-related differences of acute stroke unit care: Results from the austrian stroke unit registry. Stroke. 2014;45:1632–8. doi: 10.1161/STROKEAHA.114.004897
18. Asdaghi N, Romano JG, Wang K, Ciliberti-Vargas MA, Koch S, Gardener H, et al. Sex Disparities in Ischemic Stroke Care: FL-PR CReSD Study (Florida-Puerto Rico Collaboration to Reduce Stroke Disparities). Stroke. 2016;47:2618–26. doi: 10.1161/STROKEAHA.116.013059
19. Lorenzano S, Ahmed N, Falcou A, Mikulik R, Tatlisumak T, Roffe C, et al. Does sex influence the response to intravenous thrombolysis in ischemic stroke?: Answers from safe implementation of treatments in stroke-international stroke thrombolysis register. Stroke. 2013;44:3401–6. doi: 10.1161/STROKEAHA.113.002908
20. Kamal N, Sheng S, Xian Y, Matsouaka R, Hill MD, Bhatt DL, et al. Delays in Door-to-Needle Times and Their Impact on Treatment Time and Outcomes in Get with the Guidelines-Stroke. Stroke. 2017;48:946–54. doi: 10.1161/STROKEAHA.116.015712
21. Wang TJ, Massaro JM, Levy D, Vasan RS, Wolf PA, D’Agostino RB, et al. A Risk Score for Predicting Stroke or Death in Individuals with New-Onset Atrial Fibrillation in the Community: The Framingham Heart Study. J Am Med Assoc. 2003;290:1049–56. doi: 10.1001/jama.290.8.1049
22. Friberg J, Scharling H, Gadsbøll N, Truelsen T, Jensen GB, Copenhagen City Heart Study. Comparison of the impact of atrial fibrillation on the risk of stroke and cardiovascular death in women versus men (The Copenha- gen City Heart Study). Am J Cardiol. 2004;94:889–94. doi: 10.1016/j.amj-card.2004.06.023
23. Glader E-L, Stegmayr B, Norrving B, Terént A, Hulter-Asberg K, Wester P-O, et al. Sex differences in management and outcome after stroke: a Swedish national perspective. Stroke. 2003;34:1970–5. doi: 10.1161/01.STR.0000083534.81284.C5
24. Benjamin EJ, Wolf PA, D’Agostino RB, Silbershatz H, Kannel WB, Levy D. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998;98:946–52. doi: 10.1161/01.cir.98.10.946
25. Park SJ, Shin S Do, Ro YS, Song KJ, Oh J. Gender differences in emergency stroke care and hospital outcome in acute ischemic stroke: A multicenter observational study. Am J Emerg Med. 2013;13:178–84. doi: 10.1016/j.ajem.2012.07.004
26. Kelly AG, Hellkamp AS, Olson D, Smith EE, Schwamm LH. Predictors of rapid brain imaging in acute stroke: Analysis of the get with the guidelines-stroke program. Stroke. 2012;43:1279–84. doi: 10.1161/STROKEAHA.111.626374
27. Ashkenazi L, Toledano R, Novack V, EIluz E, Abu-Salamae I, Ifergane G. Emergency department companions of stroke patients: implications on quality of care. Medicine. 2015;94:e520. doi: 10.1097/MD.0000000000000520 [ Links ]
28. Burton KR, Kapral MK, Li S, Fang J, Moody AR, Krahn M, et al. Predictors of diagnostic neuroimaging delays among adults presenting with symptoms suggestive of acute stroke in Ontario: a prospective cohort study. CMAJ Open. 2016;4:E331-7. doi: 10.9778/cmajo.20150110 [ Links ]
29. Madsen TE, Khoury JC, Alwell KA, Moomaw CJ, Kissela BM, De Los Rios La Rosa F, et al. Analysis of tissue plasminogen activator eligibility by sex in the Greater Cincinnati/Northern Kentucky stroke study. Stroke. 2015;46:717–21. doi: 10.1161/STROKEAHA.114.006737
30. Fredwall M, Sternberg S, Blackhurst D, Lee A, Leacock R, Nathaniel TI. Gender Differences in Exclusion Criteria for Recombinant Tissue-Type Plasminogen Activator. J Stroke Cerebrovasc Dis. 2016;25:2569–74. doi: 10.1016/j.jstrokecerebrovasdis.2016.06.012
31. Sheth SA, Lee S, Warach SJ, Gralla J, Jahan R, Goyal M, et al. Sex Diffe- rences in Outcome After Endovascular Stroke Therapy for Acute Ischemic Stroke. Stroke. 2019;50:2420–7. doi: 10.1161/STROKEAHA.118.023867
32. Chalos V, de Ridder IR, Lingsma HF, Brown S, van Oostenbrugge RJ, Goyal M, et al. Does Sex Modify the Effect of Endovascular Treatment for Ischemic Stroke? Stroke. 2019;50:2413–9. doi: 10.1161/STROKEAHA.118.023743
33. Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2018;49:e46–110. doi: 10.1161/STR.0000000000000158
Responsabilidades Éticas
Conflitos de Interesse: Os autores declaram a inexistência de conflitos de interesse na realização do presente trabalho.
Fontes de Financiamento: Não existiram fontes externas de financiamento para a realização deste artigo.
Confidencialidade dos Dados: Os autores declaram ter seguido os protocolos da sua instituição acerca da publicação dos dados de doentes.
Proteção de Pessoas e Animais: Os autores declaram que os procedimentos seguidos estavam de acordo com os regulamentos estabelecidos pelos responsáveis da Comissão de Investigação Clínica e Ética e de acordo com a Declaração de Helsínquia da Associação Médica Mundial.
Proveniência e Revisão por Pares: Não comissionado; revisão externa por pares.
Ethical Disclosures
Conflicts of interest: The authors have no conflicts of interest to declare. Financing Support: This work has not received any contribution, grant or scholarship
Confidentiality of Data: The authors declare that they have followed the protocols of their work center on the publication of data from patients.
Protection of Human and Animal Subjects: The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Provenance and Peer Review: Not commissioned; externally peer reviewed.
© Autor (es) (ou seu (s) empregador (es)) e Revista SPMI 2020. Reutilização permitida de acordo com CC BY-NC. Nenhuma reutilização comercial.
© Author(s) (or their employer(s)) and SPMI Journal 2020. Re-use permitted under CC BY-NC. No commercial re-use.
Correspondence / Correspondência:
Anna Taulaigo – annataulaigo@gmail.com
Unidade Funcional Medicina 2, Hospital Curry Cabral, Centro Hospitalar Universitário de Lisboa Central, Lisboa, Portugal.
R. Beneficência 8, 1050-099 Lisboa
Received / Recebido: 20/02/2020
Accepted / Aceite: 16/06/2020
Publicado / Published: 28 de Setembro de 2020


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}