











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
A 71-year-old woman was assessed for fatigue in a 20 m flat walk in the previous year. No alterations were found on physical examination. Blood tests were normal, including inflammation parameters, brain natriuretic peptide, thyroid function, and arterial blood gases. Transthoracic echocardiogram revealed preserved left ventricular systolic function, mild right atrial dilatation, mild right ventricular enlargement, elevated pulmonary artery (PA) systolic pressure (55 mmHg), and a large, rounded mass (24x12 mm) apparently adherent to the wall of the main PA, immediately distal to the pulmonary valve, mobile and non-obstructive (Fig. 1).
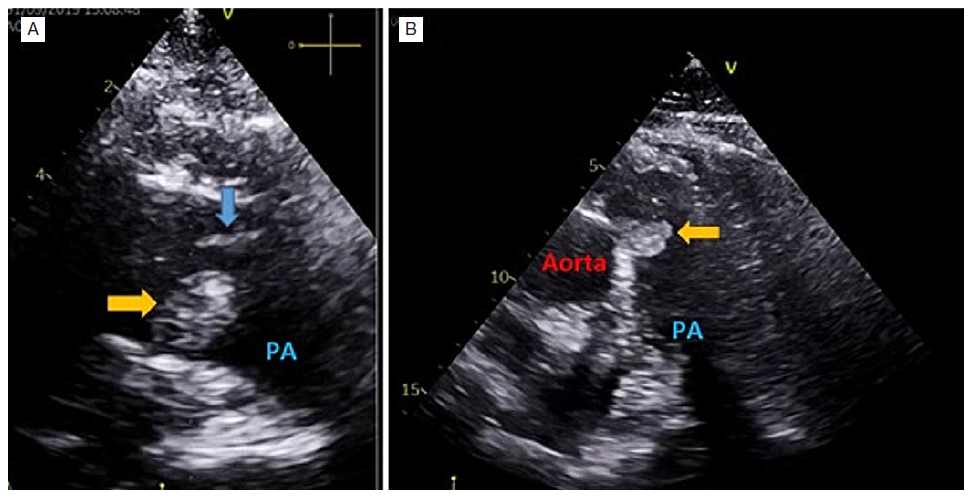
Figure 1: Transthoracic echocardiogram - parasternal short-axis view of the great vessels (A) and subcostal short-axis view (B) - show a rounded well delimitated homogenous mass (24x12 mm) (yellow arrow) apparently adherent to the medial wall of the main pulmonary artery, immediately distal to the pulmonary valve (blue arrow), mobile and non-obstructive .
Computed tomography angiography confirmed the PA mass (Fig. 2) and was suggestive of distal pulmonary thromboembolism (PTE).
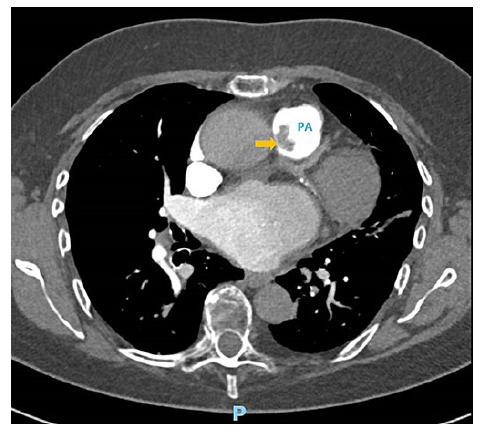
Figure 2: Computed tomography pulmonary angiography show a pulmonary artery mass (yellow arrow) without contrast enhancement or invasion of the surrounding structures.
Thus, the differential diagnosis comprised a thrombus or a tumor. Cardiac magnetic resonance and body positronemission tomography scan evidenced late gadolinium enhancement of the mass, suggestive of a tumor, without 18-FDG uptake, less suggestive of malignancy. No other lesions were found. Given the dimension and location of the mass and diagnostic uncertainty, the team decided for surgical excision. A gelatinous friable mass with a pedicle attached to the pulmonary valve was removed. The histological exam revealed a papillary fibroelastoma (PF). PF on the pulmonary valve is rare, with only 7% of cases described on this location.1 Pulmonary hypertension (PH) was admitted as a microembolization consequence of direct tumor embolization or possible thrombi formation within the fronds of the PF. An accurate differential diagnosis in the presence of a PA mass is crucial. An incorrect PTE diagnosis, the most frequent diagnosis in this setting, results in anticoagulant therapy initiation with potential adverse effects.2 The differential diagnosis between thrombus and intracardiac tumor depends on an integrated multimodality radiologic study.3,4Furthermore, the presence of PH in association with a PA mass should alert to the possibility of tumor embolization, an uncommon cause of group 4 PH.5

