











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Acute abdomen is an abdominal pain of abrupt onset, comprising a vast group of diagnoses, from a self-limiting illness to a life-threatening condition.1
Appendicitis, included within this group of diseases, is the most common surgical abdominal emergency worldwide and is caused by appendicular lumen obstruction, which can lead to high mortality and morbidity.1,2Although this diagnosis is clinical, there are some cases where it is difficult to distinguish from the different acute abdominal conditions.3
The use of ultrasound (US) in the emergency department (ED) has become widespread, but given the time constraint and patients' critical conditions, there is a need for a focused and specific approach according to patients' symptoms.4,5
Therefore, point of care ultrasound (PoCUS) has assumed an increasingly important role, namely in the acute abdomen, when there is no clinical consensus because it allows early recognition and diagnosis and consequently prompt initiation of interventions.5
Nevertheless, it is crucial that PoCUS practitioners have a structured, planned and validated learning process so that this tool can enhance patient observation and point-of-care ultrasound augmented clinical exam (PACE) can integrate routine physical examination.
We describe the case of a patient with an acute abdomen in which PACE, performed by an experienced professional, helped to diagnose appendicitis despite all other complementary exams being normal.
Case Report
A 21-year-old woman, without relevant past medical his-tory or chronic medication, presented to the ED with acute epigastric pain, which irradiated to the right iliac fossa over the week before. She had no nausea or history of vomiting.
Vital signs revealed a blood pressure of 142/73 mmHg, heart rate of 103 beats/min and oxygen saturation of 100% on room air. On physical examination, the patient presented a depressible abdomen with no palpable masses, and Blumberg, McBurney and Murphy’s signs were absent. However, she complained of progressive increasing epigastric pain with right iliac fossa irradiation and without relief factors. Blood samples (including blood count, C reactive protein, bilirubin, AST, ALT) with HCG dosing were collected, and vaginal ultrasonography was performed, all without detectable alterations.
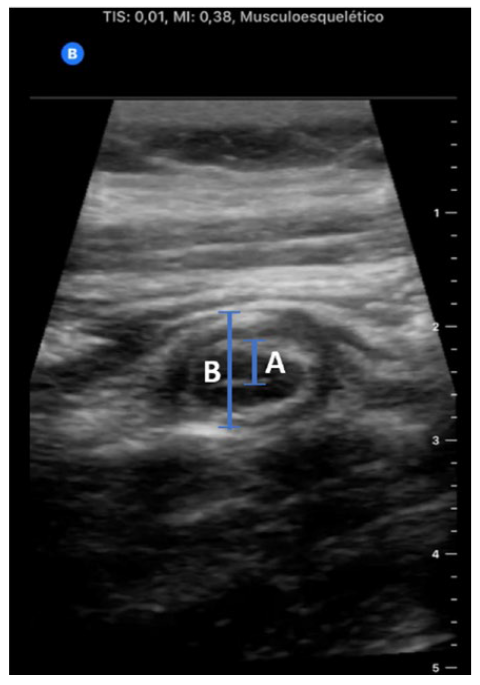
In this context, the patient was discharged home with paracetamol 1 g, three times a day, and dexketoprophen 20 mg, three times a day. However, one day later, the patient returned to the ED with abdominal pain intensification, though she maintained the same physical examination and laboratory exams. This time, an internal medicine doctor observed the patient, who performed PACE, which revealed an increased appendix diameter with noncompressible tubular structure and distorted irregular mucosa, suggestive of acute appendicitis (Fig. 1). She had no signs of ascites, nor hydronephrosis and her vaginal ultrasonography resulted without pathological alterations. Consequently, an abdominal ultrasound was performed by a radiologist, confirming the diagnosis of appendi-citis, and the patient had undergone surgery.
Discussion
Appendicitis is the most common surgical abdominal emergency worldwide, affecting 100 cases out of 10 000 inhabitants/year in Europe and the United States. It is caused by appendicular lumen obstruction, which leads to wall inflammation, ischemia, necrosis, and, if not treated, appendix perforation in almost 30% of the cases.1-3Therefore, early diagnosis and rapid surgical treatment are critically important to reduce morbidity and cost of care.2
However, the clinical diagnosis of acute appendicitis can be complex and confusing due to similar presentation and symptoms of several abdominal conditions, such as diverticulitis, acute Crohn’s disease, and infectious enterocolitis. In addition, acute genitourinary disorders, like pyelonephritis and ureterolithiasis, may also mimic symptoms and, in young women, acute gynecological diseases such as ovarian torsion, hemorrhagic ovarian cyst, pelvic inflammatory disease, and ectopic pregnancy must also be considered.2
The use of US in ED, performed both by radiologists and bedside clinicians, has become widespread, and consequently, it can be of great help in these cases.4 An acute appendicitis diagnosis is quite simple to be performed using ultrasonography since some easy direct signs allow its recognition: non-compressibility of the appendix, diameter > 6 mm, single wall thickness ≥ 3 mm, presence of the target sign (hypoechoic fluid-filled lumen, hyperechoic mucosa/submucosa and hypoechoic muscularis layer), the presence of an appendicolith and colour doppler and contrast-enhanced US showing hypervascularity of the wall in early stages (also called “ring of fire” edema).5 Nevertheless, considering time constraints and critical conditions of some ED patients, the US should be focused and specific to patient symptoms, as is done in the PACE approach.6
PACE is a targeted ultrasound investigation performed and interpreted by the physician at the bedside as part of the clinical examination, allowing early recognition, diagnosis and prompt interventions.6 In this context, the US is used to answer specific clinical questions and according to Al Ali, Jabbour and Alrajaby, the usefulness of applying this technique in a systematic method, using specific protocols, increases the sensitivity and specificity of physicians assessment, composing the fifth pillar of physical examination.1,6
With this in mind, a systematic PACE protocol must be established so that all bedside physicians use it in the same way and to ensure the correct use of this technique to be a safe and advantageous tool for patient care.
In the presented case, the protocol used was based on scanning the abdominal wall area where the patient reported more pain in search of the appendix. After this, the compressibility of the appendix was checked, and its walls and diameter were measured. According to this protocol, diagnosis can be made when a non-compressible appendix is detected with either a single wall thickness of 3 mm (or more) or an appendix diameter greater than 6 mm - all criteria were present in this case.

