











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
A 17-year-old male presented with a three-day history of vomiting and severe abdominal pain. One week before, he developed malaise, oligoarthritis, and a non-blanching maculo-papular, palpable purpuric rash over the lower limbs (Fig. 1). He was admitted to the department of Internal Medicine for treatment of severe abdominal pain, intolerance to oral intake and for diagnostic purposes. Intravenous hydration and symptomatic relief of arthralgia and colicky pain using nonsteroidal anti-inflammatory drugs was promptly initiated. Hemoglobin, leukocyte, and platelet levels were normal as were coagulation, kidney, and liver function tests. Cryoglobulins, ANAs, ANCAs, complement, and rheumatoid factor were negative. Serum IgA (443 mg/dL, reference <293) and C-reactive protein (8.2 mg/dL, refence <0.5) levels were increased. Urinalysis demonstrated mild hematuria and proteinuria. Search for infectious diseases was negative. An abdominal computed to-mography (CT) scan identified nonspecific lymphadenopathy and trace of free intraabdominal fluid.

Figure 1: Cutaneous involvement in IgAV. Palpable purpura was symmetrically distributed and located in the feet and distal tibial area. Histopathology analysis of purpuric lesions typically disclose leukocytoclastic vasculitis in postcapillary venules with IgA deposition.
Esophagogastroduodenoscopy revealed multiple superficial purpuric lesions in the duodenal and gastric mucosa (Fig. 2). Biopsy specimens showed lymphoplasmacytic infiltrate without vasculitis. Histopathology of a skin biopsy was consistent with IgA vasculitis (IgAV). High-dose prednisone (40 mg, 1 mg/kg per day) was started with complete resolution of symptoms. Prednisone taper with complete withdrawal was attained at eight weeks. Of interest, a control esophagogastroduodenoscopy, performed 12 months after the initial diagnosis, showed complete disappearance of petechiae lesions (Fig. 3).
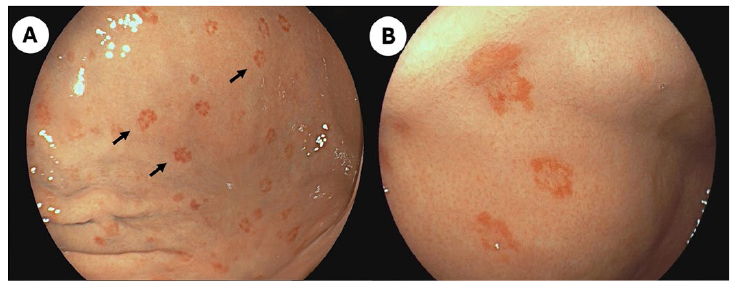
Figure 2: Gastrointestinal involvement in IgAV. Upper gastrointestinal endoscopy appearance of the stomach and descending portion of the duodenum disclosing multiple purpuric lesions (2-3 mm) and swelling of the superficial mucosa. Pathophysiology of abdominal pain and gastrointestinal lesions in IgAV involve vascular injury with resultant submucosal hemorrhage and edema. The descending duodenum, stomach, and colon are the most frequent locations of IgAV gastrointestinal involvement.
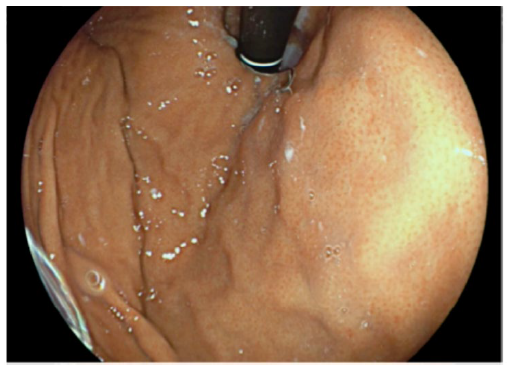
Figure 3: Control upper gastrointestinal endoscopy performed one year after the initial diagnosis showing complete resolution of the mucosal edema and purpuric lesions.
Although palpable purpura is identified in 75% of patients with IgAV, and gastrointestinal (GI) symptoms occur in 50%-85% of cases,1,2concurrent development of skin and GI purpuric lesions has been scarcely reported.3 Endoscopy findings in IgAV (typically involving the duodenum and the stomach) include purpura, hemorrhage, erosions, and ulcers.2,4,5Histology of upper GI tract usually demonstrates nonspecific lymphocyte infiltration. Vasculitis is rarely identified (<5%).2,4,5

