











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Malignant mesothelioma is a heterogeneous disease whose etiology, epidemiology, pathology, and management differ depending on the site of origin (pleura, peritoneum, pericardium, or tunica vaginalis testes).1 The peritoneum is the second serous membrane most affected, but it is still an uncommon entity.2 The epidemiological data vary across regions, with the United Kingdom, Australia, and New Zealand having the highest rates, while Japan and central European countries have the lowest rates.3 The estimated incidence of peritoneal mesothelioma (PM) in the United States is 800 cases per year.4 Compared to pleural mesothelioma, PM has an earlier median age of diagnosis (63 vs 71 years) and its correlation with asbestos exposure is weaker.5 Only 20%-40% of all PM had previous asbestos exposure.5 Duration and timing of exposure are not directly associated with disease progression.3 Although not well established, there are other risk factors: germline mutations (BRCA, CDKN2A, or NF2); genetic syndromes (BAP-1 tumour predisposition syndrome, Lynch syndrome, and Li-Fraumeni-like syndrome); autoimmune inflammatory processes; therapeutic irradiation; peritoneal irritation from previous surgeries; chronic peritonitis; Hodgkin’s disease; endometriosis; exposure to erionite, thorotrast or talcum; and presence of long-standing intra-abdominal catheters.4
PM symptoms are non-specific and may be asymptomatic, which delays the diagnosis. Symptoms include abdominal distension and pain, asthenia, weight loss, anorexia, nausea/ vomiting, early satiety, night sweats, constipation, and fever.6 At physical examination, patients may present with ascites, abdominal distention, or an abdominal mass. Due to its low frequency, PM is not the leading diagnosis hypothesis, and a diagnostic laparoscopy is often required. The diagnosis confirmation is histological, by assessment of multiple core biopsies.4
PM can be classified into three histologic subtypes (epithelial, sarcomatoid, and mixed), with the latter two having an unfavourable prognosis. Other factors listed as having a worse prognosis include nodal involvement, extraperitoneal metastasis, tumour mass of more than 5 cm in the epigastric region, and loss of normal architecture of the small bowel.4,5 CA-125 and CA15-3 tumour markers may be raised, however, there is no marker completely specific or sensitive.3,4,6Ascites cytology is not useful for diagnosis due to low sensitivity and cannot differentiate between benign and malignant mesothelioma.1 Laparoscopy is often recommended because it can assess resectability, the peritoneal cancer index (PCI) scoring system, and biopsy lesions at once.3 The classical TNM staging system is not appropriate for PM because nodal involvement and extraperitoneal metastasis are not frequent. Thus, the PCI scoring system is the staging system recommended to assess the extent of peritoneal disease burden.7 PCI score uses the mean size of the largest nodule and multiplies it by the regions with disease (minimum 1; maximum 39). The PCI scoring system is converted in T stages, PCI scores 1-10; 11-20; 21-30; >30 correspond to T 1; 2; 3; 4, respectively. Patients with T4M0 or M1 have a poor 5-year prognosis (29% survival).3,7
In this paper, the authors present an ascites diagnosis workup that leads to a PM. This case reflects the difficulty of the diagnosis.
Case Report
The authors present the case of a 45-year-old Romanian male, living for 17 years in a rural area of Portugal. The patient was a farmworker but had no contact with animals. There was a previous smoking consumption (7.5 pack year), but no other past medical history, alcohol or drug consumption, or asbestos exposure. The patient was admitted twice to the Internal Medicine ward for ascites investigation. The patient presented diffuse abdominal pain associated with abdominal distension, weight loss (10% in 3 months), and anorexia. Physical examination revealed cachexia, pale skin, abdominal distension with moderate ascites, and discomfort at palpation of the right flank and hypochondriac regions. Lymphadenopathies and skin alterations were not present. The broad investigation is described further, and laboratory results are listed below (Table 1).
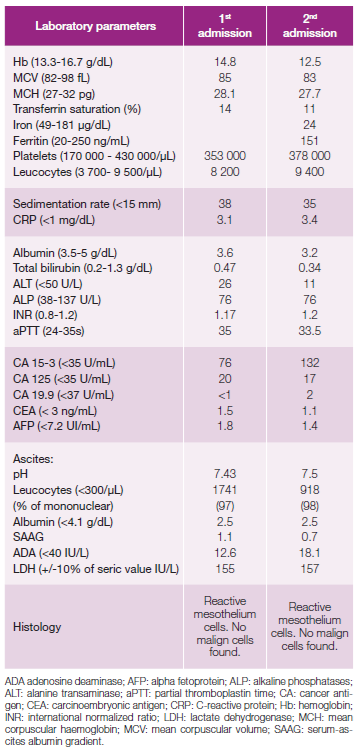
The patient had a normal hemogram, sedimentation rate of 38 mm, and CA 15-3 mildly elevated (76 U/mL). There was no hepatic injury and renal function tests were normal. Autoimmune (anti-liver/kidney microsomal, anti-mitochondrial, anti-nuclear, anti-smooth muscle, anti-dsDNA, anti-SSA/Ro antibodies) and zoonosis studies (Brucella spp, Leptospira spp, Bartonella spp, Borrelia spp, Coxiella spp, and Rickettsia spp) were negative. Human immunodeficiency virus, hepatitis virus, herpes simplex virus, parvovírus, and syphilis serologies were also negative. The patient had a positive IGRA test. First ascites analysis showed an inflammatory type of fluid, leucocyte count 1741/ µL with mononuclear cells predominance (97%). Bacterial and mycobacterium ascites cultures were negative. Adenosine deaminase (ADA) and mycobacterium PCR search were negative too. Histologic analysis revealed reactive mesothelial cells, without signs of malignant cells. Abdominal echography showed no liver structural alterations, and the abdominal, pelvic, and thoracic computed tomography (CT without contrast) only revealed ascites. Upper and lower digestive endoscopies were normal. Evacuation paracentesis was performed for patient relief without reaching a diagnostic conclusion and the patient was referred to consultation.
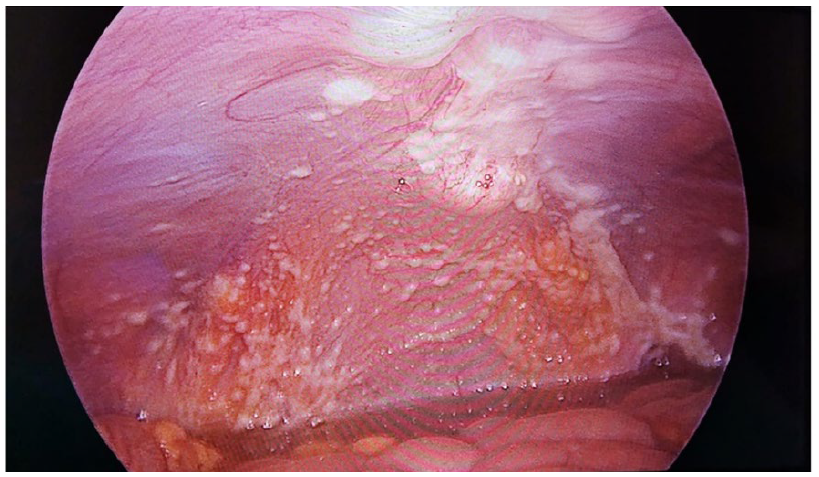
Two months after discharge, a second abdominal CT with contrast revealed nodular density of greater epiploon, adjacent to the right colon and sigmoid serosis, described as potential peritoneal carcinomatosis. The patient was re-admitted for an exploratory laparoscopy. In the meantime, the patient maintained symptoms and had reformed moderate ascites. This time, the patient presented chronic disease anaemia (Hb 12.5 g/dL), a normal leukogram, and CA 15-3 value increased. The second ascites analysis demonstrated a similar type of fluid, serum-ascites albumin gradient was 0.7, and ADA remained negative. Surgery revealed numerous nodular implants in the parietal peritoneum, falciform ligament, and great epiploon (Fig. 1). The biopsy of the epiploon nodules revealed a malignant epithelioid mesothelioma. The immunohistochemistry was positive for calretinin, Wilms tumour protein 1 (WT-1), podoplanin, cytokeratin 7 and KI-67: 10%. This condition corresponds to a T2N0M0 stage (PCI score 18). The multidisciplinary oncology team decided to start the nivolumab plus ipilimumab protocol.
Discussion
This case reflects the difficulty of this diagnosis. As previously reviewed, symptoms were non-specific, the ascites cytology was uninformative, and clinicians tended to exclude other frequent causes for ascites. In this case, the first CT was unhelpful. CT is usually enough to confirm the suspicion, nevertheless, it tends to undervalue the disease burden.3 In PM cases, CT can reveal abdominal masses (soft tissue heterogeneous and irregular mass), peritoneal effusion, mesenteric or parietal mesenteric nodules, peritoneal visceral thickening, and extra-abdominal metastasis.3 Magnetic resonance imaging is more accurate in assessing tumour progression and staging.3 It was the second CT that evidenced the two main diagnostic hypotheses: mesothelioma or peritoneal tuberculosis. The epiploon nodules led to a timely exploratory laparoscopy, which otherwise would have been delayed. Laparoscopy not only confirmed the diagnosis through biopsy but also allowed for proper staging. Initially, the authors suspected peritoneal tuberculosis since the patient was from a high-prevalence country and had a positive IGRA test. However, due to previous vaccination, low ADA levels on two measurements, negative mycobacterium cultures, and PCR, this diagnosis was presumed unlikely. For that reason, tuberculostatic agents were not started. The hypothesis of primary or secondary malignant disease persisted, although the first imaging and endoscopy exams did not reveal alterations. For that reason, a second CT was performed in the ambulatory.
The patient presents an epithelioid PM subtype, which is the most common (80% of the cases) and the least aggressive type.4 It is associated with more favourable outcomes. This subtype is characterized by frequent mild cellular atypia.4 Due to its rarity, there are few prospective trials and no evidence-based recommendations. Thus, clinicians usually extrapolate data from pleural mesothelioma. Treatment options include single chemotherapy or a combination of therapies, such as the combination of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy, systemic chemotherapy, peritoneal chemotherapy, immunotherapy, and targeted molecular therapy.3 The last two are not well established yet. However, nivolumab plus ipilimumab was started, extrapolating the European recommendations for pleural mesothelioma.8 Four months after initiating treatment, the patient maintains a performance status of 1, asthenia, and moderate ascites.
In conclusion, the authors highlight the diagnosis difficulty and alert other clinicians not to delay exploratory laparoscopy if there is a PM suspicion.

