











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
The increasing incidence of head and neck cancer has contributed to a significant increase in the number of people with a ventilation ostomy (Jakobsen et al., 2018). This growing number can be seen both in the hospital and in the community contexts. Thus, training the person to live with the ostomy is a fundamental and increasingly common area of intervention by nurses.
Acquiring competence in self-care is one of the biggest challenges posed to people with a ventilation ostomy (Queirós et al., 2021). The person and/or the family are expected to acquire skills to take care of the ostomy, its devices and potential complications when they return home (Spito & Cavaliere, 2019). Despite being complex and demanding, acquiring the skills required to take care of the ostomy is also described as a driver of a healthy transition as it improves acceptance of the stoma, quality of life and can also reduce associated health care costs by reducing the incidence of complications (Jansen et al., 2018).
The use of an instrument to assess self-care competence in people with ventilation ostomies allows data to be collected in a more organized and complete fashion, facilitating the identification of nursing care needs, as well as the nurse’s decision-making process regarding interventions to be implemented. In addition, it can contribute to improving information sharing between hospitals and community resources, as it standardizes and details the information related to the self-care competence of the ventilation ostomy.
In Portugal, there is no valid measurement instrument that allows the knowledge and self-care skills that a person with a ventilation ostomy must develop to be assessed.
Thus, the objective of this study is to evaluate the psychometric and clinimetric properties of the assessment form for the development of self-care competence in people with a ventilation ostomy previously developed by Queirós et al. (Queirós et al., 2015).
1. Literature review
A ventilation ostomy, also commonly known as tracheotomy or tracheostomy, consists of an opening or stoma created in the neck, with direct communication to the trachea, whose main objective is to allow entry and air out of the lungs (National Health Service [NHS] Southern Health, 2017).
Regardless of the clinical indication for a ventilation ostomy, or whether it is temporary or permanent, people with a recent ostomy experience a significant change in their health condition. The aesthetic and functional repercussions resulting from the surgery, possible adjuvant treatments (chemo or radiotherapy in the case of oncological disease) and the presence of the stoma can affect psychological, emotional, social aspects and even the person’s communication (Heutte et al., 2019). For this reason, the continuous monitoring and guidance of these people by a multidisciplinary team is considered crucial.
Nurses are professionals who “... provide specialized care with the objective of maximizing independence for self-care, and support people to adapt to the changes that arise due to the presence of the stoma” (Direção-Geral da Saúde, 2016, p. 20). The changes that occur with the presence of an ostomy require not only acceptance of the new condition, but also that the person acquires skills and competences to care for the ostomy and to use new materials and devices in the stoma. Therefore, promoting self-care is an essential area of intervention for people with a new ostomy and which is based on the autonomous intervention field of the nurse.
Self-care can be described as the ability of an individual, family, or community to promote health, prevent illness, maintain health, and cope with illness or disability (World Health Organization, 2019). Ostomy self-care is considered a decision-making process that influences actions related to maintaining the stoma and peristomal skin, identifying problems and complications and managing them (Villa et al., 2019). Thus, nurses are expected to implement nursing interventions that enable people to take care of their ostomy autonomously. To this end, a systematic assessment of self-care competence in clinical practice is highly recommended to identify care needs and to direct interventions to the specific needs of each person (Ausili et al., 2014).
In fact, health professionals increasingly feel the need to objectively measure the concepts they intend to assess. Measurement seems to be crucial, as it conveys the idea of unanimity, since different people in different places can assign an equivalent classification to a concept. Measuring instruments are the means by which the concept to be measured is determined. However, before being used, these instruments must be tested and properly validated, in order to ensure the quality of the results obtained (Souza et al. 2017).
Moreover, valid assessment instruments are essential to collect data on the ostomised person, to describe their competence in self-care and, if necessary, to identify educational or support interventions (Villa et al., 2019).
In 2015, Queirós et al. built an instrument entitled “Form for assessing self-care competence in people with a ventilation ostomy;” however, it has yet to be validated (Queirós et al., 2015).
Thus, the research question defined for this study was: What are the psychometric and clinimetric properties of the self-care competence assessment form in the person with a ventilation ostomy?
2. Methods
A quantitative, cross-sectional and methodological study was carried out with the aim of evaluating the psychometric and clinimetric properties of a measuring instrument.
Sample
The study sample consisted of people with a ventilation ostomy, or who were proposed to undergo the procedure, followed up in three hospitals in the north of Portugal. We chose to include people proposed to undergo the ostomy surgery because promoting self-care can be started even before the stoma is placed. The sampling method used was non-probabilistic for convenience. The sample size calculation was based on Bryman and Cramer (2003), corresponding to at least five times the number of items in the instrument to be validated. Since the instrument consists of 39 items, the sample consisted of a total of 195 participants. The inclusion criteria defined were: 18 years or older in age, having a temporary or permanent ventilation ostomy or waiting for it to be placed, and having the potential for self-care for the ventilation ostomy.
The sample of this study consisted mainly of males (92.8%), married (77.4%), with an average age of 63 years (minimum 24 years, maximum 85 years), with four years of schooling (71.8%) and retired (75.4%). Regarding their clinical condition, the majority (77.9%) had already undergone surgery more than a month prior (on average, 3 years and 10 months), knew the diagnosis that led to surgery (90.7%), the most prevalent being laryngeal carcinoma (80.5%), had a surgical ostomy (94.4%, the remaining 5 .6% were waiting for surgery), definitive (76.1%), resulting from a total laryngectomy (59%) and had not participated in a preoperative nursing consultation (59.5%). Furthermore, the sample mostly had some contact with people with a ventilation ostomy in the preoperative period (79%) and did not need support in self-care for the ventilation ostomy by an informal caregiver at home.
Data collection instrument
Data collection was performed only by this study’s main researcher in the different care contexts between April 2018 and May 2019.
The form consists of two parts, the first dedicated to the characterization of the participant, where there are sociodemographic variables, clinical and treatment variables. The objective of this first part is to define a profile of the person as well as their clinical and treatment context (Queirós et al., 2015). The second part refers to the assessment of self-care competence regarding the ventilation ostomy and consists of 39 items (outcome indicators) distributed over a set of six dimensions/domains, namely: Knowledge, Self-surveillance, Interpretation, Decision Making, Execution, and Negotiation and Use of Health Resources (Queirós et al., 2015). Each item has a Likert-type ordinal scale assigned a rating from 0 to 5, in which the higher the score, the greater the competence demonstrated, with the following ordering: 0 - “does not apply”, 1 - “does not demonstrate "; 2, 3 or 4 - “partially demonstrates”; 5 - “fully demonstrates”. As for the score between 2 and 4, its attribution varies according to the number of criteria demonstrated by the participant for each indicator of the competence domains, based on the help manual for completing the form created by the authors when it was constructed (Queirós et al., 2015).
Statistical analysis
The Statistical Package for Social Sciences (SPSS) software, version 22 for Windows, was used to analyse and process the data.
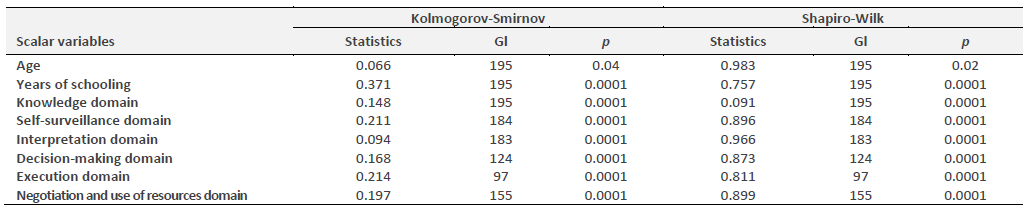
The normality of the distribution of the scalar variables was evaluated using the Kolmogorov-Smirnov and Shapiro-WilK normality test, as shown in table 1. All the variables were found to present a distribution that was not normal with p<0.05. Thus, nonparametric statistical tests of difference or association were used for the inferential statistical analysis.
To study fidelity, assessing the internal consistency of the items of the total scale and its domains, inter-judge fidelity and the two-half test. The averages of the responses of the observers by domain were also compared using the Wilcoxon test.
The test-retest was excluded from this assessment as it is related to the instrument’s temporal stability/reproducibility (Polit & Beck. 2016). As the concept to be measured relates to competence in self-care, it is not stable over time. Thus, it is expected that it will be in continuous change and development.
The study of validity consists of content, construct and criterion validity. Content validity was ensured in the focus group carried out with experts during the construction of the instrument (Queirós et al., 2015). It was not possible to assess criterion validity since there is as of yet no other valid instrument to assess the same or similar concepts. Construct validity was evaluated through factor analysis and inter-domain correlation since they are related to the confirmation of the dimensionality of the form and analysis of its theoretical structure.
A study of the relationships between some variables was also performed in order to understand whether the instrument was sensitive in its clinical application (Ribeiro. 2010).
Ethical considerations
This study complied with all the ethical assumptions inherent in the Helsinki protocol. During the planning phase, authorization was requested from the authors of the form as well as the health institutions selected to implement the study, which issued favourable opinions. During the data collection phase, informed consent was requested from the participants through a formal document where, after explaining the study, objectives and purpose, the person reflected and expressed their free and informed will to participate, or not, in this investigation.
3. Results
In assessing the instrument’s internal consistency, Cronbach’s Alpha was calculated for all the instrument’s items and its contribution to the general scale, that is, its value if it were excluded (Table 2).
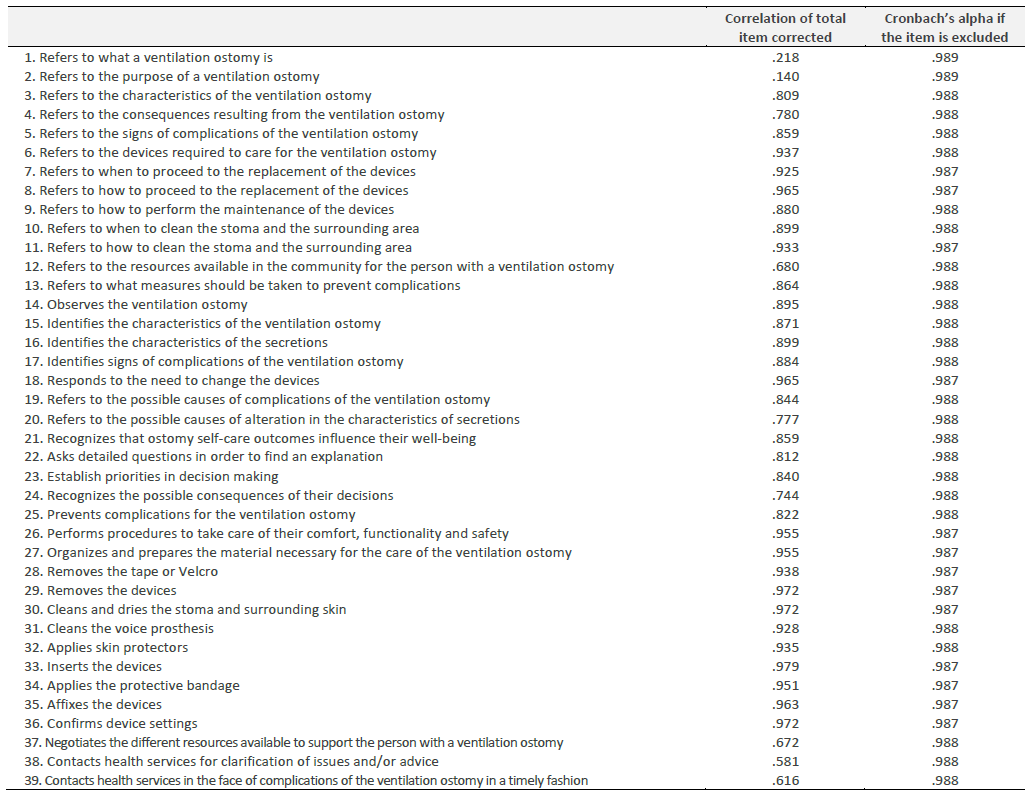
It was possible to verify that the values of the individual items are very adequate, with the exception of items 1 and 2 which had lower values. However, there was no item on the global scale whose exclusion had a significant impact on the Cronbach’s Alpha of the scale as a whole (equal to 0.98).
Since each domain assesses a different content of ostomy self-care competence, we also evaluated the internal consistency of the different domains of the scale. The results are shown in table 3.

The domains of self-surveillance, interpretation, decision-making and negotiation and use of health resources showed Cronbach’s Alpha between 0.90 and 0.95, corresponding to an excellent internal consistency for the instrument (Souza et al., 2017). The knowledge and execution domains showed Cronbach’s Alpha greater than 0.95.
During the data analysis process, there was a high number of “0 - not applicable” responses to item 31 (“cleans the voice prosthesis”) in the execution domain, as it is a specific procedure, which is only suitable for individuals who have undergone speech prosthesis placement, a characteristic that did not apply to a large part of the sample (69%). We therefore decided to exclude this item from the remaining assessments, so that it would not compromise the responses given by individuals to the other items in the execution domain. However, in order to understand whether its exclusion would have an impact on the instrument’s internal consistency, the Cronbach’s Alpha value for the execution domain excluding this item was assessed, and the result was 0.99. That is, its removal did not cause changes in the internal consistency despite the fact that this result indicated redundancy of the items in this domain.
The remaining items for which the score was “0 - not applicable” were treated as missing values.
With regard to inter-judge fidelity, a comparison was made between the data obtained by observer A versus those of observer B, who applied the form at the same time, to the same subjects, but having assigned scores to the items independently. The results are described in table 4.
Table 4 Assessment of concordance between assessors using the Spearman correlation coefficient (rs)
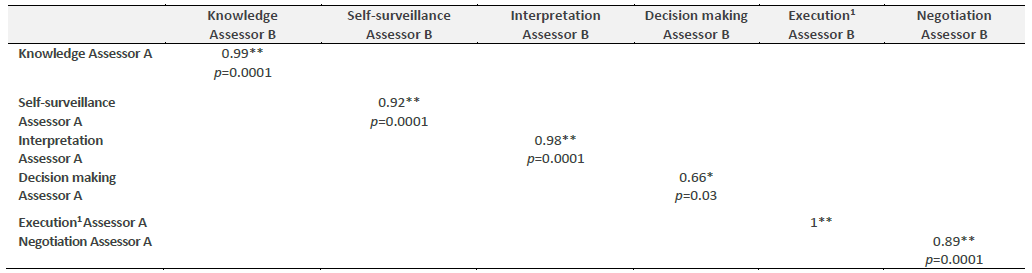
*Correlation is significant at 0.05/ **Correlation is significant at 0.01/ 1 - Excluding item 31 - “Cleans the voice prosthesis”
A very high correlation between the results obtained by the different evaluators was found, and the domains of knowledge, self-surveillance, and interpretation obtained a value of rs above 0. 90 and with a significance level of p < 0.001, which meant the results were statistically significant. The dimension negotiation and use of health resources also showed a high correlation. Execution was the only domain that obtained the value rs equal to 1, which indicates a perfect correlation, with total concordance between the two observers. The decision-making dimension obtained an rs of 0.66, which reflects a moderate correlation (Pestana & Gageiro. 2014).
The Wilcoxon Test was also performed to complete the study of reliability between assessors. This test compares the means obtained between the two assessors in each domain of the scale, as shown in table 5.

The results indicated that there only were significant differences between the means of the two observers’ assessments in the domain of interpretation.
To perform the two-half test, responses to the even-numbered items were separated from responses to the odd-numbered items, creating an even variable and an odd variable for each domain. Once these new variables were created, the correlation coefficient of the Spearman correlation between the variables was calculated. The results are described in table 6.
Table 6 The two-half test using the Spearman correlation coefficient (rs)
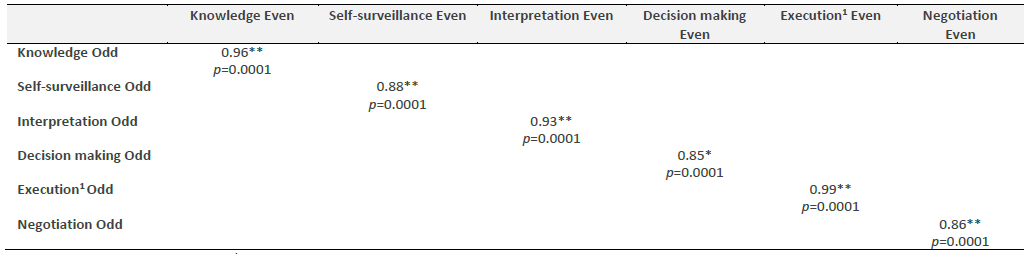
** Correlation is significant at 0.01/ 1 - Excluding item 31 - “Cleans the voice prosthesis”
From analysis of the table, the following was obtained: very high correlations in the domains of knowledge (rs=0.96; p<0.001), interpretation (rs=0.93; p<0.001) and execution (rs=0.99; p<0.001) and high correlations for self-surveillance (rs=0.88; p<0.001), decision making (rs=0.85; p<0.001) and negotiation of health resources (rs=0.86; p<0.001) (Pestana & Gageiro. 2014).
Factor analysis was chosen to study construct validity, in order to confirm the possible dimensionality of the instrument. First, exploratory factor analysis was performed using the principal components analysis method without forcing the number of factors. Four components/factors were extracted, which did not fit the theoretical structure that presided over the construction of the instrument, nor did it reveal theoretical coherence. Then, a new attempt was made, using the Varimax Rotation method with Kaiser normalization, forcing the number of factors to six with the intention of grouping the items into the form’s six domains. Although the result demonstrates more coherence than the first attempt, a structure with acceptable theoretical coherence was not obtained, nor compatible with the theoretical construct of the form.
Inter-domain correlations were also studied to understand whether the construct we are evaluating, despite being composed of different dimensions, is part of a coherent whole that we intend to evaluate, which in this case is competence in self-care. The results are described in table 7.
Table 7 Correlation between the domains of the form
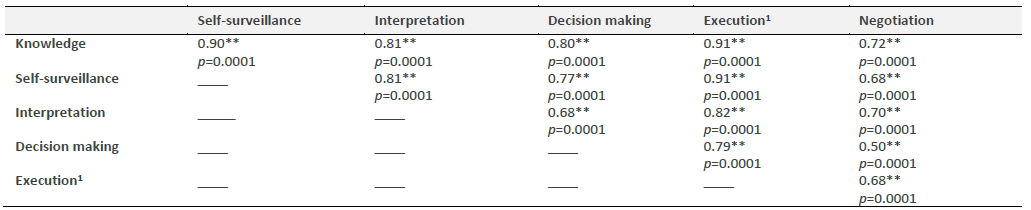
**Correlation is significant at 0.01/ 1 - Excluding item 31 - “Cleans the voice prosthesis”
It was possible to notice the existence of a positive correlation among all of the domains, demonstrating moderate, high or very high associations, all of which were statistically significant. This fact seems to reveal that all domains are related to each other, although they measure different components of the same construct.
The domain of knowledge showed the highest correlations with the remaining domains of the form, with the strongest correlation between the domain of knowledge and the domain of execution (rs=0.91; p< 0.001).
In order to assess whether the instrument was sensitive in its clinical application, we decided to test the relationship established between the domains of ostomy self-care competence and the clinical and the participants’ sociodemographic variables. According to the literature, individuals who have an informal care provider are expected to demonstrate less competence in ostomy self-care than those who do not (Mota et al., 2016). When performing the Mann-Whitney test between the two groups (with and without an informal care provider), statistically significant differences were obtained regarding the level of competence in self-care for the ventilation ostomy, in all domains (p<0.001). Individuals who did not have an informal care provider showed a higher level of competence in self-care for the ventilation ostomy as described in the literature.
The second proposition under study was regarding the existence of a relationship between the development of self-care competence in the ventilation ostomy and its duration (temporary vs definitive). According to the literature, individuals with a temporary ostomy are expected to have less competence in self-care when compared to individuals with a permanent ostomy (Taylor & Morgan. 2011). When performing the Mann-Whitney test between the two groups, statistically significant differences were obtained in all domains (p<0.05). The self-care competence demonstrated was higher in people with a permanent ostomy than in people with a temporary ventilation ostomy, which also seems to be in line with what is described in the literature.
4. Discussion
With regard to fidelity, a Cronbach’s Alpha between 0.90 and 0.95 was obtained in the domains of self-surveillance, interpretation, decision-making and negotiation and use of health resources, which corresponds to an excellent internal consistency. According to Tavakol and Dennick (2011), there are different opinions about acceptable values for Cronbach’s Alpha, usually ranging between 0.70 and 0.95. However, in the domains of knowledge and execution, the values obtained were higher than 0.95, which may suggest that some items are redundant according to these authors, as they test the same topic/subject, but in a different way. In this study, Cronbach’s Alpha was not analysed for each of the items on the form; however, it would be important to do so in these two domains, to see if they measure similar concepts. Thus, further studies are needed to explore the possible redundancy versus clinical relevance/utility of each of the items that make up the domains of knowledge and execution.
As for inter-judge fidelity, when comparing the data obtained by two different assessors, very high positive correlations were found, which translates into high agreement. The domain of execution obtained an rs value equal to 1, which corresponds to a perfect correlation. There is, therefore, total agreement between the two assessors. The decision-making dimension was the only one that obtained a moderate positive correlation, with an rs value of 0.66, but with statistical significance. The existence of a perfect correlation for execution is possibly due to the objective nature of the items that constitute it, which are easy to classify, and hence the equal results obtained. However, the same was not observed in the decision-making process, in which the dissimilarities observed were greater, despite the values being acceptable and equally significant. In turn, with the Wilcoxon test, it was only possible to perceive statistically significant differences between the two assessors in the domain of interpretation. The fact that the decision-making and interpretation domains present more subjective questions and with a possible greater complexity in the participant’s response may be the basis for their difficult measurement and justify the results obtained.
The two-half test was performed to complete the analysis of the instrument’s fidelity. The results were very positive, and in the domains of knowledge, interpretation and execution, very high and highly significant positive correlations were observed (p<0.001). In the remaining domains, the rs value was equal to or greater than 0.85, which revealed high and, once again, significant positive correlations.
As for the validity of the instrument, only the study of construct validity was performed through factor analysis and the determination of inter-domain correlations. Exploratory factor analysis was used in order to analyse the dimensionality and structure of the instrument. However, in the two attempts made, it was not possible to reorganize the factors according to a coherent theoretical structure. This constituted the main limitation of this study. Thus, further complementary studies should be carried out, namely using confirmatory factor analysis, to understand the construct validity of the instrument. With regard to the inter-domain correlation, the existence of positive and statistically significant correlations between all the domains of the form was found, although they evaluate different components of the same theoretical construct. The knowledge domain showed the highest correlations with the remaining domains of the form. In fact, all the domains are dependent on knowledge, as it is not possible for the individual to have the competence to monitor, interpret, make decisions, execute and negotiate if he has not developed and consolidated theoretical knowledge to do so.
With regard to the analysis of the instrument’s clinical sensitivity, when comparing the relationship obtained between the various domains of the instrument and the secondary variables with the available scientific evidence, there seemed to be consonance. That is, the results are in line with what is described in literature. Regarding the presence of a family caregiver and the duration of the ventilation ostomy, compatible and encouraging results were obtained.
Although some of the results presented in this preliminary study are promising, further studies are needed to assess the reliability and validity of this form. When there are instruments that measure the same or similar concepts, as well as opposing concepts, the criterion validity must be evaluated. The construct validity should also be analysed in subsequent studies. The construct validation process is considered one of the most demanding, in most cases requiring diversified studies in order to find and establish the covariance between the variables related to the construct (Bem et al., 2011). On the other hand, it would still be essential to analyse the specificity of the instrument. Finally, it would be important to validate the form in a representative sample of the country not restricted to the northern region, as was the case in this study.
Conclusion
The presence of a ventilation ostomy poses challenges to the individual, the family and health professionals, each of whom plays an important role in training for a life with an ostomy. Cohesion and mutual assistance are essential.
These challenges can be facilitated with the existence of theoretically sound and clinically relevant instruments for assessing self-care competence, which will allow nurses to guide the provision of health care in a more complete, rigorous and adjusted way.
The instrument for assessing self-care competence in the ventilation ostomy showed a high degree of fidelity with excellent internal consistency values in four of its six domains and very strong positive correlations, both in inter-assessor agreement and in the two-half test. It was also shown to be sensitive to the expected differences between the variables, indicating a good ability to assess the clinical reality. However, there is a need to carry out more studies to confirm its validity and reliability, which will give the preliminary results presented here more credence.

