











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Fever, although it is a very common manifestation during childhood and which, in most cases, proceeds without serious associated complications, continues to be one of the main reasons for seeking health services in the pediatric age.
At the preschool stage, the child's immune system is still developing. It is at this time that they begin to come into contact with viruses, ending up developing symptoms during this process. At this stage, the spread of viruses is facilitated by close contact between children in an environment that is usually closed and poorly ventilated (Blumenthal, 1998; NICE, 2019).
As a child's physiological defense mechanism, fever is still a concept wrongly known by most parents. Consequently, they adopt very intervening and/or inappropriate attitudes that are nothing more than a manifestation of insecurities and fears based on a lack of knowledge on this subject (Blumenthal, 1998; DGS, 2018; NICE, 2019). In most children, fever is diagnosed alongside self-limited infections and does not require short-term treatment. However, the felt need for multiple consultations within the same episode of illness is common, especially when fever persists.
Parenthood appears as a normative change within the family, associated with the performance of functions such as protection, education, and integration into family culture (Alarcão, 2002). Parental skills correspond to the set of knowledge and skills of mothers and/or fathers that allow them to perform, with mastery, the parental role and guarantee the maximum growth and development potential of the child (Cardoso, 2014).
On the other hand, from an integrative perspective of the various levels of care, systemic models emerge with great credibility and consensus. On the one hand, they consider multifactoriality, and on the other, they call for multidisciplinary convergence among health professionals (Figueiredo & Amendoeira, 2019). Betty Neuman (1995) focuses on the family's reaction to the factors involved in adapting the system. The intervention should be based on the identification, understanding, and classification of the stressors that influence the management of fever and on the resources available in the community environment or in the family itself that can enhance health gains.
The ecological model of the determinants of parenting (Belsky, 2006) suggests the interrelationship of parental behavior with different factors: personality and psychological resources of the parents, characteristics of the child, and sources of stress and support from the social context in which the parenting relationship -child is inserted. There are multiple factors determining parental behavior, including individual, historical, and social characteristics that are combined and appear to influence parental functioning (Luster & Okagaki,2005).
However, in this model it is not the child's characteristics, per se, that directly influence the parenting process, but rather the compatibility between the characteristics of the child and the caregivers (Belsky & Jaffee, 2006). To properly understand these factors, a biopsychosocial approach will be essential, considering genetic, cognitive or environmental factors (Belsky & Jaffee, 2006), placing greater emphasis on factors external to the family in the socialization process of individuals, such as the peer group and neighborhood.
This model is dynamic and moderating, allowing observation of protection systems against threats to the parenting process (Belsky & Jaffee, 2006). Therefore, optimal parenting is defined as a dynamic state that may vary in degree between the three determinants and depending on what allows a better quality of care for the child at a given time (Belsky & Jaffee, 2006).
Regarding their influence on the parenting process, the determinants do not have the same weight, the author believes that the most important thing will be the parental characteristics and that high parental functioning will continue to occur even if two of the three determinants are at risk, as long as the parental personal and psychological resources remain unchanged (Belsky & Jaffee, 2006).
In a critical assessment of Belsky's model, attention is drawn to the importance of the social context in which the family operates (extra-family factors), such as the risks and resources of the community, the quality of the neighborhood, poverty, cultural and ethnic customs and not just the broad social support that Belsky initially refers to (Barroso & Machado, 2010).
The Integrated Care Process for Short-Term Fever in Pediatric Age was designed in 2018 by the DGS and is applied in an integrated manner at different levels of care, with each institution being responsible for building strategies for its implementation. Continuity of care and coordination are recognized as essential elements to ensure that the child receives the best health care, timely and effective, and based on evidence and scientific consensus (DGS, 2018).
The N.I.C.E (National Institute for Health and Care Excellence, 2021) guidelines in the United Kingdom suggest a need to study parental perception as well as practices in fever management, particularly in outpatient therapeutic management regarding the assessment and management of febrile illness in children under the age of five.
Since the introduction of the term “fever phobia” 30 years ago, there have been few studies of changes in parental knowledge. Known factors that contribute to the demand for health services are parents' lack of knowledge, anxiety about fever, and the experience of inconsistencies in the approach of different health professionals (Blumenthal, 1998). This can lead to uncertainty, frustration, and dissatisfaction with care, as well as incorrect conceptions in this regard.
Several international studies reveal that parents adopt varied and incorrect attitudes when measuring and treating their children's fever (Pestana, 2003; Gomide, 2014). Parents' beliefs and knowledge about fever influence their behavior towards feverish children and, consequently, the use of antipyretics. Parents' conceptions about fever in children are often associated with prejudices transmitted by tradition, which are often mystified (Casanova et al., 2014).
These factors, in combination with a high rate of consultations and re-evaluations, increase healthcare costs and unnecessary use of antibiotics (DGS, 2018; NICE, 2019). Fever in children produces emotional, physical, and socioeconomic effects on parents, leading them to be absent from work, seek medical advice, and spend on medication (Gomide, 2014).
The majority of studies carried out in the literature take place almost exclusively in hospitals, some of which are in the context of serious illness. However, parents' knowledge and fear can be strongly influenced by the stressful situation inherent to their child's acute illness (Gomide, 2014).
Taking into account that the main role of primary health care involves health education and prevention attitudes, it is in this context that greater emphasis should be placed on training parents. The development of good clinical practices in the assessment and monitoring of fever in children must be promoted and ensured, in order to enable parents to self-manage fever and reduce the excessive number of inappropriate attacks (Casanova et al., 2014).
Thus, the carrying out of this research arose within the scope of the perception of clinical practice of inadequate recourse due to isolated fever to consultations for acute illness in primary health care and aims to support the empirical study towards improving the quality of care. Having as a population the parents of children of pre-school age, the objective was to systematize which factors determine (concept) parental knowledge and practices in the context of a fever through the identification of studies that contribute with evidence that supports practices appropriately.
1. Methods
Scoping Review (ScR) can clarify key concepts/definitions in the literature and identify key characteristics or factors related to a concept, including those related to methodological research. Using the Joanna Briggs Institute (JBI) method, the PCC question (population, concept, context) was defined: “What factors determine parental knowledge and practices in preschool children regarding fever management?” After defining the question, the research process began, with the keywords previously selected as MesH Browser 2024 descriptors, validated in each scientific database to be used in order to scientifically assess the terms: Parents/ Family/ Child, preschool / Child/ Fever/ Primary health Care/ General practitioners/ Physicians, family/ Family nursing.
After validating the terms, scientific articles were selected from the 20th to the 28th of July 2024, in the CINAHL Plus with Full-Text database (through the EBSCOhost computer platform available on the Ordem dos Enfermeiros website), in PubMed, Cochrane, Lillacs and Scielo, with articles published in full text between 2014-2024 being selected.
From crossing the various descriptors, 413 articles were obtained, with the respective titles and abstracts being read by the 3 reviewers/authors using the digital resource the Rayan platform, on which the screening was carried out according to the following protocol (figure 1). All articles whose approach to fever was associated with acute illness/emergency context/antibiotic therapy, which focused on the use of thermometers or equipment, or which fell outside the target group were excluded: children outside the age range 2-6 years.
After this methodological path, the 29 unreadable articles were read in full according to the defined criteria.
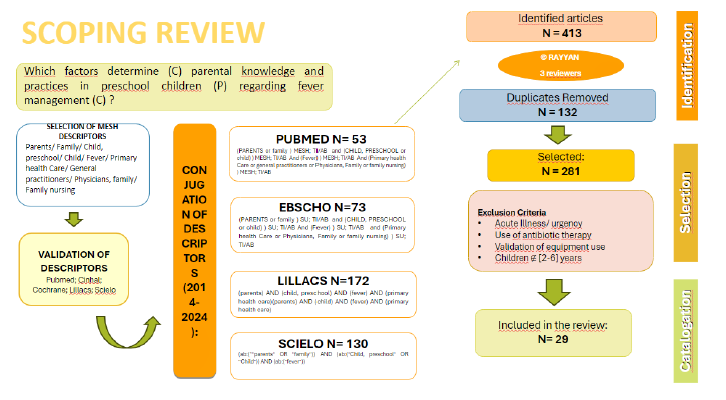
Figure 1 Research Protocol (july, 2024). Adapted from: Prisma Flow Diagram, Joanna Briggs Institute (2015).
2. Results
In order to facilitate understanding and discussion of the results, the studies were divided by types of determinants: Internal factors, which include articles that mention parents' knowledge and expectations in managing fever, and external factors that allude to the importance /intervention of health professionals in compliance with standards, as shown in the following table:
Table 1 Cataloging results by determinants. Adapted from: Melnyk, B.M. & Fineout-Overholt, E. (2015)
| 29 ARTICLES | |
|---|---|
| 13 Quantitative Studies 11 Qualitative Studies 1 Mixed Studies 1 Opinion Article 1 Scoping Review 2 Community Intervention Programs | |
| INTERNAL FACTORS: Parent/ Child Characteristics | EXTERNAL FACTORS: Environment, Family/Sociocultural network and health care |
| Fear, Anxiety contribute to ineffective fever management and arise due to gaps in knowledge and self-management of fever. Parents need to be safe and seek physical examination and information (Afonso et al., 2018; Kuijpers et al., 2021; Pitoli et al., 2020; Akbayram et al., 2021; Rivera-Fernández-Galán et al., 2022; de bont et al., 2015; Elkon-Tamir et al., 2017). | Family and social network, internet, professionals and health resources (Morris et al., 2021). |
| Previous experience; level of education; qualifications in the health sector; age; level of health literacy influence fever management (Choi & Kim, 2014; Kelly et al., 2017; Villarejo-Rodríguez & Rodríguez-Martín,2019; Edwards, Bolling-Walker & Deupree, 2020). | Importance of Community Pharmacies, friends and media (Urbane et al., 2019; Rivera-Fernández-Galán,2022; Kelly et al., 2017; Al arifi & Alwhaibi, 2021) |
| Predisposing, facilitating and need factors influence parents' decisions (Burokienė et al., 2017) | Access to healthcare (Cakpo et al., 2024; Chapron et al., 2018). |
| Academic level and beliefs influence measures to reduce fever and knowledge of warning signs (Pérez & Bartolomé, 2016). | More simulations and Education Programs with parents (Rivera-Fernández-Galán et al., 2022; Alqudah et al., 2014; Chefdeville & Pages, 2019; Lynch et al., 2024; Tavan et al., 2022) |
| Search for hospital care (greater security and confidence) in acute illness (Pitoli et al., 2020; Urbane et al., 2019). | Creating a relationship of trust and greater security for healthcare professionals (Westin et al., 2024) |
| Recognition of intuition and parental bonding as a source of information for health professionals (Van de Maat et al., 2018). | Lack of Detailed Approach in PHC to fever management - in IS consultations, anticipatory care and parenting preparation courses (Silva et al., 2020). |
| Teleconsultations and Information Leaflets (Chefdeville & Pages, 2019). | |
| Excessive professional work and health fatigue increase the number of prescription errors (de Bont et al., 2015). | |
| Lack of dissemination of recommendations/standards among health professionals (de Bont et al., 2015; Raffaeli et al., 2016). | |
| Failures in the Standardization of Criteria by Health Professionals - Action Protocols (Silva et al., 2020). | |
3. Discussion
Parents' conception of fever has a historical dimension. In the 16th and 17th centuries, the idea prevailed that fever represented a reaction of the body to help the body separate and eliminate harmful substances and was also a sign of the presence of the invasion of foreign agents into the body (Urbane et al., 2019 ). The belief that fever can cause brain damage and death is more recent (Choi & Kim, 2014). Parents' heightened fear of a child with a fever gives rise to concerns that, associated with their conceptions, often result in incorrect treatment practices and feelings of insecurity in the face of a feverish child (Kuijpers et al., 2021; Pitoli et al. , 2020).
The signs most valued by parents as indicators of fever are the child's general condition (behavior), which is as or more important than the measured value, and the physical consequences (Kuijpers et al., 2021; Pitoli et al., 2020 ). In some studies, for about half of parents, fever indicates serious illness, and 92.8% believe it is potentially fatal to the child's life (Choi & Kim, 2014; Urbane et al., 2019).
Walsh & Edwards (2006) and Walsh et al. (2008) consider parents' knowledge to be very weak regarding the temperature considered normal and considered fever. Younger parents and those with a higher socioeconomic status can accurately read the mercury thermometer (Choi & Kim, 2014; Urbane et al., 2019; Walsh & Edwards, 2006; Walsh et al., 2008). Parents seek advice from doctors and other health professionals when their children's temperatures do not reduce to the level they consider satisfactory despite the doses of medication administered (Walsh & Edwards, 2006; Walsh et al., 2008). And, they resort to the Emergency Department when they experience low temperatures (Walsh & Edwards, 2006; Walsh et al., 2008).
According to Walsh & Edwards (2006) and Walsh et al. (2008), parental concern about convulsions, dehydration, and physical discomfort associated with fever has increased. The authors concluded that the majority of parents reveal poor knowledge and phobia of fever, excessively administering antipyretics (ibuprofen and paracetamol) to reduce it and at relatively low temperatures.
In Portugal, a study carried out by Rodrigues et al. (2010) demonstrated that, in 62.8% of cases, a subjective temperature assessment occurred. The fact that they found that there is still a need for treatment for relatively low-temperature values (<38ºC), disproportionate monitoring, and disproportionate use of treatment with interspersed antipyretics, leads the authors to state that there is a need to raise awareness among parents about the benefits of fever in an infectious context (Rodrigues et al., 2010). They state that the training of parents and health professionals must be based on the rational use of medication, guided not by the temperature value but by the discomfort related to fever, prioritizing monotherapy schemes (Rodrigues et al., 2010) .
According to NICE (2019) guidelines, the priority is to maintain the child's hydration and recognize the signs of dehydration/warning signs. The antipyretic is effective if it lowers the temperature by 1º to 1.5º after 2-3 hours (DGS, 2018). In this context, some authors confirm that lack of knowledge leads to inappropriate use of antipyretics and premature seeking of healthcare (56.7% of parents) (Urbane et al., 2019). There is greater reluctance to use suppositories (Kelly et al., 2017), and using physical means as the first option is preferred by health professional parents (Villarejo-Rodríguez & Rodríguez-Martín, 2019). Antipyretics are also quickly administered in case of fever for fear of complications, but the interval between doses is very variable (Rivera-Fernández-Galán et al., 2022).
The use of antibiotics is common, but healthcare professional parents are reluctant to do so (Villarejo-Rodríguez & Rodríguez-Martín, 2019). There is also a tendency for non-health professional parents who live in rural areas to resort to the use of natural/alternative therapies, but these are rejected by health professional parents (Villarejo-Rodríguez & Rodríguez-Martín, 2019).
Given the results of the evidence obtained, the main intrapersonal factors that interfere in fever management emerge as the child's age, previous experience, and the parents' health training. Interpersonal support from the family environment and shared responsibility by parents and mothers' work outside the home (Choi & Kim, 2014; Kelly et al., 2017; Villarejo-Rodríguez, 2019; Edwards et al., 2020). In the study by Rodrigues et al. (2010), parents with less education (≤ 9th grade) administered antipyretics inappropriately at relatively low temperatures (<37.5ºC). Parents with older children (≥ 5 years), without higher qualifications and non-health professionals are less qualified to manage fever (Raffaele et al., 2016).
There are also predisposing, facilitating, and necessity factors that influence parents' decisions (Burokienė et al., 2017), and academic level and beliefs also influence measures to reduce fever and knowledge of warning signs (Pérez Polo & Bartolomé Ferrero,2016).
Most previous literature describes this issue in the context of hospital care. However, it is in the context of primary health care that greater emphasis should be placed on empowering parents: around 60.1% of parents turn to Primary Health Care first (Urbane et al., 2019). Still, for 68.2%, the hospital environment is seen as safer, more reassuring (Pitoli et al., 2020; Urbane et al., 2019), and suitable due to the inherent technology and, in rare cases, due to greater accessibility and proximity (Pitoli et al., 2020).
Thus, health professionals, as an external determinant, play a role in empowering parents to promote adequate fever management. Health promotion strategies aim to reinforce families' lines of defense (Neuman, 1995), and the DGS (2018) emphasizes the importance of adequate child supervision and coordination between different levels of care. Professionals and access to healthcare emerge as relevant factors in the studies found (Morris et al., 2021; Cakpo et al., 2024; Chapron et al., 2018). However, overwork and fatigue among healthcare professionals increase the number of prescription errors (de Bont et al., 2015).
The ecological model highlights the importance of the community in parental behavior and child behavior, as well as in parenting performance (Belsky & Jaffee, 2006). The most recent update of the Belsky Model takes into account all the social and community aspects mentioned above and the ecological model of parenting (Belsky & Jaffee, 2006), as described by Luster and Okagaki (2005), adds the contextualization of beliefs and cultural heritages in parental behaviors. Parents have a vast network of interpersonal relationships, which include not only a family nucleus but also a social nucleus (Rivera-Fernández-Galán et al., 2022; Al Arifi & Alwhaibi, 2021). Taking the external environment into account, parents turn to families and friends, community pharmacies, and the media/information leaflets when they want information about fever (Urbane et al., 2019; Rivera-Fernández-Galán et al., 2022; Kelly et al., 2017; Al Arifi & Alwhaibi, 2021).
The parents' first choice in case of doubt would be the family and then the family doctor (Kelly et al., 2017). For parents, there is a need for more accessible and consistent information in this area, simple and clear to reduce anxiety and worry in this process (Kelly et al., 2017).
Wrong practices, such as waking children at night or using antipyretics alternately to lower temperatures, are more frequent in parents with insufficient information about fever management, making them more anxious (Akbayram, 2021; Rivera-Fernández-Galán et al., 2022 ). As the main information to pass on, they suggest helping parents understand the etiology of fever, raising awareness of the benefits of fever in an infectious context, and informing them about the correct administration of antipyretics (Afonso et al., 2018). NICE (2019) presents the context of teleconsultation as a useful tool to help parents identify warning signs and screen for serious illness.
Thus, there is a need to improve the dissemination of recommendations among parents in order to avoid common therapeutic errors and unnecessary overload in emergencies through strategies such as the creation of written materials, face-to-face and online education sessions, and educational websites (Urbane et al., 2019; Raffaeli et al., 2016) as well as optimizing the dissemination of guidelines among health professionals (Raffaeli et al., 2016). The recognition of intuition and parental bonding as a source of information for health professionals is particularly important (van de Maat et al., 2018) to create a relationship of trust and greater security among health professionals (Westin et al., 2024).
The evidence found corroborates that Health Professionals play a preponderant role in adapting to the Parenting process, making it necessary to build a partnership with parents in order to provide them with knowledge and parental skills to manage the health/illness processes of their children effectively. children. In this context, family teams play a fundamental and privileged role in:
Understand parental knowledge and practices regarding fever in children,
Train parents to understand the etiology of fever and warning signs, raise awareness of its benignity, and provide information about its control, helping to reduce anxiety and improve fever management in children.
In this sense, many authors warn that educational programs with parents and constructive procedures should be implemented in services, which favor forms of appropriate use of various assessment devices, non-pharmacological interventions and disseminate information on the appropriate use of antipyretics and antibiotics (Rivera- Fernández-Galán et al., 2022; Alqudah et al., 2014; Other authors also mention the development of action protocols, standardizing criteria across units (Silva et al., 2020). Other authors add the importance of a detailed approach in CSP to fever management in child health consultations (as part of anticipatory care) and in Parenting Preparation Courses (Afonso et al., 2018). In this way, it will be possible to improve parental practices in caring for children with fever and consequently an adequate demand for services. It is possible to establish a schematic representation between the determinants of parenting found in this research and strategies to be implemented in clinical practice within the scope of fever management in preschool children (Figure 2).
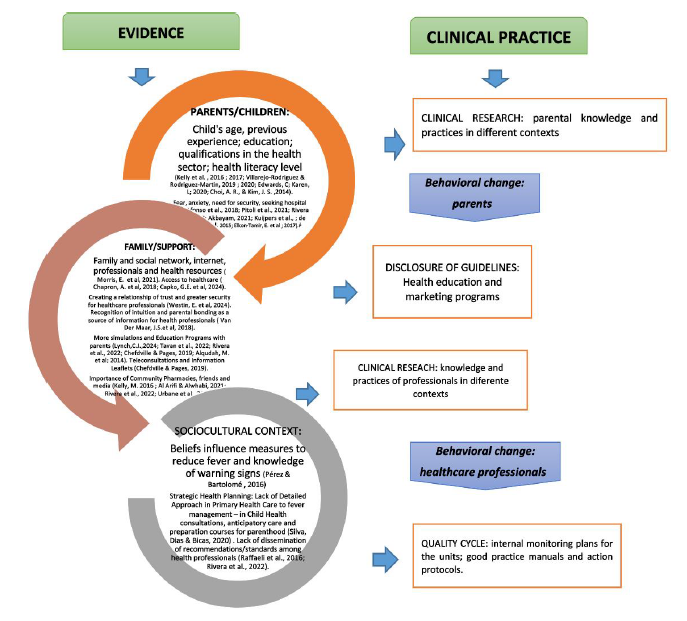
Figure 2 Determinants of parenting in fever management and clinical practice. Model of determinants of parenting adapted from Kotchich and Forehand (2002) and Luster and Okagadi (2005).
This Scoping Review may present some limitations in relation to the diversity of available evidence since the coverage of a larger number of databases could have provided other important contributions to the analysis of the results.
The reduced understanding of fever by parents determines the need for more research to identify what they understand about the topic and how they deal with the associated anxiety and fear. On the other hand, it is also important to understand the perceptions and procedures of healthcare professionals in this area. In this context, the reduced amount of evidence found was also a factor in the analysis, which suggests investment in studies focusing on PHC health professionals (especially nurses) and the practices established, as they are the most supportive resource. and proximity. We also add the possibility of conducting experimental studies with groups of nurses from different contexts to evaluate the strategies used to promote effective management of fever in children.
Conclusion
In professional practice, we can see a lot of divergence in knowledge and parental interventions when dealing with children with fever.
In the digital society we live in, it is essential to publicize appropriate practices among families, promote responsibility, autonomy, and trust, and avoid the adoption of wrong therapeutic attitudes and inadequate use of health services. At the same time, efforts should be made to strengthen the integrated management of fever in children across different levels of care.
Although this scoping review does not evaluate the quality of available evidence, contributions are made to future efforts to better understand the population (parents and/or health professionals) regarding children with fever through studies carried out in the units. Based on this, it may be suggested that good practice documents be designed to update procedures in the context of IS consultation and the construction of interinstitutional protocols. Health marketing strategies and informational instruments must be inherent, whether through individual face-to-face consultations, group actions, or teleconsultations.
Author contributions
Conceptualization, J.M., L.B. and B.M.; data curation, J.M., L.B. and B.M.; formal analysis, J.M., L.B. and B.M.; investigation, J.M., L.B. and B.M.; methodology, J.M., L.B. and B.M.; project administration, J.M., L.B. and B.M.; resources, J.M., L.B. and B.M.; software, J.M., L.B. and B.M.; supervision, J.M., L.B. and B.M.; validation, J.M., L.B. and B.M.; visualization, J.M., L.B. and B.M.; writing-original draft, J.M., L.B. and B.M.; writing-review and editing, J.M., L.B. and B.M.

