Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Heart failure (HF) is defined as a clinical syndrome characterized by symptoms such as dyspnea, orthopnea, and lower limb edema, alongside signs like elevated jugular venous pressure and pulmonary congestion. Identifying the etiology of HF is a critical step in its diagnosis (McDonagh et al., 2021).
This condition is associated with high morbidity and mortality rates. Its prevalence has been rising due to population aging and advancements in the treatment of ischemic heart disease. Consequently, individuals with HF experience prolonged lives but continue to face poor prognoses (Emmons-Bell et al., 2022; Savarese et al., 2023).
The disease course is variable, often marked by acute decompensations requiring repeated hospitalizations (Savarese et al., 2023). As the disease progresses, functional capacity and quality of life decline (McDonagh et al., 2021). Current American and European guidelines highlight the importance of palliative care (PC) for individuals with HF at all stages of the disease (Heidenreich et al., 2022; McDonagh et al., 2021).
The World Health Organization (World Health Organization) defines PC as an "approach that improves the quality of life of patients and their families facing problems associated with life-threatening illness" (World Health Organization, 2020). The American Heart Association (AHA) emphasizes that PC ensures or enhances the quality of life for individuals with HF, advocating for its integration into a formal system of interdisciplinary care (Heidenreich et al., 2022). Similarly, the European Society of Cardiology (ESC) recommends PC for all individuals with HF, irrespective of the disease stage (McDonagh et al., 2021).
This review aims to map the scientific evidence on PC for individuals with HF in critical care contexts. The research question was framed using the PCC (Person, Concept, Context) strategy: "What constitutes PC for individuals with HF in critical care?" Inclusion and exclusion criteria are outlined in Table 1.
Table 1 Inclusion and Exclusion Criteria
| Inclusion Criteria |
| Population: Adults aged 19 or over, with no defined age limit, diagnosed with HF. |
| Concept: Need for PC. |
| Background: Admission to intensive care units (ICU) or recourse to the emergency department (ED), whose main reason for admission was HF. |
| Types of sources: All types of studies: quantitative and/or qualitative. Were considered: - Primary studies: experimental and quasi-experimental, randomized clinical trials, prospective and retrospective cohort studies, case-control studies, analytical and descriptive cross-sectional studies, as well as descriptive observational study designs, including case series and case studies. - Qualitative studies: phenomenological studies, ethographic studies, grounded theory, descriptive studies and action research. - Systematic reviews, meta-analyses, guidelines, texts, letters and opinion articles. |
| Exclusion Criteria |
| Population: Children (aged 18 or under); Adults with HF whose reason for hospitalization or emergency episode is not related to their pathology (such as other cardiovascular pathologies); People with other chronic diseases and/or cancer. |
| Concept: People hospitalized with HF without PC needs |
| Context: Hospitalization in wards or institutions in the community; Internment in hospices. |
1. Methods
A review protocol was developed and registered on the OSF platform (https://doi.org/10.17605/OSF.IO/7YDJT). This scoping review followed the methodology proposed by the Joanna Briggs Institute (JBI) (Aromataris & Munn, 2020), adhering to the PRISMA-ScR EQUATOR checklist (Tricco et al., 2018).
The research strategy comprised three phases. Firstly, a preliminary search was carried out in the MEDLINE Complete and CINAHL databases (via EBSCO), using natural language terms to identify articles related to the subject under study. Subsequently, the titles, abstracts, and keywords were read and analyzed to identify the most relevant indexed terms for the research.
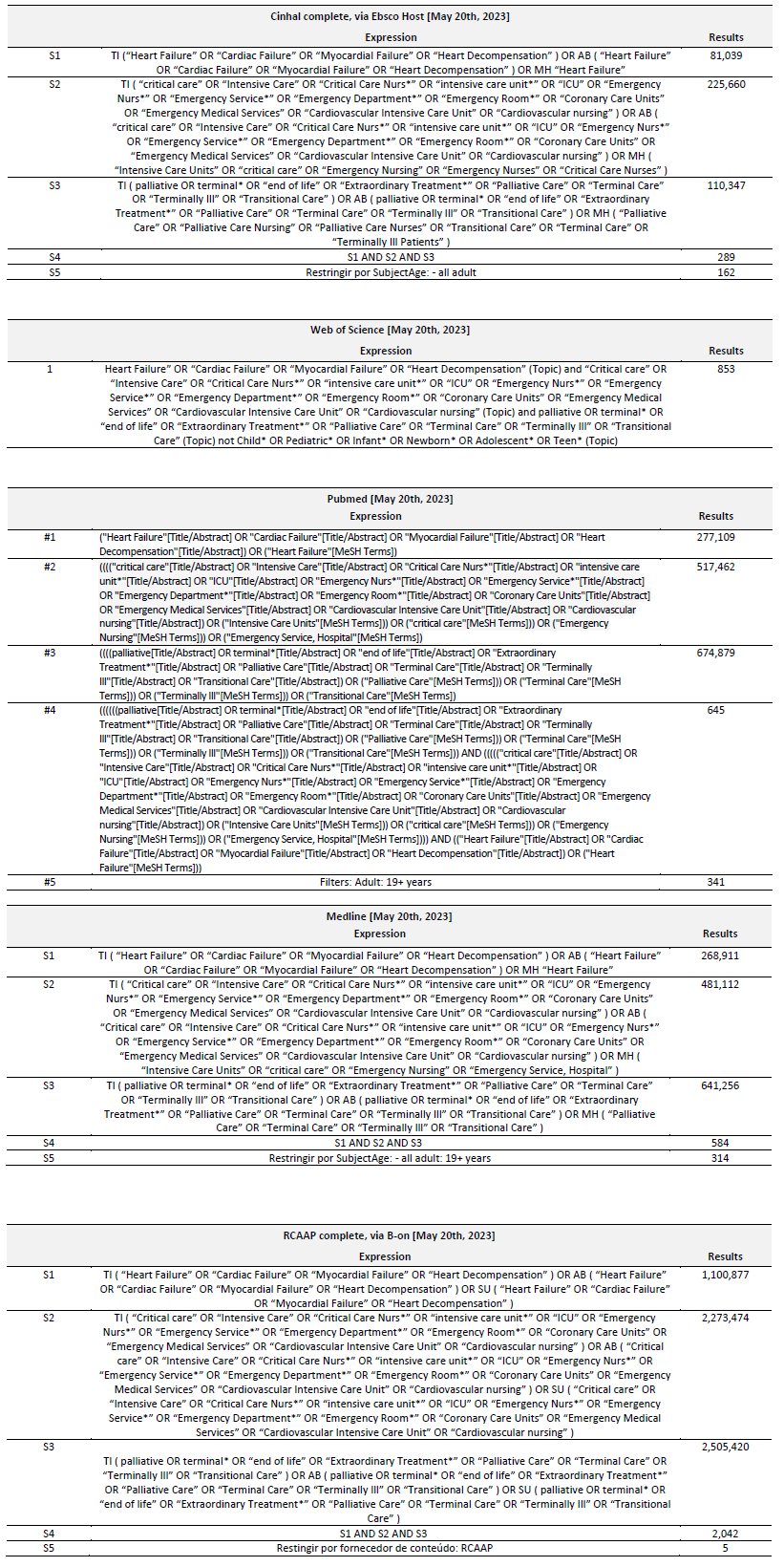
In the second phase, and with the aim of developing the complete research strategy, comprehensive searches were conducted in databases (MEDLINE Complete, CINAHL, PubMed, Web of Science, and RCAAP), combining natural language and indexed terms using Boolean operators ("OR" and "AND"). These searches were performed on May 20, 2024, and detailed strategies for each database are provided in Annex 1.
In the third phase of the research, the references of the articles selected for this review were analyzed to find complementary studies that could answer the research question.
Articles in Portuguese, English, and Spanish were included, with no restrictions on publication date. References were managed using Zotero®, and duplicates were removed using Rayyan®. Two independent reviewers screened titles and abstracts based on inclusion and exclusion criteria. Conflicts were resolved through discussion or consultation with a third reviewer.
1.1 Data collection instrument
In order to address the objectives and answer the review question, data extraction was carried out using a table designed by the authors as part of the review protocol in accordance with the guidelines of the JBI (Aromataris & Munn, 2020).
2. Results
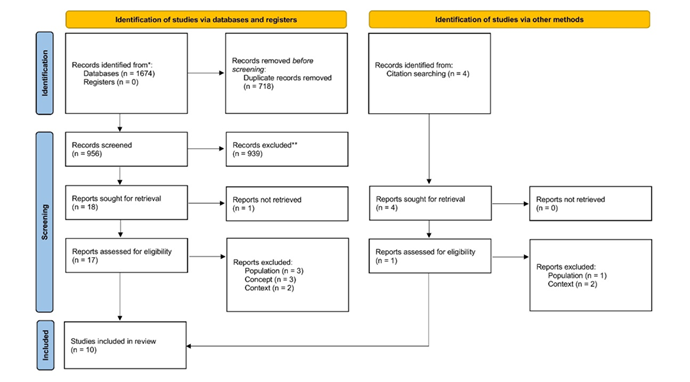
A search of the databases yielded 1,674 articles. After removing duplicates, 956 articles remained. Following a review of the titles and abstracts, 939 articles were excluded for not meeting the inclusion criteria, leaving 18 articles for full-text analysis. The full text of one source could not be obtained. After reading the remaining articles in full, 9 were selected for inclusion in this review.
Subsequently, an analysis of the bibliographic references of the included articles identified 4 additional sources of evidence, which were retrieved and considered eligible for full-text analysis. Of these, 3 articles were excluded after detailed review, resulting in 1 additional source being included in the review.
In total, this review included 10 articles. The article selection process is detailed in the PRISMA flowchart (Page et al., 2021) presented in Figure 1.
The selected studies were published between 2006 and 2024 with 5 from the United States (USA) (Aaronson et al., 2019; Brady, 2016; George et al., 2015; Wiencek & Webster, 2012; Wingate & Wiegand, 2008) , one each from Spain (López et al., 2016), Italy (Romano', 2019), Taiwan (Chou et al., 2024), the Netherlands (Beuks et al., 2006), and the United Kingdom (Kumar et al., 2009).
Table 2 shows the content extracted from the sources of evidence.
Table 2 Data extraction table
| Author and year | Title | Type of study | Other details (country, newspaper, volume, number, pages) | Context | Participants | Concept |
| López, S, et al 2016 | Detection of the palliative patient with acute heart failure at urgencias | Opinion letter | Spain, An. Sist. Sanit. Navar. 2016; 39 (2): 323-324 | ED | Person with HF | There are no validated scales for the ED that promote the identification of palliative care (PC) needs. There have been calls for the development of tools to quickly identify PC needs among patients with acute cardiac issues in the ED. |
| George et al., 2015 | Content Validation of a Novel Screening Tool to Identify Emergency Department Patients with Significant Palliative Care Needs | Primary study - Validation | USA, Academic Emergency Medicine, 22(7), 823-837. | ED | Anyone with advanced chronic illness (including HF) | There are no validated PC needs screening tools for the ED; In this study, a PC needs screening tool was developed and validated for clients with chronic illnesses in the ED. The tool can be applied by different professionals and does not require additional interviews with the client. |
| Wingate, S; Weigard, D, 2008 | End-of-life care in the critical care unit for patients with heart failure | Review article | USA, Critical Care Nurse, 28(2), 84-94 | ICU | Person with HF | Interventions should be planned based on the prognosis, which should be discussed by the team. Consider initiating and discontinuing life support measures. A family conference should be held 72 hours after admission, ensuring open communication with the patient and family, and providing information on the current condition, prognosis, and care objectives. Manage implantable cardiac devices and ventricular assist devices (VADs). The patient must give informed consent. Advance directives (AD) are essential for decision-making by the team and/or family. Adjust pharmacological therapy according to symptoms to control discomfort. Administer analgesics (morphine), sedatives (diazepam and midazolam), diuretics, and anticholinergics (for noisy breathing). Position the patient appropriately. Administer oxygen (only in the presence of hypoxia) and use fans to relieve dyspnea. Apply nitroglycerin ointment (to the chest) before bedtime.The focus of end-of-life care should be on PC, with symptom control as the central goal. It is important to define the place of death, and the "participants" involved, while also adapting care to cultural and religious preferences. Remove vital signs monitors and deactivate unnecessary alarms. Prepare the family for changes in clinical status and ensure unrestricted access to the patient. Provide available resources for bereavement support and encourage participation in bereavement groups. |
| Brady, D., 2016 | Planning for Deactivation of Implantable Cardioverter Defibrillators at the End of Life in Patients With Heart Failure | Review article | USA, Critical Care Nurse, 36(6), 24-31 | Patients with HF | When the implantable cardioverter-defibrillator (ICD) is deactivated, the principles of bioethics and informed consent must be upheld. The right to continue active ICD therapies must be guaranteed, even if the decision is made not to perform Do Not Resuscitate (DNR) orders and/or comfort care. Institutions should have policies and procedures in place to systematically approach device deactivation, including procedures for both urgent and non-urgent deactivation. Recommendations for ICD management: Pre-implantation Discussion - Discussions about the ICD should be initiated in all care settings prior to implantation. Education is essential, and nurses can play a key role in this process.Triggers for discussion - After ICD shocks; frequent hospitalizations (3 or more within 6 months); when DNR orders are in place and/or signs of poor prognosis are present; during transfer to a PC unit; inclusion of discussion in end-of-life conferences. Device screening upon admission - Assess the presence of the device through clinical observation; interrogate the device; document the information. Multidisciplinary team discussion and integration of PC in critical care settings - In the ICU, PC can assist in symptom management and relieve suffering. Bedside nurses' ability to deactivate ICDs - Bedside nurses should be trained to deactivate the ICD using a magnet and should collaborate with the patient and family in the deactivation decision-making process. | |
| Aaronson, E., et al 2019 | The Surprise Question Can Be Used to Identify Heart Failure Patients in the Emergency Department Who Would Benefit From Palliative Care | Prospective cohort study | USA, Journal of Pain and Symptom Management, 57(5), 944-951 | ED | People with HF who go to the ED | A strategy is required to identify individuals with HF who present to the ED with PC needs. The "Surprise Question" appears to be an important tool for identifying HF patients in the ED who could benefit from PC. |
| Wiencek, C; Webster, L 2012 | Preparing for Sudden Cardiac Death Following Implantable Cardioverter-Defibrillator Deactivation | Case Study | USA, Journal of Hospice & Palliative Nursing, 14(7), 478-483 | ICU | Person with HF | Nurses should support the decision to deactivate cardiac devices and offer support to the family. They should also be knowledgeable about how to deactivate the device. There should be ongoing discussion regarding the management of ICDs, with proactive communication focusing on goals and objectives rather than solely on treatments. Decision-making should be shared among the healthcare team, the patient, and the family. Informed consent is required for the deactivation of life-sustaining therapies. AD should be used and encouraged. PC teams should be involved early to ensure symptom control and enhance quality of life. |
| Kumar G., et al, 2009 | Withdrawal of intensive care treatment at home - 'a good death' | Case studies | United Kingdom, Anaesthesia and Intensive Care, 37(3), 484-486. | ICU | People with HF | It is a professional obligation for doctors and nurses to take measures that ensure a dignified death. Interventions should focus on symptom management and strategies to promote comfort and dignity (e.g., discontinuation of treatments), while also respecting the patient's autonomy. Clinical stability is often required to allow a person receiving invasive treatments to die at home. This process can be led by nurses, with PC and primary healthcare teams playing a crucial role. In many cases, there is no living will. Additionally, patient consent may be limited due to sedation. |
| Romano, M., 2019 | The Role of Palliative Care in the Cardiac Intensive Care Unit | Review article | Italy, Healthcare, 7(1), 30. | ICU | People with cardiovascular disease (especially HF) | Interventions that cause suffering should not be continued, particularly to satisfy the wishes of the family, especially if such decisions result in further suffering for the patient. The therapeutic plan should be carefully planned, periodically reviewed, and discussed with the patient and their family. The use of AD should be encouraged. Symptom management is essential. The author mentions an algorithm for ICD deactivation and suspension of VADs. Discontinuing ICD therapies and/or VADs activity is a palliative end-of-life measure and should not be confused with euthanasia or assisted suicide. This process must respect cultural beliefs and applicable legislation. Additionally, alarm systems related to VADs should be disabled. The family must be an integral part of this process. Midazolam and propofol, in combination with opioids, are recommended for palliative sedation. It is essential to ensure that bioethical principles are upheld throughout the process. |
| Chou, P., et al, 2024 | Trends and Changes in Intensive Care Use for Patients With Heart Failure in the Last Month of Life | Observational study | Taiwan, INQUIRY: The Journal of Health Care Organization, Provision, and Financing, 61, 00469580241239143. | ICU | People with HF in end-of-life care | Symptoms such as depression and anxiety should be closely monitored. The patient should have the autonomy to make decisions regarding life-sustaining treatments in end-of-life care. Allowing the patient to die at home while breathing spontaneously, without orotracheal intubation, is considered a preferable way to approach death. The presence of the family at the time of death is viewed as an important symbol of fulfillment. Cultural factors significantly influence the shared decision-making process between doctors and patients with end-stage HF. |
| Beuks, B., et al, 2006 | A good death | Case Study | Netherlands, Intensive Care Medicine, 32(5), 752-753 | ICU | HF patient in ICU - case study | The multidisciplinary team must reach a consensus on the patient's prognosis and support the patient's informed decision to die at home. They must provide the necessary resources to facilitate this process. Dying at home should be a viable option for the patient and can be planned if the clinical situation permits. Communication with caregivers should be maintained, and "local circumstances" must be assessed. These considerations must align with the patient's cultural values and beliefs. |
The analysis of the results obtained allowed them to be aggregated into 2 categories and 8 subcategories, as shown in Table 3.
Table 3 Organization of results into categories
| Category | Subcategory | Frequency | Authors |
| A. PC in the ED | A1. Identifying the need for PC | 3 | (Aaronson et al., 2019; George et al., 2015; López et al., 2016) |
| B. PC in the ICU | B1. Symptom management | 5 | (Chou et al., 2024; Kumar et al., 2009; Romano’, 2019; Wiencek & Webster, 2012; Wingate & Wiegand, 2008) |
| B2. Communication, decision-making and advance care planning | 5 | (Beuks et al., 2006; Chou et al., 2024; Romano’, 2019; Wiencek & Webster, 2012; Wingate & Wiegand, 2008) | |
| B3. ICD and VADs management | 4 | (Brady, 2016; Romano’, 2019; Wiencek & Webster, 2012; Wingate & Wiegand, 2008) | |
| B4. Dying process | 4 | (Beuks et al., 2006; Chou et al., 2024; Kumar et al., 2009; Wingate & Wiegand, 2008) | |
| B5. Culturally sensitive care | 3 | (Beuks et al., 2006; Chou et al., 2024; Romano’, 2019) | |
| B6. Definition of prognosis | 3 | (Beuks et al., 2006; Brady, 2016; Wingate & Wiegand, 2008) | |
| B7. Principles of bioethics and informed consent | 2 | Brady, 2016; Kumar et al., 2009 |
2.1 Quality of the articles included.
When preparing a scoping review, there is no requirement to assess the methodological quality of the studies included (Aromataris & Munn, 2020). However, during the review process, a preliminary methodological analysis of the selected studies was conducted.
The 10 articles included in the review employ different methodologies: 3 narrative reviews, 3 case studies, 1 opinion article (letter to the editor), 1 validation study of a tool for identifying palliative needs in the ED, 1 observational study, and 1 cohort study. The inclusion of opinion articles and case studies may limit the applicability of the findings due to their subjective nature. However, review, validation, cohort, and observational studies provide a more structured and robust foundation for understanding the topic. Narrative reviews offer a synthesis of various sources of evidence, while the validation study provides a tool for practical application in care delivery.
3. Discussion
People with HF, at some stage of their illness, are admitted to critical care. These care environments (ICU and ED) should be integral to the provision of adequate PC (Bierle et al., 2021).
From the analysis of the results, it is evident that in the category of PC in the ED, the evidence shows that identifying palliative needs is essential for referral to specialized PC services (Aaronson et al., 2019; George et al., 2015; López et al., 2016). The ED represents a context that poses challenges to the provision of PC (Pereira & Reis-Pina, 2021). However, individuals with HF have several resources in this context due to the decompensation of symptoms inherent in the disease’s progression. Thus, this setting is crucial for identifying PC needs in people with HF (Lipinski et al., 2018). Identifying unmet palliative needs is a key step in providing PC (Heidenreich et al., 2022; McDonagh et al., 2021). American guidelines even state that care should not be limited to specialized PC but should encompass all healthcare settings where care is provided to these individuals (Heidenreich et al., 2022). However, clear guidelines for operationalizing early referral are lacking (Egídio De Sousa et al., 2021).
In the PC in ICU category, there are four subcategories (B1, B2, B3, and B6), which align with the AHA guidelines (Heidenreich et al., 2022) and ESC guidelines (McDonagh et al., 2021). Regarding the subcategory of symptom control, most authors agree that symptoms should be managed, although they do not specify pharmacological or non-pharmacological interventions. However, two authors mention interventions to be implemented for symptom control (Romano', 2019; Wingate & Wiegand, 2008). The ESC guidelines offer clear guidance on symptom management, including specific interventions (McDonagh et al., 2021).
Romano' (2019) highlights thirst and spiritual well-being as often underestimated symptoms that deserve more attention from healthcare professionals. Literature suggests that people with advanced HF experience high levels of spirituality, yet often have unmet spiritual needs. Addressing these spiritual needs can improve quality of life (Bierle et al., 2021; Tobin et al., 2022). Neither of the guidelines mentioned addresses this category of symptoms (Heidenreich et al., 2022; McDonagh et al., 2021).
The results obtained in the subcategories of ICD and VADs management and the definition of prognosis align with the two guidelines (Heidenreich et al., 2022; McDonagh et al., 2021). Two authors even provide clear guidelines and procedures for deactivating ICDs, with specific protocols for device deactivation (Brady, 2016; Romano', 2019). On the other hand, there seems to be consensus, both in the studies included and in the literature, that HF follows a unique and unpredictable course, making it difficult to predict the disease's progression (Bierle et al., 2021; Egídio De Sousa et al., 2021).
In the subcategory of the dying process, the choice of place and participants in the dying process proved to be crucial. The literature supports this view, stating that the individual should have the option to choose where and with whom they wish to die. The AD is an essential step in this regard (Lee & Hwang, 2022). As suggested by a study in this review, interventions specific to the ICU can hinder the transfer of these individuals to their homes, and coordination with community care is essential (Beuks et al., 2006). Quinn et al. (2020) suggest that while most people die in hospitals, PC in end-of-life care can enable individuals to die at home.
Regarding the subcategory of communication, decision-making, and advance directives, it should be noted that the authors do not address the timing of the AD (which is referred to by various authors in different ways but with the same meaning). Furthermore, the two guidelines do not define a specific timeframe either. Lee & Hwang (2022) propose that care planning should begin early in the illness and continue throughout. During the end-of-life phase, it is suggested that any unresolved AD should be conducted or existing directives should be reviewed. It is important to clarify and affirm the individual's wishes regarding resuscitation efforts, life support measures, and the steps to ensure a dignified death, including decisions on the place and people present during the dying process. Different issues should be addressed at different stages of the illness.
In light of the subcategories discussed, culture emerges as a highly relevant topic, as suggested by three authors (Beuks et al., 2006; Chou et al., 2024; Romano', 2019). Traditions and ideologies can significantly influence the acceptance and delivery of PC (Hill et al., 2023). Current clinical consensus indicates that from the first interaction between the patient and healthcare professionals, there should be open communication, validation of the disease's unique progression and often uncertain prognosis, and recognition of the family’s and patient’s values (Hill et al., 2023). These elements can facilitate shared decision-making, as mentioned by some authors in this review (Beuks et al., 2006; Chou et al., 2024; Romano', 2019; Wiencek & Webster, 2012; Wingate & Wiegand, 2008). Additionally, it is essential to recognize the roles of family members. Understanding whether they are involved in self-care, adapting to new conditions and limitations, or providing emotional and financial support during the disease’s progression is important (Hill et al., 2023). As noted in some of the studies included in this review, advance directives (Beuks et al., 2006; Chou et al., 2024; Romano', 2019; Wiencek & Webster, 2012; Wingate & Wiegand, 2008), end-of-life discussions, and decisions regarding the process, participants, and place of death can be addressed not only with the individual but also with significant others (Beuks et al., 2006; Chou et al., 2024; Kumar et al., 2009; Wingate & Wiegand, 2008). Recent literature supports this view (Hill et al., 2023).
Although PC has been achieved for people with HF in critical care, there are several barriers to its delivery in ICUs and EDs. Clinical decision-making is often made by cardiologists who lack academic training in PC (Silva et al., 2024). Thus, gaps in PC training and the shortage of specialists in this field are significant barriers (Romanò, 2020; Silva et al., 2024). A clinical approach focused on prognosis, coupled with difficulty in establishing it, hinders recognition of the need for PC. Moreover, there is currently a stigma surrounding the implementation of palliative interventions, as PC is often associated with death and the dying process (Romanò, 2020).
The limitations of this review include the fact that studies in languages other than Portuguese, English, and Spanish were not included. Furthermore, no implications for practice can be drawn, as the methodological quality of the included articles was not assessed.
3.1. Practical applicability
The findings of this review clearly highlight the urgent need to ensure PC for individuals with HF throughout the course of their illness. While several benefits for people with this condition have been identified, barriers that limit the fulfillment of their palliative needs have also emerged.
Given the barriers to the provision of PC mentioned earlier, investing in PC training for professionals on the multidisciplinary team could be crucial to enhancing their understanding of generalist PC delivery. Furthermore, although further research is still required, nurses with expertise in HF could play a significant role in implementing measures and/or referring patients to specialized PC services (Nunciaroni et al., 2023).
Assessing symptoms can be helpful in addressing the specific needs of these patients. Therefore, using tools such as the Edmonton Symptom Assessment System (ESAS) can be beneficial for guiding clinical practice and tailoring interventions to meet individual needs. In some cases, nurses can be key facilitators in the application of these tools, enabling quicker responses within the multidisciplinary team. Following the symptom assessment, an individualized care plan should be developed, including interventions that target physical symptoms (such as dyspnea, pain, and fatigue), psychological symptoms (depression and anxiety), as well as social and spiritual needs (Beattie et al., 2020).
The existence of clear action protocols in the ICU, including triggers for discussions within the multidisciplinary team and defined timelines for referral to specialized PC, can be essential to ensuring effective symptom management and alleviating suffering (Sobanski et al., 2020).
Several studies have explored the assessment and screening of palliative needs in the ED, identifying tools that can aid in this process. In this context, the use of the "Surprise Question" could be instrumental in early identification of unmet palliative needs in the ED (Ribeiro et al., 2024; Van Lummel et al., 2022).
Conclusion
There were no deviations from the protocol during the scoping review.
Although the majority of authors, as well as the two guidelines discussed in this review, advocate for early PC interventions throughout the course of the disease, most of the care discussed pertains to the end-of-life phase. The most prominent early intervention approach is seen in the management of device-related complications (DCI), where it is emphasized that care discussions and planning should occur during the implementation of the treatment. Both the American and European guidelines support the inclusion of PC throughout the disease trajectory. However, only the American guidelines provide clear recommendations for all healthcare settings.
Although no specific recommendations are provided for various care settings, it was found that critical care is a crucial environment for promoting PC and enhancing the quality of life for these individuals. The ED serves as a key setting for identifying the palliative needs of patients with HF who present there. On the other hand, evidence indicates that the ICU has well-defined PC practices that should be considered throughout the illness, particularly regarding ICD deactivation, effective and proactive communication, decision-making, and advance care planning.
Including PC as a topic in the training curricula for nurses and doctors could be beneficial in enhancing their involvement in clinical practice.
Authors' contribution
Conceptualization, F.P; dada curation, F.P.; formal analysis, F.P., L.B. and P.P.S.; investigation, F.P., L.B. and P.P.S.; methodology, F.P., L.B. and P.P.S.; project administration, F.P.; resources, F.P.; supervision, L.B. and P.P.S.; validation, L.B. and P.P.S.; visualization, F.P. and P.P.S.; writing-original draft, F.P.; writing-review and editing, F.P.