











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
The concept of obstetric violence has garnered significant attention in the media recently (Mendes et al., 2022). The concept involves multiple factors and requires the participation of professional associations, health institutions, health professionals, and expectant mothers and their families. Obstetric violence refers to abusive, disrespectful, invasive, or discriminatory practices during labor, as indicated by scientific evidence (Abbasi et al., 2022; A. D. S. Melo et al., 2020; Silva et al., 2023). Other authors also mention that this nomenclature refers to any act of violence directed at pregnant, parturient, or puerperal women or their children. This denotes disrespect for their autonomy, physical and mental integrity, desires, and feelings (Ribeiro et al., 2021).
The World Health Organization (WHO) recognizes that intrapartum care is crucial for the well-being of women and their babies and has issued recommendations to ensure a positive birth experience (WHO, 2018). However, the concept of "obstetric violence" can have a detrimental impact on professional practice (Chadwick, 2021; Terribile & Filho, 2023). Research indicates that pregnant women often experience undignified care and privacy violations (Abbasi et al., 2022; Dwekat et al., 2021; Escobal et al., 2022). According to Martínez-Galiano et al. (2021), two out of three women believe they have been subjected to some form of violence. Egan et al. (2016) highlight that mistreatment violating human and reproductive rights is linked to deficiencies in infrastructure, service organization, professional training, and societal perceptions of women. Therefore, the notion of obstetric violence calls for not only social attention but also legal intervention and analysis.
1. State of the art
Obstetric violence has sparked numerous controversies globally. Several authors have noted that it is still culturally accepted (B. L. P. L. Melo et al., 2022), and there is a lack of consensus among healthcare professionals such as physicians, nurses, and researchers. Chadwick (2023) highlights the dangers of downplaying the severity of obstetric violence. In Portugal, researchers have already focused on studying satisfaction with childbirth. For example, Costa et al. (2004) assessed childbirth experience and satisfaction using a questionnaire with eight subscales. However, most studies using this questionnaire have centered on women's satisfaction with childbirth, with no specific focus on good obstetric practices.
In recent years, there have been numerous studies aimed at assessing women's perception of obstetric violence. These studies have led to the development of several questionnaires designed to evaluate obstetric violence in various settings. For instance, in 2020, a questionnaire was introduced to gauge the perception of obstetric violence among nursing, midwifery, and medical students (Mena-Tudela et al., 2020). Taking a different approach, VanGompel et al. (2022) endeavored to characterize and quantify obstetric racism. At the same time, Paiz et al. (2022) proposed a framework for an instrument to measure the degree of inadequate treatment of women during childbirth.
The development of a scale to assess obstetric violence in Chile was justified by its social relevance (Castro & Rates, 2021). This scale garnered attention in Spain, where it was adapted and culturally validated (Torre et al., 2023). Furthermore, Akik (2023) adapted a questionnaire on obstetric violence to fit Turkish culture, which was originally developed for a national study in Mexico to evaluate factors related to the experience of obstetric violence (Castro & Frías, 2020).
Obstetric violence can manifest in various forms, influenced by the specific country and culture in which the woman is situated (Perrotte et al., 2020). Given the existing literature, a questionnaire was administered to the Portuguese population, aligning with the WHO's guidelines for best obstetric practices. In this context, obstetric violence refers to actions carried out by healthcare professionals that contravene the recommended best practices issued by the WHO. This study aimed to ascertain whether there is empirical evidence supporting a multidimensional structure for a scale that evaluates the perception of obstetric violence and whether obstetric violence can be effectively gauged using a measurement instrument.
2. Methods and data collection instruments
A lack of available assessment tools for measuring the perception of obstetric violence in Portugal led to the creation of a new instrument. Developed following WHO guidelines for a positive birth experience, a multidisciplinary team of experts transformed these recommendations into 38 statements. Four specialists in obstetric nursing, including individuals with PhDs in Education, Psychology, and Nursing, analyzed these statements. A Likert scale was then constructed to allow responses ranging from 1 to 4, with 1 representing maximum disagreement and 4 representing maximum agreement for each item.
The statements were then presented to a diverse group of ten women of varying ages and educational levels. After achieving consensus on the evaluation of the items, a sociodemographic questionnaire was developed to collect information about the participants, including whether they had been mothers for less than five years, details about their delivery, current and maternal age, education level, marital status, place of residence, number of children, childbirth preparation, and pregnancy care received. The research protocol included this sociodemographic questionnaire and the 38 statements to assess the perception of the birth experience, satisfaction with life, and the quality of care received during labor and delivery.
Following approval by the Ethics Committee of the University of the Azores, the protocol was uploaded to the Survey 123 platform and shared on social media platforms such as Facebook. To mitigate the potential impact of the term "obstetric violence" on participants' responses, the study was presented as aiming to explore Portuguese women's perceptions of their labor experiences. Participants were assured of the anonymity of their responses and were informed of their ability to withdraw from the questionnaire at any time.
2.1 Sample
The study involved 615 women who had been mothers for less than five years. The average age of the participants was 34.02 years (SD = 5.01). Most participants reported having higher education (65.7%) and being married (50.9%). Regarding geographic residence, 53.2% lived in mainland Portugal, 40.3% in the Azores Archipelago, and 6.5% in the Madeira Archipelago. Regarding the type of delivery, 39.7% were eutocic, 37.7% were delivered by cesarean section, and 22.6% were instrumentalized.
2.2 Statistical analysis
The data were analyzed using SPSS software, specifically version 28 for MacOS and AMOS21 for Windows. Statistical procedures included an exploratory factor analysis (EFA) and verification of Cronbach’s alphas to assess the correlation between items and measure the theoretical construct. After identifying items with the highest correlation and satisfactory commonalities (<0.5) (Matos & Rodrigues, 2019), 10 items were obtained, divided into two dimensions: 5 items for the emotional dimension and five for the physical dimension.
After conducting confirmatory factor analysis (CFA) with maximum likelihood estimation, the overall fit quality of the factor model was assessed using the Chi-square Adjustment test (X2), where a value of X2/g.l. Less than 5 indicates an acceptable model. Additionally, a good fit was shown by the Comparative Fit Index (CFI), Goodness of Fit Index (GFI), and Root Mean Square Error of Approximation (RMSEA) values close to 1 and RMSEA values below 0.05 (Marôco, 2021a, 2021b). The intensity and direction of the association between the dimensions of the instruments and convergent validation were determined using Spearman's correlation coefficient (rs). Lastly, the invariance of the scale's structure and parameters concerning the delivery type was evaluated.
3. Results
For the entire sample (N=615), the reliability coefficient of the 10-item scale was 0.82. The emotional dimension showed ( = 0.77, and the physical dimension showed ( = 0.72. The Kaiser-Meyer-Olkin measure, which assessed the data quality, revealed the suitability of the sample and the homogeneity of the variables (KMO = 0.865; X2(45) = 1677.106, p < 0.001). The item-total correlations were moderately high, ranging from 0.54 to 0.71.
Table 1 displays the positive factor loadings for the items comprising the two dimensions and the correlations between the original variables. The items exhibit Cronbach's alpha values greater than 0.70, indicating their adequacy. Furthermore, the factor analysis in Table 1 reveals that the various intercorrelations between the items indicate other latent factors.
Table 1 Normalized factor loadings of the two-factor model and Cronbach's alpha
| Item | Statement | Factor Load | Cronbach's alpha if you delete the item | |
| Emotional Dimension | 2 | They devalued my attempts to push. | 0.57 | 0.79 |
| 6 | They told me to shut up when I screamed. | 0.67 | 0.81 | |
| 8 | I felt insulted during labor and/or delivery. | 0.86 | 0.79 | |
| 9 | I felt criticized by health professionals for the options I took. | 0.80 | 0.81 | |
| 10 | My preferences were not met. | 0.53 | 0.81 | |
| Physics Dimension | 1 | They cut my perineum without anesthesia. | 0.70 | 0.80 |
| 3 | They pushed my belly to give birth to the baby. | 0.69 | 0.82 | |
| 4 | They did more than three vaginal touches. | 0.52 | 0.81 | |
| 5 | They cut my perineum without any explanation. | 0.77 | 0.80 | |
| 7 | They forced myself to lie on my back and with my legs elevated to have my son. | 0.68 | 0.79 |
The results in Figure 1 indicate that the quality indices of the confirmatory factor model demonstrate values that support a good fit. Specifically, the SRMR is below 0.08, X2/g.l. is less than 5, and both GFI and CFI fall within the range of [0.9, 0.95], while the TLI is close to 1, all of which indicate a firm fit.
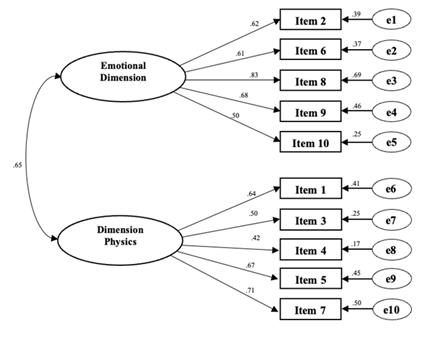
Figure 1 Confirmatory Factor Analysis of the Obstetric Violence Scale X2(34) = 150.946; p < 0.001, X2df = 4.440; CFI = 0.93; TLI = 0.88; GFI = 0.95; RMSEA = 0.07, p <0.001; SRMR = 0.05
Table 2 shows the results of the confirmatory factor models' quality analysis for each type of delivery. The model analyzed with the sample of women undergoing cesarean section shows poor values (CFI = 0.84; TLI = 0.45; RMSEA = 0.10).
Table 2 Evaluation of the Quality of the Model for the type of delivery
| Type of delivery | Quality of the factorial model |
|---|---|
| Eutocics (n=244) | X 2 (34) = 89.627; p < 0.001, X 2 df = 2.636; CFI = 0.90; TLI = 0.88; GFI = 0.93; RMSEA = 0.082, p = 0.006 SRMR = 0.06 |
| Cesarean sections (n=232) | X 2 (34) = 118.573; p < 0.001, X 2 df = 3.487; CFI = 0.84; TLI = 0.45; GFI = 0.90; RMSEA = 0.10, p < 0.001 SRMR = 0.07 |
| Instrumentalized (n=139) | X 2 (34) = 60.323; p = 0.004, X 2 df = 1.774; CFI = 0.92; TLI = 0.89; GFI = 0.93; RMSEA = 0.075, p = 0.09 SRMR = 0.06 |
| Note: X 2 df = chi-square/degrees of freedom; CFI = Comparative Fit Index; TLI = Tucker-Lewis Index; Goodness of Fit Index; RMSEA = Root Mean Square Error of Approximation; SRMR = Standardized Root Mean Square Residual. |
In examining the midpoint of the obstetric violence perception assessment scale, the participants demonstrated an average value of 16.26 (SD = 6.14). The descriptive statistics indicate that 91.1% of the participants viewed the birth experience positively. Upon evaluating convergent validity, it was observed that the scale for assessing the perception of obstetric violence exhibits a weak correlation with the scale of life satisfaction (rs = 0.23; p < 0.001) and a strong correlation with the perception of the woman feeling well cared for (rs = 0.63; p < 0.001).
3.1 Measurement Invariance
One of the benefits of confirmatory factor analysis is its ability to assess whether the structure and parameters of a specific instrument remain consistent across different groups. In this study, categorical variables were created to test invariance for the type of delivery (eutocic, cesarean section, instrumentalized). The invariance test began with adjusting each group's confirmatory factor analysis model to ensure adequate fit. Tests for invariance were conducted by comparing the group classifications for equality of factor loadings of items (metric invariance) and equality of item intercepts (scalar invariance).
3.1.1 Invariances analysis in the type of labor
Upon analyzing the configurational model adjusted for the type of delivery group, it was noted that the model had a poor fit with X2(102) = 268.526; p < 0.001, CFI = 0.89, TLI = 0.85; RMSEA = 0.052, 90% CI [0.044, 0.059] and SRMR = 0.063. The fit for the metric model was also slightly different with X2(118) = 302.724; p < 0.001, CFI = 0.87, TLI = 0.86; RMSEA = 0.051, 90% CI [0.044, 0.058] and SRMR = 0.063. Considering the commonly used criterion ΔCFI ≤ 0.0127 (Cheung & Rensvold, 2002), test results X2 and ΔCFI indicate a decrease in fit due to the addition of equality constraints (ΔX2 = 34.198, ΔCFI = 0.013), confirming metric non-invariance.
In testing scalar invariance, it was determined whether the item intercepts were invariant between the groups of delivery types (eutocic, cesarean section, instrumentalized). The results of the scalar model X2(134) = 422.941; p < 0.001, CFI = 0.80, TLI = 0.80; RMSEA = 0.059, 90% CI [0.053, 0.066] and SRMR = 0.069 suggest that the assumption of scalar invariance holds (ΔX2 = 120.217, ΔCFI < 0.001). It was concluded that the factorial structure and the intercepts of the indicators were not similar in the type of delivery for the present sample of pregnant women.
4. Discussion
Designing a scale is a complex process requiring substantial psychometric evidence and thorough planning (Jain et al., 2016; Toronto & Remington, 2020). A factor analysis was conducted to uncover a set of underlying variables. Due to the limited understanding of the factorial structure, exploratory factor analysis was employed to assess the relationships between the observable variables. Subsequently, a confirmatory factor analysis was conducted to apply constraints on the factors and observable variables (Marôco, 2021a, 2021b).
In the current study, we confirmed a satisfactory level of internal consistency with Cronbach's alpha values exceeding 0.70, a threshold recognized as acceptable by Marôco and Garcia-Marques (2006). The assessment of the validity of the exploratory factor analysis, as measured by the homogeneity of the variables (KMO), revealed a strong correlation between the variables (>0.80), and we also established the statistical significance of the Bartlett test (Marôco, 2021b; Matos & Rodrigues, 2019). Furthermore, the item-total correlations were found to be acceptable. Additionally, the evaluation of the commonalities through the extraction method indicated commonalities greater than 0.50, indicating a significant proportion of common variance(Matos & Rodrigues, 2019).
The validity of the assumptions underlying factor analysis prompts the assessment of the model's goodness-of-fit indices. According to Marôco (2021a, 2021b), X2/df is considered acceptable if it is less than 5; SRMS < 0.08 indicates a good fit; GFI, CFI, and TLI between [0.9; 0.95] are deemed indicative of a good fit; and RMSEA within the range of ]0.05; 0.08] is considered an acceptable fit. Most models evaluated in the present study demonstrate a good overall fit. It is important to note that the only model assessed in the sample of women undergoing cesarean delivery showed poor CFI. Although this model can be adjusted for covariance errors (Marôco, 2021a), the unadjusted model was chosen because the sample included both planned and emergency cesarean sections. Research indicates that in most cases, the choice of cesarean section is made exclusively by the obstetrician without the woman's involvement. The woman's decision is often based on information from prior birthing experiences and influences from family members or the media (Barros & Franco, 2013; Escobal et al., 2022; Loke et al., 2019; Martins et al., 2018).
The invariance assessment for the type of delivery allowed us to confirm non-metric invariance (Chen, 2007; Cheung & Rensvold, 2002) and scalar invariance. Although a study by González et al. (2019) identified differences between types of delivery, they did not find significant differences in pregnant women's satisfaction regarding the type of delivery.
The strong correlation between the perception of obstetric violence and the satisfaction scale with the care provided seems to support the validity of the Obstetric Violence Assessment Scale. The developed scale appears to consist of two categories: the physical dimension and the psychological dimension. The physical dimension covers items related to physical mistreatment, such as pressure on the belly during childbirth, with literature reporting that more than half of women have been victims of this form of violence (Martínez-Galiano et al., 2021). The psychological dimension encompasses items related to insult, devaluation, or value judgment during labor and delivery. Power imbalances between physicians and patients, as well as the structural violence of societies that tolerate disrespectful and abusive behavior towards women, are identified as causes of obstetric violence (Perrotte et al., 2020).
Despite being developed in Portugal, the scale is designed for broader global applicability, drawing on WHO guidelines for best practices worldwide.
Conclusion
In conclusion, the issue of obstetric violence is a multifaceted and significant concern that has garnered increasing attention globally, including in Portugal. It encompasses a range of harmful practices that infringe on the physical and psychological well-being of women during childbirth. These include both overt and subtle forms of mistreatment, ranging from physical interventions without consent to emotional neglect or coercion. This study aimed to develop and validate a reliable instrument to measure the perception of obstetric violence, providing empirical evidence of a two-dimensional structure-emotional and physical-that aligns with women's experiences of mistreatment during labor and delivery.
The newly developed scale demonstrates solid psychometric properties, including strong internal consistency and satisfactory model fit indices. These results underscore its validity as a tool for assessing obstetric violence across different contexts. The findings also reveal that women's perceptions of obstetric violence are significantly correlated with their overall satisfaction with care, emphasizing the need to improve maternity care practices. This scale empowers healthcare professionals to gain deeper insights into women's experiences and pinpoint areas for enhancing obstetric care.
Importantly, the scale provides a means to shed light on the extent of obstetric violence, informing healthcare policies and interventions aimed at enhancing women's autonomy, dignity, and birth experiences. The study also points to the broader societal and structural factors that perpetuate such violence, including cultural norms, power imbalances between healthcare providers and patients, and systemic failures in maternal care. Addressing obstetric violence thus requires a concerted effort from healthcare professionals, policymakers, and civil society to uphold the rights and well-being of women, ensuring that childbirth is a respectful, empowering experience for all.
Authors' contribution
Conceptualization, J.M. and M.T.; data curation, J.M., P.A.S., S.C., S.L. and M.T.; formal analysis, J.M., P.A.S. and M.T.; investigation, J.M. and M.T.; methodology, J.M., P.A.S. and M.T.; project administration, J.M. and M.T.; resources, J.M. and M.T.; software, J.M. and P.A.S.; supervision, M.T; validation, J.M., P.A.S., S.C. and M.T.; visualization, J.M., P.A.S., S.C., S.L. and M.T.; writing-original draft, J.M, P.A.S. and M.T; writing-review and editing, J.M., P.A.S., S.C., S.L. and M.T.

