











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Missed nursing care corresponds to any care component that is omitted (totally or partially), or significantly postponed. This phenomenon can contribute to lengthened hospitalization periods, an increased number of falls and an increased prevalence of pressure ulcers/infections. It can also hinder effective pain management and result in medication errors, among other negative effects (Kalisch et al., 2009).
Quality of care, patient safety, and patient satisfaction are highly related to the nursing care provided. Therefore, it is important to evaluate the correlation between missed nursing care and the previously mentioned indicators of healthcare quality (Ahansaz et al., 2024).
Frequently, there is a need/choice to prioritize some forms of care over others, sometimes on a minute-by-minute basis. However, there is still no scientific foundation for this practice, which is essential for conducting further research. Aspects associated with the patient’s psychosocial needs, care planning, and ambulation appear to be often postponed/omitted, while other components (e.g., care related to the administration of therapeutic substances) are usually prioritized (Wakefield, 2014).
In general, the critically ill patient is admitted to a hospital through its emergency department. Afterward, he/she may or may not be admitted to the hospital’s intensive care unit (Mboya et al., 2023). Concerning emergency departments, if their size/human resources are inadequate, missed nursing care can take place, namely associated with high patient numbers, lack of physical space, and insufficient nurse-to-patient ratios (Duhalde et al., 2023). As regards intensive care units, since they accommodate highly complex tasks, they are particularly susceptible to the occurrence of nursing care omissions (Nobahar et al., 2023).
Nurses who provide care to critically ill patients or to patients whose condition may become acute are expected to do so effectively while ensuring care quality and safety (Wakefield, 2014). They have a direct influence on the quality of the provided care, since their role entails a close proximity to the care recipient. Therefore, it is crucial that they are able to identify care omissions and the respective potential causes, in order to establish precautionary measures (Bispo et al., 2023).
Given the reality portrayed above, it is essential to determine which nursing care omissions are common in emergency departments and intensive care units. Furthermore, it is important to ascertain the causes and effects of omissions, as well as possible mitigation strategies.
1. Methods
Firstly, we analyzed the state of the art regarding missed nursing care common to emergency departments and intensive care units, which revealed the absence of recent scientific evidence on this particular field of knowledge.
At that stage, we recognized an opportunity to map the existing scientific evidence related to the abovementioned phenomenon in a precise and summarized manner. Therefore, we decided to conduct this scoping review as a starting point for the production of knowledge on the subject under study, devising the following research question: “What is the current knowledge on missed nursing care common to emergency and intensive care settings?”
In addition, we considered four sub-themes, represented by the following questions:
Which nursing care omissions are common to the studied contexts?
Which causes of missed nursing care are common to the studied contexts?
Which effects of missed nursing care are common to the studied contexts?
Which mitigation strategies for missed nursing care are common to the studied contexts?
Thus, the present work’s development addresses the issue of nursing care omissions shared by emergency departments and intensive care units, being based on PRISMA guidelines. After choosing the research questions, we defined several inclusion and exclusion criteria. Next, we selected the relevant articles, applying the aforementioned criteria. Lastly, we analyzed and discussed the results that were obtained.
To perform the bibliographic search, we followed the PCC mnemonic (“Population,” “Concept,” and “Context”), which, following the same order, refers to “adult patient,” “missed nursing care,” and “intensive care and emergency department.” We employed a Boolean search method, using diverse terminology (free/natural terms, MeSH terms, and CINAHL subject headings) that reflected the established concept and context. To expand the search results, we did not use any terminology associated with the target population. Instead, we subsequently applied a filter within the different databases to select works involving adult patients.
To address the concept, we applied the terminology shown below:
As free/natural terms - omission OR miss* OR “medical error*” OR “health care error*” OR negligence OR “error of omission” OR “omission error” OR rationing OR “care left undone” OR “unfinished nursing care” OR “unfinished care” OR “delayed nursing care”;
As MeSH terms - “Medical Errors”;
As CINAHL subject headings - “Health Care Errors” OR Negligence.
To address the context, we applied the terminology shown below:
As free/natural terms - “critical care” OR “critical patient” OR “critical ill*” OR “critically ill patient” OR “emergency care” OR “Emergency Nurs*” OR “intensive care nurs*” OR “intensive care”;
As MeSH terms - “Emergency Nursing” OR “Critical Care Nursing” OR “critical care” OR “Critical Illness”;
As CINAHL subject headings - “Critical illness” OR “Emergency Nursing” OR “Critical Care Nursing” OR “Critical Care Nurses” OR “Intensive Care Units”.
The search was carried out between February 25 and March 26, 2024, within several databases: Scopus, Medline, PubMed, CINAHL, MedicLatina, and RCAAP.
As regards inclusion criteria, we considered articles freely available in full text, which corresponded to quantitative/qualitative/mixed studies, systematic literature reviews, or gray literature, and were written in Portuguese, English, or Spanish. With respect to publication date, no time limit was applied. In terms of content, we only included works that addressed the following topics:
Missed nursing care in adult critically ill patients admitted to emergency departments;
Missed nursing care in adult critically ill patients admitted to intensive care units;
Nursing care omissions in critically ill patients;
Factors that influence missed nursing care;
Mitigation strategies for missed nursing care;
Consequences of missed nursing care.
We also established various exclusion criteria, namely:
Documents focusing on medical diagnostic/prescription errors;
Studies addressing the concept of missed nursing care in other contexts;
Articles without free access to the full-text version;
Editorials, letters to the editor, commentaries, case studies, opinion pieces, book chapters, and master’s theses.
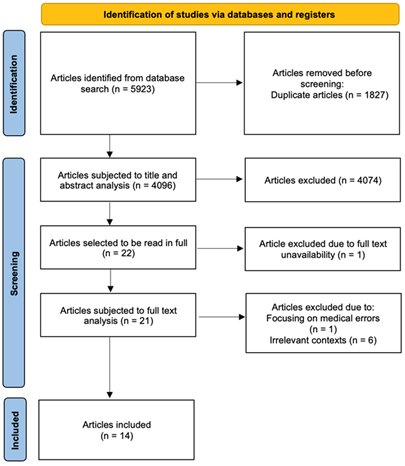
The database search produced a total of 5923 works, of which 1827 were duplicates. The Rayyan platform was used to perform title and abstract reading of the remaining 4096 articles. During this stage, 22 works were selected to be read in full. However, one of them was subsequently excluded due to the unavailability of its full text.
The full-text version of each article was subjected to a “blind reading” carried out by two reviewers. In case of disagreement, two additional reviewers were consulted. Moreover, we sought to conduct an in-depth analysis to consolidate the employed search expressions. At this point, one article was excluded because it focused on medical errors. In contrast, six articles were excluded because they addressed missed nursing care in contexts other than emergency departments and intensive care units. Hence, the final sample consisted of 14 works. The entire selection process described above is shown in Figure 1.
2. Results
The obtained results are presented in Table 1, being organized according to title, author(s), year of publication, type of study, location(s), context, and findings.
Table 1 Results organized according to title, author(s), publication year, type of study, location(s), context, and findings.
| Title, Author(s) and Publication Year | Type of Study and Location(s) | Context | Findings |
|---|---|---|---|
| Missed nursing care in emergency departments: A scoping review (Duhalde et al., 2023) | Qualitative study (level of evidence: IVa) Australia, United States of America, Canada, Sweden, Brazil, Denmark, Ireland, Jordan, New Zealand, South Korea, Thailand, Netherlands and United Kingdom. | Emergency Departments | Missed Nursing Care: Assessment of vital signs; Pain control (patients with a 7-10 pain only received medication after 30 minutes); Increased waiting time for triage/reassessment after triage; Nurse-patient relationship (emotional support, interest and compassion); Provision of care/assistance as regards general hygiene, oral hygiene, or elimination; Documentation of pain assessment; Documentation of allergies; Documentation of intravenous access-related care; Basic care. Causes: Lack of space; Inadequate nurse-to-patient ratio; Prioritizing acute care over basic care; Care provision to patients who require more complex care may generate nursing care omissions in other patients; Nurses who manage various priorities, in addition to providing direct care, are more prone to practicing care omissions. Effects: Deterioration of the patient’s condition; Development of pressure ulcers; Treatment-related errors; Triage errors. |
| The relationship between missed nursing care and teamwork in emergency nurses: A predictive correlational study (Ghezeljeh et al., 2021) | Qualitative study (level of evidence: IV) Iran. | Emergency Departments | Mitigation Strategies: Teamwork; Effective team leadership; Implementing regulations, and creating a balance between salary and workload; Adequate planning and task distribution, and direct monitoring of individually assigned tasks; Leading by example. |
| The characteristics and factors associated with omitted nursing care in the intensive care unit: A cross-sectional study (Vincelette et al., 2023) | Qualitative study (level of evidence: IVb) Canada. | Intensive Care Units | Missed Nursing Care: Patient mobilization; Oral hygiene in orotracheally intubated patients; Documentation of the provided care. Effects: Worse perception of the provided care’s quality and safety; More adverse events. Mitigation Strategies: Creating a better work environment. |
| Healthcare-associated infections in adult intensive care units: A multisource study examining nurses’ safety attitudes, quality of care, missed care, and nurse staffing (Alanazi et al., 2023) | Qualitative study (level of evidence: IVb) Saudi Arabia. | Intensive Care Units | Effects: Higher incidence of healthcare-associated infections and ventilator-associated pneumonia. Mitigation Strategies: Increasing the number of nurses can minimize nursing care omissions, thus enhancing job satisfaction and reducing the incidence of healthcare-associated infections. |
| Monthly variation of unfinished nursing care at the US Army Burn Center (VanFosson et al., 2018) | Qualitative study (level of evidence: IVa) United States of America. | Intensive Care Units | Missed Nursing Care: Timely response to the patients’ requests; Documentation of nursing care/interventions; Intravenous access-related care; Emotional and psychological support; Patient education; Review of care documentation by the team; Review of care plans. Causes: Shifts carried out by part-time staff seem to enhance nursing care omissions; The part-timers’ need for support from the permanent staff can lead to an increase in nursing care omissions amongst the latter; Lack of time for care provision. |
| A Comparison of Nursing Activity Score Means for Missed Care Dimensions in Intensive Care Unit Patients (Mohammadi et al., 2023) | Qualitative study (level of evidence: IVb) Iran. | Intensive Care Units | Missed Nursing Care: Prevention of deep vein thrombosis; Assessment of blood circulation and skin condition, in the upper and lower limbs, at the restraint application sites; Checking ventilator parameters at the beginning of each shift; Changing the endotracheal tube’s position at least once during each shift; Verifying the endotracheal tube’s position, as well as its cuff pressure; Assessment of the patient’s state of consciousness; Hand hygiene, before and after physical contact with the patient; Assessment of oxygen saturation (SpO2); Assessment of gastric residual volume. Causes: Increased workload. Mitigation Strategies: Professional experience seems to be a preventive factor, as regards the practice of care omissions. |
| The Relationship between Nursing Job Satisfaction and Missed Nursing Care in Critical Care Units (Al-Mnaizel & Al-Zaru, 2023) | Qualitative study (level of evidence: IVb) Jordan. | Intensive Care Units | Missed Nursing Care: Altering the patient’s positioning every two hours; Oral hygiene; Patient education; Patient reassessments; Discharge planning. Causes: Absence/unavailability of the nurse in charge; Miscommunication with the medical team; Deficient transmission of information between shifts; Poor teamwork; Medication not available when needed; Unexpected increase in the number of patients, or sudden worsening of the patients’ health status; High admission/discharge rates. Mitigation Strategies: Enhancing job satisfaction; Offering the possibility of career progression, ensuring a supportive and respectful work environment, and acknowledging the team’s dedication and hard work; Improving work conditions, namely by admitting more nurses, guaranteeing immediate medication availability, and planning for unexpected increases in the number of patients, or sudden worsening of the patients’ health status; Implementing effective communication strategies. |
| Nursing Professional Commitment as a Mediator of the Relationship Between Work Environment and Missed Nursing Care Among Nurses: A Cross-Sectional Analysis (Hendy et al., 2024) | Qualitative study (level of evidence: IVb) Egypt. | Intensive Care Units | Causes: Night shifts; More years of professional experience; Increased patient-to-nurse ratio; Miscommunication and lack of human/material resources. Mitigation Strategies: A good work environment, strong professional ties, and continuous training on ethical values and nursing care, contribute to a reduction in nursing care omissions. |
| Omission of nursing care, professional practice environment and workload in intensive care units (Silva et al., 2020) | Qualitative study (level of evidence: IVb) Brazil. | Intensive Care Units | Missed Nursing Care: Ambulation three times a day; Planning and patient/family education for discharge; Airway suctioning; Care associated with intravenous accesses/infusions; Participation in multidisciplinary meetings, to review care plans. Causes: Lack of nurses; Sudden worsening of the patients’ health status; Unexpected rises in patient volume; Increases in the number of unstable patients; Deficient administrative/technical/auxiliary staff; Excessive workloads and a poor work environment contribute to the incomplete implementation of care plans. Mitigation Strategies: Ensuring an adequate number of professionals. |
| Effects of Work Environment on Quality of Care in ICUs: A Multisite Survey in China (Liu et al., 2016) | Qualitative study (level of evidence: IVb) China. | Intensive Care Units | Causes: Limited time; Lack of professionals. Mitigation Strategies: Good work environment; Adequate nurse-to-patient ratios. |
| The relationship between teamwork, moral sensitivity, and missed nursing care in intensive care unit nurses (Nobahar et al., 2023) | Qualitative study (level of evidence: IVb) Iran. | Intensive Care Units | Missed Nursing Care: Discharge planning and patient education. Mitigation Strategies: Teamwork; Moral sensitivity (includes respecting the patient’s independence, knowing how to communicate with the patient, dealing with ethical problems/conflicts, and applying moral principles during decision-making processes, while showing honesty, benevolence, and ample professional knowledge); Having older professionals in the team. |
| Rationing of Nursing Care in Intensive Care Units (Młynarska et al., 2020) | Qualitative study (level of evidence: IVb) Poland. | Intensive Care Units | Causes: Staff fatigue (physical, cognitive and psychosocial). |
| Effects of Work Environment on Quality of Care in ICUs: A Multisite Survey in China (Liu et al., 2019) | Qualitative study (level of evidence: IVb) China. | Intensive Care Units | Missed Nursing Care: Patient comforting; Patient/family education, to promote health. Causes: Limited time and resources. |
| Similarities and Differences in Nurse-Reported Care Rationing Between Critical Care, Surgical, and Medical Specialties (Higgs et al., 2020) | Qualitative study (level of evidence: IVb) Australia. | Emergency Departments and Intensive Care Units | Missed Nursing Care: Implementing fall prevention strategies; Providing assistance with elimination-related care (< 5 minutes); Offering emotional support to the patient/family; Ambulation three times a day; Altering the patient’s positioning every two hours; Oral hygiene; Feeding the patient while the food is still warm; Participating in multidisciplinary meetings about care plans. Mitigation Strategies: Experienced nurses recognize more nursing care omissions, frequently resorting to task delegation/supervision, namely as regards oral hygiene and feeding, which are often performed by other professionals (e.g., operational assistants). |
As can be observed, the 14 articles included in this review depict qualitative studies, conducted between 2016 and 2024. These works analyze data obtained in different locations (four studies gathered data from the Americas, two from Oceania, eight from Asia, two from Europe and one from Africa).
Of the 14 included articles, two focus specifically on missed nursing care in emergency departments, eleven concentrate on missed nursing care in intensive care units, and one addresses both contexts.
Most of the included studies exhibit a level of evidence IVb, which reflects the research’s qualitative nature (JBI Levels of Evidence and Grades of Recommendation Working Party, 2020).
Among the included works, nursing care omissions related to the previously identified context are identified in nine articles. Similarly, the associated causes are described in nine articles, while the associated effects are described in only three articles. Possible mitigation strategies are addressed in 10 articles.
To provide an answer to the research question, “What is the current knowledge on missed nursing care common to emergency and intensive care settings?” it is necessary to individually look at the previously mentioned subthemes.
When it comes to nursing care omissions common to both settings, we were able to identify eight care components mainly related to direct patient care, leading us to provide an answer to the first subtheme.
Regarding the causes of missed nursing care, we found four common topics mainly related to the volume of work, providing an answer to the second subtheme.
Due to the lack of evidence related to the common effects of missed nursing care, we were unable to provide an answer to the third subtheme.
Concerning mitigation strategies, scarce evidence was found, which did not allow us to answer unequivocally to the respective subtheme.
3. Discussion
Due to various causal factors, multiple components of nursing care are often significantly delayed or even not executed at all. Such omissions, in themselves, can affect the provided care’s quality and safety (Nantsupawat et al., 2022).
The 14 works included in this review not only identify the main care omissions that occur in emergency departments and intensive care units but also explore their causes and effects while suggesting strategies to minimize their incidence. Nonetheless, the studies in question refer to a variety of services, provide a wide range of data, and appear to be unrelated until they are viewed in the light of the research questions, seeking a hidden connection. Hence, despite the studies’ distinct approaches/findings, we were able to discover common points that allowed answering some of the aforesaid questions.
The omission of nursing care within the studied contexts affects several care components, such as feeding the patient while the food is still warm (Higgs et al., 2020), establishing a positive nurse-patient relationship (characterized by emotional support, interest, and compassion) (Duhalde et al., 2023), and ensuring adequate planning, as well as patient/family education, for discharge (Silva et al., 2020). As regards missed nursing care common to emergency departments and intensive care units, we identified various affected elements, namely:
The nurse-patient relationship (which should comprise emotional support, interest and compassion) (Duhalde et al., 2023; Higgs et al., 2020; Liu et al., 2019; VanFosson et al., 2018);
Oral hygiene and elimination-related care (Al-Mnaizel & Al-Zaru, 2023; Duhalde et al., 2023; Higgs et al., 2020; VanFosson et al., 2018; Vincelette et al., 2023);
Basic care (Duhalde et al., 2023; Higgs et al., 2020);
Patient mobilization/positioning (Al-Mnaizel & Al-Zaru, 2023; Higgs et al., 2020; Vincelette et al., 2023);
Ambulation three times a day (Higgs et al., 2020; Silva et al., 2020);
Documentation of the provided care (Duhalde et al., 2023; VanFosson et al., 2018; Vincelette et al., 2023);
Care associated with intravenous accesses/infusions (Silva et al., 2020; VanFosson et al., 2018);
Participation in multidisciplinary meetings about care plans (Higgs et al., 2020; Silva et al., 2020).
Moreover, by analyzing the obtained results, we were able to recognize numerous causal factors that contributed to the omission of nursing care, being mostly related to management issues (regarding care procedures and human/material resources), miscommunication between teams/professionals, and an unfavorable work environment (Al-Mnaizel & Al-Zaru, 2023; Duhalde et al., 2023; Liu et al., 2019; Silva et al., 2020).
As to the causes of missed nursing care common to intensive care and emergency departments, we identified the following aspects:
Excessive workloads (Duhalde et al., 2023; Mohammadi et al., 2023; Silva et al., 2020);
Unexpected increases in the number of patients or sudden worsening of the patient's health status (Al-Mnaizel & Al-Zaru, 2023; Duhalde et al., 2023; Silva et al., 2020);
Increased patient-to-nurse ratios (Duhalde et al., 2023; Hendy et al., 2024);
Lack of nurses (Silva et al., 2020).
It is important to acknowledge how emergency department reality has changed, specifically when it comes to the increase in the length of stay (Amritzer et al., 2024) and how well-equipped the departments are to handle the constantly shifting nurse-to-patient ratio.
With respect to consequences, we were able to discover several negative effects of nursing care omissions in emergency departments, such as the deterioration of the patient’s condition, the development of pressure ulcers, treatment-related errors, and triage errors (Duhalde et al., 2023). On the other hand, in intensive care units, missed nursing care increased the number of adverse events and resulted in worse perceptions regarding care quality and safety (Vincelette et al., 2023). Furthermore, it raised the incidence of healthcare-associated infections and ventilator-associated pneumonia (Alanazi et al., 2023).
In this category, it was not possible to establish common points between the two environments since we found scarce evidence on the consequences of nursing care omissions in such settings. Nonetheless, we can identify various negative outcomes that could easily occur in both types of settings while seeking to adopt preventive strategies. For instance, hospitalization in emergency departments can be associated with the development of pressure ulcers due to prolonged positioning on hard surfaces, stretchers, etc. (Santamaria et al., 2019). This phenomenon could also be observed in intensive care units since patient mobilization is one of the care components recognized as deficient in that particular context (Vincelette et al., 2023).
Having identified the nursing care omissions common to the studied environments, as well as their possible causes, it was equally important to identify the shared mitigation strategies in order to hinder the occurrence of adverse events.
Concerning emergency departments, the available literature mentions several mitigation strategies, namely teamwork, effective team leadership, implementing regulations, creating a balance between salary and workload, adequate planning and task distribution, direct monitoring of individually assigned tasks, and leading by example (Ghezeljeh et al., 2021). In this sense, the advantages of employing experienced nurses were also mentioned since such professionals have the ability to detect more nursing care omissions (Higgs et al., 2020; Mohammadi et al., 2023).
Likewise, as regards intensive care units, the included studies describe numerous mitigation strategies, often highlighting the importance of a good work environment (Al-Mnaizel & Al-Zaru, 2023; Hendy et al., 2024; Liu et al., 2016; Vincelette et al., 2023). In these circumstances, the presence of more nurses can ensure suitable volumes of professionals, as well as adequate nurse-to-patient ratios, thus contributing to the minimization of missed nursing care (which, in turn, increases job satisfaction while reducing the incidence of healthcare-associated infections) (Alanazi et al., 2023; Al-Mnaizel & Al-Zaru, 2023; Liu et al., 2016; Silva et al., 2020).
Enhancing job satisfaction is one of the key measures applied in intensive care units, as well as offering the possibility of career progression, acknowledging the team’s dedication and hard work, guaranteeing immediate medication availability, planning for unexpected increases in the number of patients/sudden worsening of the patient’s health status, and implementing effective communication strategies (Al-Mnaizel & Al-Zaru, 2023). The significance of strong professional ties, together with continuous training on ethical values and nursing care, is also recognized (Hendy et al., 2024).
In the abovementioned setting, there are other relevant aspects that mitigate missed nursing care, such as teamwork, moral sensitivity (including respecting the patient’s independence, knowing how to communicate with the patient, dealing with ethical problems/conflicts, and applying moral principles during decision-making processes, while showing honesty, benevolence, and ample professional knowledge); and the existence of older elements within the team (Nobahar et al., 2023).
After analyzing the obtained evidence on mitigation strategies for missed nursing care, only teamwork and experienced/older team elements seem to be common in the studied environments. Thus, we were not able to answer unequivocally to the respective research question.
Limitations
Notwithstanding its relevant findings, this scoping review presents several limitations.
Firstly, we only considered articles with free access to their full-text version, not purchasing access to other pertinent works.
Secondly, the employed search terms/expressions may have restricted the number of obtained results since, in the final sample, there was a substantial disparity as regards the quantity of included articles per context (only three works addressed the studied issue in emergency departments, while 12 works addressed the studied issue in intensive care units). Furthermore, the number of obtained results may have been limited by the search terminology used to explore the subject of missed nursing care. Nevertheless, the definition of specific terms/expressions applied in both contexts, together with the information available in gray literature, facilitated the articles’ selection and analysis.
Lastly, the analyzed studies present a lack of evidence as regards missed nursing care effects and limited evidence with respect to mitigation strategies common to both contexts, which hinders us from answering unequivocally some of the research questions.
Conclusion
Missed nursing care is often used as an indicator of the quality of care provided. This study allowed us to map the available scientific evidence on missed nursing care common to the emergency department and intensive care unit, providing answers to some of the previously established research questions and revealing the main nursing care omissions common to both settings, as well as their causes. Nonetheless, it presents limitations, namely related to the scarce available evidence, as substantial shared effects/mitigation strategies were not detected. Accordingly, there is a clear need for further research on missed nursing care in the abovementioned context.
In this sense, it is crucial to develop additional studies on nursing care omissions, their causes, their effects, and possible mitigation strategies in emergency departments and intensive care units. The need to produce more scientific knowledge is particularly noticeable in the case of emergency departments since only three of the 14 included studies addressed this setting. Regarding the effects of missed nursing care in this setting, it is striking how scarce the evidence is, leading us to believe that the knowledge about mitigation strategies could also be improved if more evidence in primary studies were to be produced. One of the aspects that may affect missed nursing care in emergency departments is the high influx of patients as well as their increased length of stay in this department; both variables have not been acknowledged in the previously found evidence.
Moreover, besides examining each context individually, shared aspects should also be investigated, as both settings receive critically ill patients who require highly complex care.
They equally involve teamwork when treating a critically ill patient, and in several studies, this concept is identified as having an impact on the mitigation of missed nursing care. When it comes to job satisfaction, it is mentioned as having a high impact on intensive care units, and even though this concept is not directly approached in emergency departments, the balance between salary and workload, adequate planning, and task distribution, amongst other topics, all contribute to improving professional satisfaction. Considering this fact, developing future research surrounding the creation of strategies to improve professional satisfaction and optimization of teamwork and its relation to missed nursing care would pose as a valuable approach to this topic.
As previously mentioned, patients are often transferred from emergency departments to intensive care units, which leads us to believe that an interesting approach would be to improve the transfer procedures as well as the teamwork between both settings, thus mitigating missed nursing care by reducing the loss of patient-related information.
When dealing with critically ill patients in diverse contexts, the scarcity of scientific evidence on missed nursing care significantly hampers care management, also hindering the implementation of quality/safety-promoting strategies. Hence, this specific field of knowledge is of utmost importance for an effective, high-quality, and safe nursing practice.
Author’s contribution
Conceptualization, F.J., M.C., T.S.A. and P.P.S.; data curation, F.J. and M.C.; formal analysis, F.J., M.C., T.S.A. and P.P.S.; investigation, F.J., M.C., T.S.A. and P.P.S.; methodology, F.J., M.C., T.S.A. and P.P.S.; project administration, F.J. and M.C.; resources, F.J., M.C., T.S.A. and P.P.S.; software, F.J. and M.C.; supervision, T.S.A. and P.P.S.; validation, T.S.A. and P.P.S.; visualization, F.J. and M.C.; writing-original draft, F.J. and M.C.; writing-review and editing, F.J., M.C., T.S.A. and P.P.S.

